











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkKEY POINTS
Current knowledge
• Transverse carpal ligament involves carpal tunnel and Guyon’s canal
• Historically, open carpal tunnel release decompresses Guyon’s canal
Contribution of the article to current knowledge
• Endoscopic carpal tunnel release correlates with anato my foundation regarding transverse carpal ligament
• Endoscopic or open carpal tunnel release decompress Guyon’s canal
Carpal tunnel syndrome (CTS) is the most common peripheral nerve entrapment syndrome, estimated to occur in 3.8% of the general population1,2. When conservative treatments fail, surgical intervention is recommended. Both open and endoscopic carpal tunnel release (CTR) techniques are well established3,4. The carpal tunnel and Guyon’s canal are connected anatomically via the transverse carpal ligament5. Previous literature has dem onstrated that CTR decreases pressure in Guyon’s canal, whether performed with open or endoscopic techniques6,7. Following open CTR, patient-reported outcomes improve with regards to ulnar nerve symptoms8,9 and two-point discrimination improves in the ulnar nerve distribution8. Additionally, the cross-sectional area of the ulnar nerve has been shown to increase in size following CTR10,11. Also, sensory conduction has been shown to improve for the ulnar nerve following open carpal tunnel release on nerve conduction studies12. In general, symptoms related to the CTS are known to be worse among the diabetic population13,14, however, there have been no significant differences in safety and outcomes compared to the non-diabetic population15.
Endoscopic carpal tunnel surgery became a widely used and accepted technique in the last two decades, promising early recovery and less pain without any inferior outcomes16-20. To our knowledge, there has not been ob jective evidence reported regarding symptomatic improve ment in ulnar nerve pathology following endoscopic CTR. Based on the current available literature, we hypothesize that endoscopic CTR improves static two-point discrimi nation in both the median and ulnar nerve distributions following surgery. Furthermore, we hypothesize that these changes are apparent in both diabetic and non-diabetic populations.
Materials and methods
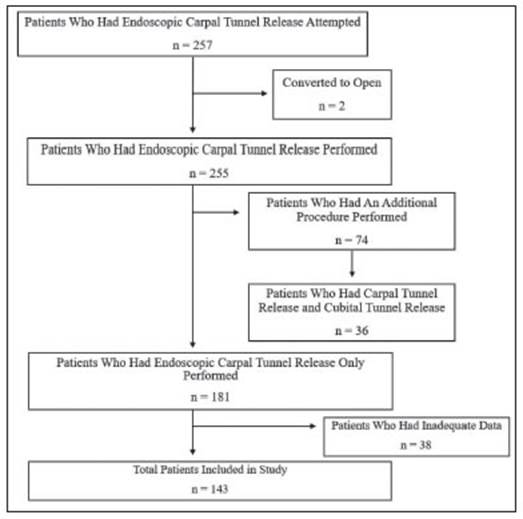
Colorado Multiple Institutional Review Board (COMIRB) ap proval was obtained (protocol 16-2566). All patients who un derwent endoscopic CTR at one community hospital, Denver Health, Colorado, USA with the senior surgeon, Dr. Banegas, from April 2016 to June 2019 were reviewed retrospectively with a waiver of informed consent. Included patients under went endoscopic CTR as their only hand surgery procedure and had preand one month post-operative clinic visits with documented two-point discrimination in the ulnar and median nerve distributions. If there was any significant two-point dis crimination ulnar territory sensory loss, or no clear correlation of two-point discrimination exam with patient’s symptoms, an EMG was performed to diagnose or rule out cubital tunnel syndrome (CuTS). Patients with recurrent CTS or concomitant CuTS and undergoing cubital tunnel release (CuTR), were separated from the main patient population pool. Those with inadequate post-operative data or follow-up, or who needed to be converted to open CTR were all excluded (Fig. 1).
All endoscopic procedures were performed using the stan dard described single portal technique with the CenterlineTM (Arthrex Inc., Naples, FL) endoscopic carpal tunnel system. Two-point discrimination was measured with Semmes-Wein stein Monofilament test and documented by the senior author, Dr. Banegas, with a standard static two-point discrimination wheel in one millimeter (mm) increments pre-operatively and at one month post-operative follow up visit. Significant diminished sensation was defined as the mean two-point discrimination measurement being greater than 6 millimeters (mm) in the median and/or ulnar nerve territory21-24.
Student’s t-test was used to analyze the effects of age, sex, and diabetes mellitus (DM) in the ulnar and median nerve ter ritories with two-point discrimination tests. One-way analysis of variance (ANOVA) was used to test for differences in two-point discrimination among patient’s based on their smoking status.
Results
A total of 143 patients with complete preand post-operative two-point discrimination data were identified during the study time period. There were 100 female and 43 male, with mean age of 48.5 and 50.1, respectively. Patient demographics data revealed that 25.9% of patients were active smokers and 31.5% had DM (Table 1).

