











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkDyskeratosis congenita (DC) is a rare hereditary disease caused by a defect in the maintenance of the telomeres, causing premature telomere shortening and subsequent replicative senescence, leading to premature stem cell exhaustion1. It has been originally described as skin pigmentation, nail dystrophy and leucoplakia2. Bone marrow failure (BMF) was later described and it is the main cause of mortality in part due to infections by opportunistic pathogens3. Moreover, patients with DC have a great cumulative risk for developing malignant tumors witch can affect almost every tissue1. Treatment is mainly of the complications, and it includes androgen therapy and al logeneic hematopoietic stem cell transplantation for BMF.
Actinomycotic cerebral abscess, are a rare form of infective disease caused by anaerobic Gram-positive bacteria of the Actinomyces spp. which is commensal flora of the oral cavity as well as the digestive and urinary tract4anaerobic Gram-positive bacteria that normally colo nize the human mouth and digestive and genital tracts. Physicians must be aware of typical clinical presentations, such as cervicofacial actinomycosis following dental focus of infection, pelvic actinomycosis in women with an intra uterine device, and pulmonary actinomycosis in smokers with poor dental hygiene. They are highly susceptible to beta-lactams.
We present the case of a 32-year-old man with right brachiocrural palsy, aphasia and uncommon mucocuta neus features.
Clinical case
A 32-year-old man with one-month history of progressive right brachiocrural palsy and aphasia presented to the emergency department. MRI of the brain showed multiple contrast-en hanced lesions (Fig. 1). Clinical examination showed uncom mon dermatological features, including: skin pigmentation (Fig. 2A), nail dystrophy (Fig. 2B), leukoplakia (Fig. 2C), alopecia, blepharitis and missing teeth. Laboratory studies showed a white-cell count of 2900/mm3, a hemoglobin level of 9.7 mg/dl and a platelet count of 50 000/mm3. Human immunodeficiency virus test was negative and CD4 count was 72/mm3.
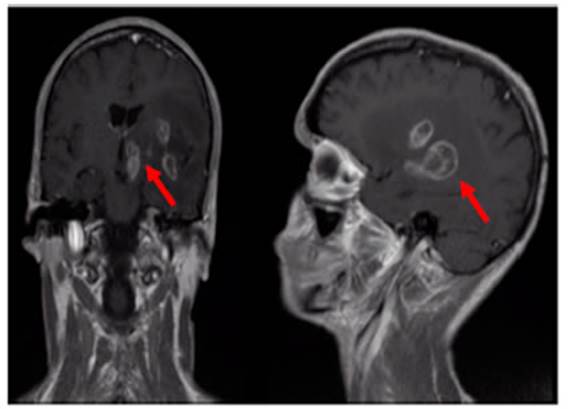

Fig. 2 Skin pigmentation (A), nail dystrophy (B), leukoplakia (C), lichen-like skin lesions which followed Blaschko’s lines of the patient’s mother (D)
The patient had two siblings, a brother with similar derma tological findings and diagnosis of bone marrow aplasia and a healthy sister. Clinical findings and a family history resembling X-linked inheritance was consistent with dyskeratosis congenita. Dermatological exam was done to the patient’s mother. Lichen-like skin lesions which followed Blaschko’s lines (Fig. 2D) were observed, compatible with cutaneous mosaicism, which clinically confirms that the mother carried a genetic mutation compatible with the ones found in DC. Biopsy of the brain lesions showed infection by Actinomyces viscosus. After two months of treatment with ampicillin the patient showed a partial recovery. Leucopenia, anemia and thrombocytopenia persisted.
The patient was initially discharged with mild right-side palsy and moderate aphasia. One month later, he presented to the emergency department with fever and dyspnea, he was hospitalized with diagnosis of severe pneumonia which caused his death.
Discussion
Infections caused by actinomyces are typically but not exclusively seen in patients with inmunosupresion5. Moreover, cervicofacial actinomycosis has been reported in patients with dental procedures or poor dental health6. In this case, a rare genetic disorder which combines im munodeficiency due to bone marrow failure and loose teeth, has been the background for an invasive infection, caused by Actinomyces viscosus.
Interrogation for similar features in other family mem bers, was a key approach for the final diagnosis. In this case, only male members were affected, consistent with X-linked inheritance, which was confirmed by the finding of signs of genetic mosaic in the mother. X-linked, autosomal recessive and autosomal dominant are the three ways of inheritance described in DC, with multiple genes involved1.
As BMF is the main cause of death in patients with DC, allogenic hematopoietic stem cell transplantation could offer a curative approach, however, DC patients have a greater mortality when compared to patients with other causes for BMF, probably due to more lung and liver complications7. Moreover, androgen therapy has shown to be effective in treating bone marrow failure in a small group of patients with DC8. Adverse effects of both ap proaches should be carefully considered in this scenario.
On the other hand, surveillance for possible neoplasms could prevent advanced stage disease, meaning the possibility of oncologic curative treatment. A good dental health could diminish the risk of invasive infections due to oral cavity pathogens. Hence, despite being and untreat able disease, prompt diagnosis and close surveillance could prevent or delay severe complications as the one of our case. Unfortunately, in this case, despite a clear family history of a systemic disorder, the patient and his family didn’t have a diagnosis consistent with DC prior to consultation at our institution, probably due to the fact that they live in a rural area with limited access to medical care.

