











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Smoking is one of the leading causes of morbidity and mortality. According to the World Health Organization (WHO), tobacco consumption is the leading cause of death from non-communicable diseases, such as heart disease, lung disease and cancer. 1 Global figures show that tobacco consumption causes more than 7 million deaths each year, of which more than 6 million are smokers and about 890 000 are non-smokers exposed to second-hand smoke. Almost 80% of more than 1 billion smokers in the world live in low- or middle-income countries. 2 In Argentina, more than 44 500 people die annually from smoking-related diseases and these deaths represent 13.2% of all deaths occurring in people older than 35 years, mainly due to cardiovascular diseases, chronic obstructive pulmonary disease (COPD) and lung cancer. 3 Based on the evidence from a large number of studies on the effects of tobacco consumption, several methods have been proposed to measure it and estimate the burden of disease. In our country, four National Surveys on Risk Factors (Encuestas Nacionales sobre Factores de Riesgo, ENFR) have been performed in 2005, 2009, 2013 and 2018, in which, among other aspects, tobacco consumption has been measured based on the population's statements about their status as smokers, non-smokers or ex-smokers. 4-7 Since 1980, the impact estimate of different risk factors on population mortality by applying epidemiological methods has become frequent in Anglo-Saxon countries, mainly in the United States. To estimate mortality attributable to different risk factors, several methods are available, which vary in terms of both data required and acceptance of assumptions. These methods are mainly based on the concept of the population attributable fraction, that is, the percentage of cases that could be prevented if exposure to the risk factor under study was removed. To estimate mortality attributed to tobacco consumption, different calculation processes are identified, 8 which may be classified according to whether they are dependent or independent of smoking prevalence, that is, whether or not smoking prevalence is used to estimate the mortality burden. The application of a prevalence-based method to estimate attributed mortality is based on prior knowledge of the number of smokers, ex-smokers and non-smokers in the population. These data derive from the four ENFRs. The present work aims to show the burden of mortality due to tobacco consumption in the Province of Buenos Aires in the survey periods of the four ENFRs.
METHODS
Mortality attributable to tobacco consumption was calculated by using a prevalence-based method and assuming the risks associated with tobacco consumption according to the Cancer Prevention Study II (CPSII). 9 Two data sources were available for its implementation:
1. Calculation of the prevalence of tobacco consumption: smokers, ex-smokers and non-smokers for men and women by risk age groups: 35-64 years old and 65 years or older. The data sources were the ENFR microdata bases: 2005/2009/2013/2018 from the Instituto Nacional de Estadística y Censos (INDEC; the National Institute of Statistics and Censuses in Argentina). 7
2. Table of observed mortality by age group and sex according to the cause of death. The database was that containing overall mortality data from 2005 to 2018 reported by the Dirección Provincial de Estadísticas de la Salud (DIS; Provincial Department of Health Statistics) of the Province of Buenos Aires.
Statistical analysis
1. Prevalence of tobacco consumption: the microdata bases of the ENFRs were exported to SPSS (Statistical Package for the Social Sciences) and the prevalences were calculated by the survey year and by risk groups (age and sex). The results published by the INDEC for each ENFR served as control, so that, the overall estimates should be consistent with those published. Point values and confidence intervals were calculated for complex samples by using the weighting factors provided by the database.
2. Observed mortality: DIS’s databases were exported to SPSS and deaths by smoking-related cause were calculated according to the risk group (age and sex). The calculation was performed using the following formula:
AM = OM*FAP, where PAF =
[p0 + p1RR1 + p2RR2]-1 / [p0 + p1RR1 + p2RR2]
AM means attributable mortality; OM, observed mortality (number of deaths by cause, age and sex); PAF, population attributable fraction; p0, p1, and p2 represent the prevalence of non-smokers, smokers and ex-smokers, respectively; RR1 and RR2 represent the relative risk in smokers and ex-smokers, respectively. Each p value was calculated for each ENFR adjusted for age group and sex.
