











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkKEY POINTS
Actual knowledge
• The global rates of endophthalmitis ranges between 0.021% and 0.32% worldwhile.
Contribution of the article to current knowledge
• The incidence rate (0.102%) in the study population was within the incidence rate range reported globally.
• The endophthalmitis diagnosis was confirmed through culture and/or PCR in 80% of the cases.
• In 93.3% of the cases, signs and symptoms developed within the first 14 postoperative days.
• To prevent endophthalmitis, it is essential implementing basic standardized prophylactic measures.
Cataract surgery is one of the most frequent ophthal mological surgical procedures in the world. Although it is usually a procedure with high success rate and low postoperative comorbidity, in some cases there may be complications, such as infection.
Endophthalmitis is the most dreaded infectious com plication. The patients may need one or more procedures (injection of therapeutic substances, vitrectomy), or even hospitalization for the intravenous administration of antibi otics. This might negatively impact on the patient’s quality of life and on the healthcare system.
The global rates of endophthalmitis ranges between 0.021% and 0.32%1,2. It is estimated that, annually, the total number of cataract surgeries performed worldwide is above 30 million. With that number in mind, and assuming one case of endophthalmitis out of a thousand surgeries, 30 000 postoperative endophthalmitis cases after cataract surgery occur annually, leading to blindness in the oper ated eye in around 10 000 patients3.
Perioperative antibiotic protocols have demonstrated efficacy to prevent this disease but are associated with more toxicity and resistance generation. So, the decision to use them should be based on clinical evidence.
The aim of this study was to estimate the incidence of postoperative endophthalmitis after cataract surgery at Hospital Italiano de Buenos Aires.
Material and methods
A retrospective cohort study was conducted on adult patients who underwent phacoemulsification for cataract at the Hos pital Italiano de Buenos Aires from January 1st, 2006, and December 31, 2020. Is a medical facility which provides a high degree of subspecialty expertise.
This includes patients diagnosed with endophthalmitis within the first 6 weeks after surgery. Patients who underwent extracapsular surgery or combined trabeculectomy and vitreo retinal surgery were excluded.
The study obtained the Institutional Review Board (Proto col N° 2727) approval and was conducted according to the Declaration of Helsinki standards.
The database was built from the endophthalmitis record of the Section of Infectious Diseases and Ocular Surface, double checking data with the electronic medical records (EMR).
The following data were collected: sex, age, presence of diabetes, immunocompromised conditions (hematologic malignancy or immunosuppressive medication), preoperative prophylactic measures. Best Correct Visual Acuity (BCVA) prior to the infectious event was collected as well as presented on the LogMAR scale.
In those patients where (ocular) media opacity did not allow assessing the posterior segment of the eye, an ocular ultra sound was performed to evaluate the vitreous humor and rule out complications such as retinal or choroidal detachments. An ultrasound showing echoes within the vitreous cavity and/ or the presence of vitreous membranes not associated with other causes was deemed positive.
In endophthalmitis cases, ocular fluids samples (aqueous humor, vitreous humor, or both) were obtained for analysis. Direct examination, culture (in solid culture medium of blood agar, chocolate agar and Sabouraud agar), antibiogram, and in most cases, polymerase chain reaction (PCR) were requested. Patients with signs and symptoms of endophthalmitis, and at least one of these tests positive were classified as proven endophthalmitis. In patients with signs and symptoms of en dophthalmitis but with negative results in the aforementioned tests, other possible causes (such as toxic anterior segment syndrome [TASS], non-infectious uveitis) were ruled out, and they were classified as suspected endophthalmitis cases.
According to the clinical presentation, an intravitreal in jection of vancomycin 1 milligram (mg) (0.1 milliliter [ml]), ceftazidime 2 mg (0.1 ml), and dexamethasone 0.4 mg (0.1 ml) (the latter in cases of suspected bacterial etiology) and/ or pars plana vitrectomy were performed.