Two-point discrimination in the median nerve distribu tion improved after surgery by an average of 3.3 ± 2.7 mm (mean difference 7.7 vs 4.4 mm, p < 0.001). In addition, 136 patients had over 2 mm two-point discrimination exam results in the ulnar nerve territory, although there was no evidence of CuTS in pre-operative nerve conduction study reports. When two-point discrimination was compared before and after endoscopic CTR surgery, there was also a significant difference in the ulnar nerve territory (mean difference 5.7 vs 4.1 mm, p < 0.001) (Table 2).

When age was continuously analysed using the Pearson correlation coefficient test, there were no linear relationships between aging and two-point discrimination outcomes in both the median and ulnar nerve territories. Furthermore, when a statistical comparison was conduct ed based on gender, DM, and smoking status, there were no statistically meaningful differences, as well (Table 2).
The overall average surgical time was 46.1 minutes, including time between patient presentation to the opera tive room and transfer to the post-anaesthesia care unit.
Average procedure time was 18.4 minutes, and average tourniquet time was 10.5 minutes. Patients were placed in a soft dressing for 5 days after the surgery. After taking down the dressing, they were advised to continue their daily activities, as tolerated. No one required any narcotic prescriptions. Average follow up time was 11.8 months (range 4 to 17 months). There was only one complication reported, which was a surgical site infection who was an active smoker and responded well to a 5-day course of oral antibiotic treatment. When documented, it was found that all patients were able to return their normal activity levels in less than 3 weeks following surgery.
In addition to these findings, we identified 36 other patients who underwent CuTR simultaneously with CTR, based on the nerve conduction study results. Twenty-eight of these had diminished ulnar two-point discrimina tion tests. When we compared two-point discrimination improvements in the ulnar nerve territory between CTR only and CTR + CuTR groups, the CuTR group had worse pre-operative values (9.2 ± 3.6 mm vs. 5.7 ± 1.4) and greater improvements compared to the CTR only group (mean of preand post-operative difference 5.1 vs 3.4 mm, p = 0.001).
Discussion
CTR is a safe procedure with high patient satisfaction outcomes25-30. Silver et al8 demonstrated anatomic sup port for the concept that release of the transverse carpal tunnel ligament decompresses both the carpal tunnel and Guyon’s canal. Authors also showed that patient-reported outcomes and two-point discrimination, with regards to ulnar nerve symptoms, showed improvement following open CTR alone. This study aimed to evaluate whether these findings were present in a population undergoing endoscopic CTR, while providing objective data, by utiliz ing a preand post-operative two-point discrimination test.
In general, patients in this study showed demonstrable evidence of improved two-point discrimination in both the ulnar and median nerve distributions following endoscopic CTR. It can be inferred that the ulnar nerve changes are due to an indirect release of Guyon’s canal, as described with the open procedure. This study supports the idea that compression across the ulnar nerve at Guyon’s canal is present in a certain portion of patients with CTS. We also noted that with concomitant EMG-confirmed CuTS, the two-point discrimination measurements were significantly greater in the ulnar nerve territory. As such, releasing the cubital tunnel subsequently improved the two-point discrimination more prominently than in the carpal tunnel only group.
This study has limitations. The retrospective nature of the study precluded any observational bias. Also, the preand post-operative two-point discrimination measure ments may be a subjective test, but it was standardized and consistently performed by the same experienced clinician with a single instrument in each case. Hence, increasing the sensitivity and accuracy of the test. Lastly, continued longitudinal follow-up evaluations of patients’ two-point discrimination would be of benefit in determining any temporal effects on post-operative changes.
In conclusion, the results of this study support that endoscopic CTR can be an effective means of decom pression for both the median and ulnar nerve at the wrist.