Variables: 1-Risk groups: Age of 35-64 years and 65 years or older. These categories are established in the CP SII. 2-Tobacco consumption: The document used was that published by the INDEC for the management of the ENFR databases. It classifies tobacco consumption variable into three categories: smoker, ex-smoker, and non-smoker. 3- Cause of death: It was classified according to the International Classification of Diseases (ICD)-10th Revision. Individual data on age, sex and cause of death were assigned for each of the diseases in the CPSII model. Deaths and tobacco consumption prevalences were grouped into four periods equivalent to each ENFR. The CPSII attributable fractions were applied considering those cut-off points. Similarly, specific mortality rates were calculated by risk age group and sex for the total of each set of diseases associated with tobacco consumption: tumours, cardiovascular and respiratory diseases, from the list of tobacco-attributable causes according to the model. The population used as denominator to estimate the overall death rates was based on the demographic projections for the Province of Buenos Aires published by the DIS. This led to observe the evolution of the raw death rates by age group and sex for each annual period evaluated. The statistical softwares Epi Dat 4.2 and SPSS 20 were used.
RESULTS
In Table 1, the prevalences of tobacco consumption by sex and age according to each one of the four ENFR estimates are shown. In Tables 2 to 5, absolute deaths and attributable mortality fractions by cause and groupings in persons aged 35 years or older are shown. Overall, there was a decrease in smoking prevalence from 29.5% in 2005 to 23.1% in 2018 (absolute reduction of 6.4%, and percentage reduction of 21.7%). The prevalence of ex-smokers increased from 17.2% in 2005 to 17.7% in 2018; expressed in inhabitants, from 1 673 861 to 1 925 674 (251 813 more). There were 223 925 deaths recorded within the 19 smoking-related causes, 51 890 (23.1%) of which were attributed to smoking. Of these, 36 690 (70%) were men and 15 200 (30%) were women.

Table 1 Prevalence of tobacco consumption (%) as per the ENFRs performed in the Province of Buenos Aires

Table 2 Mortality attributable to tobacco consumption in males aged 35-64 years. Province of Buenos Aires. ENFR series: 2005, 2009, 2013, 2018

Table 3 Mortality attributable to tobacco consumption in females aged 35-64 years. Province of Buenos Aires. ENFR series: 2005, 2009, 2013, 2018

Table 4 Mortality attributable to tobacco consumption in males aged >64 years. Province of Buenos Aires. ENFR series: 2005, 2009, 2013, 2018
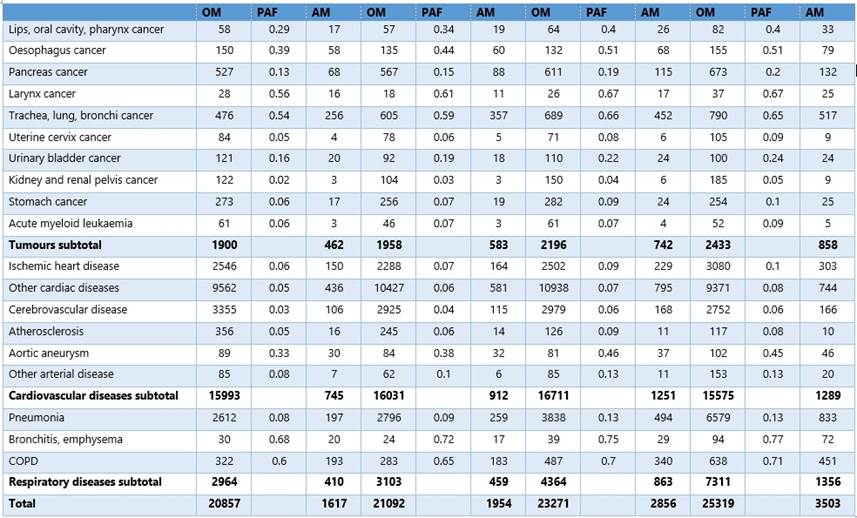
Table 5 Mortality attributable to tobacco consumption in females aged >64 years. Province of Buenos Aires. ENFR series: 2005, 2009, 2013, 2018
The leading cause of death from smoking-related tumours included trachea, lung and bronchi cancer. Among men aged 35-64 years, 90% of tumours were attributed to tobacco; 3688 out of 4090 deaths in the four years analysed were attributed to smoking. As regards laryngeal cancer, 431 out of 507 deaths in the four years analysed were attributed to smoking. In men aged 35-64 years, overall cardiovascular diseases represented 18 255 deaths, 6293 of which were attributed to tobacco consumption (34%). In the case of respiratory diseases in men aged 35-64 years, 1462 out of the 3653 deaths were attributed to tobacco consumption (40%), and in the case of smoking-attributable pneumonia, 673 out of 2696 deaths were attributed to tobacco consumption (24.9%). In this age group and sex, COPD has not modified its incidence or death rates or its attributable fraction. Out of 878 cumulative deaths, 718 (81.7%) were attributed to tobacco consumption. In men older than 64 years, there is a trend towards a reduction in mortality attributable to all smoking-related tumours. Lung, trachea and bronchi cancer produced 6319 deaths in the four cumulative years, 5417 of which were attributed to smoking (85%). Regarding laryngeal cancer, the second tumour with the second highest attributable fraction, 572 out of 717 cumulative deaths were attributed to smoking (79.5%). In the group of cardiovascular diseases in men older than 64 years, 8166 out of 55 114 cumulative deaths were attributed to smoking (14.8%). The largest fraction attributable to smoking was that of aortic aneurysm: 680 out of 1132 deaths (60%). In absolute terms, the highest mortality was observed in the group of other cardiac diseases with accounting for 31230 deaths, 4951 of which were attributed to smoking (15.9%). In the case of respiratory diseases, 5806 out of 17 446 deaths in men older than 64 years were caused by tobacco consumption (33.2%).
In women aged 35-64 years, there was a cumulative total of 4817 deaths from smoking-related tumours in the four years analysed, 2148 of which were directly attributed to smoking (45%). Laryn geal cancer presented the highest PAF: 57 out of 72 deaths in the four years analysed could have been prevented with smoking control. Trachea, lung and bronchi cancer represented 1748 deaths, 1379 of which were attributed to tobacco consumption. Oesophagus tumours and lip and oral cavity cancer presented PAFs near 60%. Smoking-attributable mortality due to heart disease showed a decrease from 2005 (29.1 per 100 000) to 2018 (18.7 per 100 000), a 35.5% reduction. In total, there were 8008 deaths from cardiovascular causes in women aged 35-64 years during the four cumulative years, 2310 of which were attributed to smoking (28%). Cerebrovascular disease shows the highest attributable fraction: 47% (1042 out of 2212 cumulative deaths were attributed to smoking). This was followed by ischemic heart disease (1704 deaths in the four years, 38.2% attributed to smoking). Although the group of other cardiac diseases produced a greater number of deaths, only 13.7% out of 3946 cumulative deaths in the four years analysed were attributed to smoking. As regards smoking-related respiratory diseases in women aged 35-64 years, 37.4% out of 2167 deaths were attributed to smoking. Women aged 65 years or older were the group with the highest increase in tobacco consumption in the Province of Buenos Aires. Among them, death rate resulting from smoking-related tumours has increased concomitantly. If we consider the rates of all smoking-related tumours and we focus exclusively on smoking-attributable death rates, the increased from 49.9 per 100 000 in 2005 to 75.9 per 100 000 in 2018. Out of 8487 deaths from cancer in women aged 65 years or older accumulated in the four years analysed, 2644 were attributed to smoking (31%). Lung, trachea and bronchi cancer resulted in 2560 deaths in women aged 65 years or older in the four years analysed, 1582 attributed to smok ing (62%). Death rate resulting from these tumours increased from 51.4 per 100 000 in 2005 to 69.9 per 100 000 in 2018. In the case of lip and oral cavity cancer, there were 261 deaths, 36.3% attributable to smoking. Cardiovascular diseases in women aged 65 years or older represented 64 310 deaths, 4195 attributable to smoking (3.7%).