Prior to surgery, all patients underwent prophylaxis with antibiotic eye drops with fourth-generation quinolones (moxi floxacin 5 mg/ml or gatifloxacin 3 mg/ml) two hours before surgery, povidone iodine 10% was applied to the periocular skin, and povidone iodine 5% to the cornea and conjunctival sac for a minimum of three minutes prior to the surgery. In the postoperative recovery, (topic) fourth-generation quinolone was administered every 6 hours associated with anti-inflamma tory corticosteroid (dexamethasone 1 mg/ml or prednisolone acetate 10mg/ml) at the surgeon’s discretion.
As outcomes, incidence of postoperative endophthalmitis, time to clinical presentation and clinical presentation type, iso lation rate of the causative microorganism, and post-treatment final visual acuity were recorded.
For the statistical descriptive analysis, mean and standard deviation (SD) were used for quantitative variables, and propor tions with their 95% confidence intervals (95%CI) were used for categorical variables. STATA 13.0 software (StataCorp, College Station, Texas 77845, USA) was used for the statistical analysis.
Results
A total of 29 326 cataract phacoemulsification surgery performed between 2006 and 2020 were included. Thirty endophthalmitis cases diagnosed within 6 weeks after surgery were identified. The annual incidence of acute en dophthalmitis was 0.102% (95%IC 0.069-0.146). Tables 1 and 2 summarize baseline characteristics, risk factors and clinical presentations.

In some cases, it was not possible to collect data regarding incision type or duration of surgical procedure due to lack of surgical protocols.
An ocular ultrasound was performed on twenty-two (73.3%) patients. It was positive in fourteen (63.6%) and negative in eight (36.3%) patients.
The mean time of symptoms onset was seven days (SD 8.5). There were fourteen (46.6%) cases of early onset between the 1st and the 3rd day, six (20%) cases between the 4th and the 7th day, eight (26.6%) cases between the 8th and the 14th day, and two (6.6%) case of late onset after 14 days.
The endophthalmitis diagnosis was confirmed in twenty-four patients (80% of the cases) through culture and/or PCR.
Cultures were performed in twenty-eight (93.3%) patients, and microorganism isolation was achieved in eleven (39.2%) cultures (Table 3).

Two cases of mixed infection were recorded, one due to Candida along with Streptococcus, and the other had a positive PCR for Propionibacterium acnes, with positive cultures for Aspergillus sp.
PCR was performed in seventeen (56.6%) patients; microorganisms’ genome was identified in sixteen (94.1%) of those patients’ samples (Table 4). In two patients, only PCR was performed since samples were not enough for cultures.

Regarding treatment options (n: 30 patients), intra vitreal injection of antibiotics was administered only to seventeen (56.6%) patients; initial vitrectomy was per formed in thirteen (43.3%) patients, vitrectomy after one intravitreal injection of antibiotics in five patients (16.6%) and one (3.3%) patient required evisceration. Vitrectomy was performed in patients showing best corrected visual acuity (BCVA) equal to or lower than 1.0 LogMAR (loga rithm of the minimum angle of resolution).
Regarding systemic treatment, oral medication was administered to twenty-one (70%) patients depending on the clinical presentation with moxifloxacin 400 mg per day, ciprofloxacin 500 mg every 12 hours, or voriconazole 200 mg every 12 hours; nine (30%) patients received in travenous treatment with vancomycin 1 gram (g) every 12 hours and ceftazidime 1 g every 8 hours or only imipenem 1 g every 6 hours.
Final BCVA mean was 0.5 (SD 0.5) and median 0.2 (IQR 0.0-1.0). Final BCVA was higher than 0.3 LogMAR in fourteen (46.6%) patients, between 0.4 and 1.0 LogMAR in three (10%) patients, and lower than or equal to 1.0 LogMAR (legal blindness) in twelve (40%) patients, one patient results (33%) could not be recorded because he passed away.