DISCUSSION
The presumption that tobacco consumption was a risk factor for health emerged in 1920. It was only until 1980 that the grounds for estimating the smoking impact on mortality were made explicit by means of epidemiological methods. 8,10 CPSII is a cohort study conducted by the American Cancer Society which began in September of 1982. 9 CPSII limits the causes of death attributable to smoking to 19 and identifies them under the heading "established causal relationship". Estimation of attributed mortality using a prevalence-based method is the simplest calculation procedure in terms of data availability. This method, the most widely used in the scientific literature to estimate tobacco-attributable mortality, which has been implemented in the CDC's SAMMEC (Smoking Attributable Mortality Morbidity and Economic Cost) software, is commonly used for the serial estimation of tobacco-attributable mortality in the United States, and its use is widely spread. 11,12 To properly estimate and use modelling, it is necessary to know the excess risk of death of those exposed (smokers and/or ex-smokers), data that may be collected from a cohort study. 13 In 2008, the WHO adopted a set of practical and cost-effective measures to strengthen the implementation of the main provisions on demand reduction under the WHO Framework Convention on Tobacco Control (WHO FCTC): the MPOWER measures. Each measure corresponds to at least one provision of the WHO FCTC. 1,2 The six MPOWER measures are the following: •To monitor the consumption of tobacco and the prevention measures. •To protect population from tobacco smoke. •To offer help to people to quit smoking. •To warn of dangers associated with smoking. •To enforce prohibitions on advertising, promotion and sponsorship. •To increase tobacco taxes. It is necessary to strengthen these and other promotion and prevention measures in order to reduce exposure to tobacco. If tobacco consumption could be reduced to zero (obviously an unrealistic but ideal scenario), 19 756 deaths due to tobacco-related tumours, 20 966 deaths related to cardiovascular causes and 11 168 deaths related to pneumonia, bronchitis and COPD would have been avoided in the province of Buenos Aires; in other words, 51 890 deaths occurred in the four years analysed. This represents 23.1% of the total 223 925 deaths derived from the 19 causes attributable to tobacco consumption. In contrast to the analysis focused exclusively on adjusted death rates, smoking-attributable mortality indicates the magnitude of the risk factor burden on mortality. 14,15 The PAF magnitude of death due to tobacco consumption continues being a challenge for public health, mainly because of the burden of disease and the demand on health services. 16 Particularly, in America, the estimates of healthcare costs have yielded 33 billion dollars directly, which is equivalent to 0.7% of the Gross Domestic Product of the region. 17 Similarly, tax burden on tobacco industry does not directly cover healthcare costs, which in Argentina have been calculated at 37%. Although the studies are not numerous, they have estimated the burden of attributable mortality in the country (as in the Province of Tucumán) 18 showing that 4.1% of deaths could be attributed to smoking, which is lower than the data recently reported for Argentina (14%). 3 It is necessary to measure the magnitude of the situation by considering the percentage of reduction that could be expected not only for the total number of deaths, but specifically for the causes associated with tobacco consumption, because there, the burden of smoking is clearly more significant. 19,20
CONCLUSIONS
Prevalence studies like this have important limitations: they assume the risks linearly as weighting factors of a population group, whereas covariables are completely unknown. Similarly, other epidemiological weighting factors are left outside the estimates. The ENFRs have weaknesses since the measurement of habits are self-reported. Nevertheless, in many cases, they are the only potential large models to estimate the burden of disease from recognized risk factors. Mortality attributable to smoking remains high and is unacceptable because there are concrete possibilities for its reduction. It is necessary to further strengthen measures to reduce exposure to tobacco.