Discussion
The incidence rate (0.102%) in the study population was within the incidence rate range reported globally. Dur ing a systematic review, the endophthalmitis incidence rates in different parts of the world are 0.14% (6935/5 133 623) in North America, 0.07% (1253/1 777 045) in Europe, 0.14% (723/504 471) in Australia, 0.15% (1108/763 690) in Asia, 0.32% (26/8190) in Africa, and 0.27% (74/27 264) in South America2. Most of these patients received intracameral antibiotics as a prophy lactic measure. In a recent large meta-analysis, since the year 2000, the incidence of endophthalmitis has ranged from 0.012%-1.3%4. And in another systematic review from 1963 to March 2003 out of a total of 3 140 650 cataract extractions resulted in an overall endo phthalmitis rate of 0.128%5.
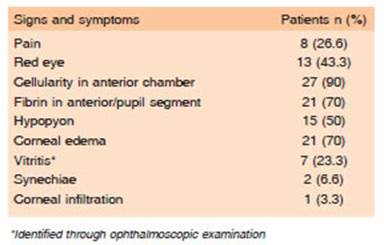
In the studied cohort, hypopyon (50%) and red eye (43.3%) findings were lower than those found in the Endophthalmitis Vitrectomy Study (EVS) (75 to 85% of hypopyon, 82% of red eye). The report of pain was not frequent (26.6%) compared to others (74% EVS, and 79% European Society of Cataract & Refractive Sur geons [ESCRS])6. This leads to increase the diagnostic suspicion of a potentially severe condition, even when these frequent clinical attributes found in other series, are not present.
The endophthalmitis diagnosis was confirmed through culture and/or PCR in twenty-four (80%) patients. This global rate of positive results has been slightly higher than those obtained in the EVS and ESCRS studies (69%)7,8.
In 93.3% (n:28) of the cases, signs and symptoms de veloped within the first 14 postoperative days, compared to 78% in EVS and 86% in ESCRS. Two cases (6.6%), one due to Aspergillus sp and the other with none germ recovered, presented after 14 days, compared with 22% EVS and 14% ESCRS.
The studied population presented a high isolation pro portion of gram-negative microorganisms (Pseudomonas aeruginosa). These cases were documented as part of two hospital outbreaks in 2011 (n:5) and 2015 (n:3). In order to face these events, an action plan for isolation of microorganisms in the surgical equipment was agreed with the HIBA Infection Control Committee; however, the causative source of peri or intraoperative contamina tion could not finally be identified. Therefore, different measures of asepsis and prophylaxis were implemented in operating rooms and surgical instruments (review of filters in air conditioning systems, individual use of drops per patient, frequent disposal of povidone iodine, increase in phacoemulsification hand parts, sterilization protocols review, among others).
The second most frequent isolated microorganism in our study was Staphylococcus epidermidis and Strep tococcus, the first being the prevalent microorganism in most of the publications8,9-13.
All patients received oral or intravenous treatment. The use of fourth-generation quinolones (gatifloxacin or moxifloxacin) is a treatment option accepted by several authors, since these antibiotics show good tolerability and intraocular penetration14.
Patients with an acute virulent presentation received intravenous treatment according to the recommendation ESCRS guidelines6.
Final BCVA was higher than 0.3 LogMAR in 46.6% (n:14) patients, slightly lower compared to 53% of the EVS. In another study where early vitrectomy was performed on a consecutive series of 47 eyes, 91% achieved final BCVA higher than 0.3 LogMAR15-17.
Of the patients who presented at baseline with a BCVA lower than or equal to 1.0 LogMAR (83.3%), final acuity lower than or equal to 1.0 LogMAR was achieved in 44%. This is consistent with the EVS, which showed the patient's visual outcome was the VA at the moment of the initial presentation, regardless of the identified microorganism17.
The two cases with the worst clinical progress, were one patient who developed a phthisis bulbi, and a second one who underwent an evisceration, and corresponded to two virulent pathogens, Pseudomonas aeruginosa and Aspergillus sp, respectively.
The limitations of this study are related to the retro spective nature of the design, and to data of the surgical procedure not recorded and analyzed (duration of the surgical procedure, size and type of incision, intraoperative complications). On the other hand, it only represents the results of a single hospital in the region.
The incidence of endophthalmitis after cataract sur gery in a tertiary hospital of Buenos Aires is within those reported worldwide.
Regional data of endophthalmitis incidence helps to decide if the introduction of new antibiotic prophylaxis measures should be implemented.

