










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkArchivos argentinos de pediatría
versión impresa ISSN 0325-0075versión On-line ISSN 1668-3501
Arch. argent. pediatr. vol.114 no.6 Buenos Aires dic. 2016
http://dx.doi.org/10.5546/aap.2016.521
ORIGINAL ARTICLE
http://dx.doi.org/10.5546/aap.2016.eng.521
Communication skills of residents to families with Down syndrome babies
Assoc. Prof. Derya G. Dogan, M.D.a, Yesim Kutluturk M.D.b, Meltem Kivilcim M.D.a and Sinem K. Canaloglu, MSc.a
a. Inonu University School of Medicine, Department of Developmental Behavioral Pediatrics, Malatya, Turkey
b. Inonu University School of Medicine, Department of Pediatrics, Malatya, Turkey
E-mail address: Derya G. Dogan, M.D.: deryagumus@yahoo.com
Funding: None.
Conflict of interest: None.
Received: 4-26-2016
Accepted: 7-22-2016
ABSTRACT
Background. Generally, pediatricians are the first health caregivers to deliver initial diagnosis of Down syndrome (DS) to the families. However, most of the parents are not satisfied with the contents and how they receive information when their child is born with DS. Pediatric residents should target educational interventions to help parents to overcome with these issues and to provide accurate information. The objective is to assess comfort levels and training requirements of pediatric residents to communicate with parents of babies born with Down syndrome.
Methods. Diagnostic Situations Inventory (DSI) is a rating scale which included ten questions to assess discomfort level. A survey was sent via mobile, websites and all the social media which were available to all pediatrics residents in the country. Socio-demographic factors including information about training requirement were collected as well. Results. From the 326 participants, total mean discomfort level was 30.22 in DSI out of 50 which was the highest score. Discomfort level was significantly increased in female participants (p= 0.033). Being female (p= 0.014), having less residency level (p= 0.028), examining less number of patients with Down syndrome (p= 0.025) and having higher discomfort levels (p= 0.001) were found to be related with increased training requirement. From the residents, 84% declared the need for additional training.
Conclusions. This study showed that pediatric residents had a high level of discomfort when communicating with parentes of newborn with Down Syndrome. Female residentes had a discomfort level significantly higher than male residentes.
Key words: Pediatrics resident; Down syndrome; Diagnosis; Communication skills; Training.
INTRODUCTION
Down syndrome (DS) is the most common genetic condition, 1 out of every 800 live births do get affected by DS,1 and more than 85% of mothers with affected baby learn their children's diagnosis after the birth.2 Generally pediatricians are the first health caregivers to deliver DS diagnosis to the families in countries where genetic counseling is not widespread, and they are in a position to help parents to overcome the first burden when they hear that their baby is diagnosed with DS. It is reported, even after twenty years, families generally remember the first words that the doctors have used during the conversation about the initial diagnosis.3 Unfortunately, families were not satisfied with the information about having a baby with DS along with the content and how to report it.4,5
The diversity among cultures, educational background, and differences in language dialect are extremely important in order to communicate genetic information.6 During that situation of delivering the news about DS to the families, we do not know how pediatric residents feel, and behave with families.
As far as we know, in order to develop communication abilities only one instrument, the "Diagnostic Situations Inventory (DSI)" has been developed to examine the attitude of residents when delivering diagnosis of a newborn baby with Down syndrome to the family. Diagnostic Situations Inventory was developed by Ferguson et al. from USA and was used for improving pediatrics and obstetrics residents' understanding of issues, comfort levels and patient needs regarding screening for and diagnosing DS.7
The ultimate goal of this study was to generate a better perception about delivering news in a sensitive and appropriate manner to the families who have children with newly diagnosed DS among pediatrics residents in eastern countries.
The objective was to assess comfort levels and training requirements of pediatric residents to communicate with parents of babies with Down syndrome.
METHODS
This was a cross-sectional, self-administered, mailed survey. The Diagnostic Situations Inventory was designed on surveymonkey.com website and was distributed to pediatric residents with a cover letter by mobile, websites, and social media at two different times on January and February 2015. Also there was a reminder letter that was mailed to residents whose questionnaire had not been received in two weeks after the initial mailing. The cover letter explained the purpose of the study and emphasized that the participation was completely voluntary. The inclusion criterion was being a pediatric resident in Turkey during the survey. Residents who were graduated before the year 2000 and after 2014 were excluded. The sample size was calculated by power analysis that it should be at least 128 participants.
According to information gathered from nine questions asked before starting to apply DSI, demographic information including the age, gender, year of education, marital status and number of the children with DS assessed during residency program were obtained. Additionally, one question was asked to determine if the resident wanted to have training in this field or not.
In order to test the comfort level of pediatric residents in delivering a diagnosis of Down syndrome, the DSI was implemented with the permission of the original author. The inventory updated by Lunney et al. in 20128 was used in this research.
Diagnostic Situations Inventory reflects varying degrees of ambiguity in many challenges related to the diagnosis of DS. Five of the items measure discomfort with medically ambiguous questions for which there were no clear medical answers, and the other five items measure discomfort with unambiguous questions for which more factual information could be provided. Since the inventory is prepared both for pediatric and obstetric residents, the tenth question ("A patient who has been told that her screening test indicates she is at a greatly increased risk for having a child with Down syndrome decides against having a definitive diagnostic test") of the inventory which is about prenatal diagnosis was changed to a question ("A parent asks you if her child would be able to do his/her own self-care like other healthy children") about self care with the permission of the author. Responses were scored using Likert scales with ''1'' being ''Not at All Uncomfortable'' and ''5'' being ''Extremely Uncomfortable'' for each item. The greatest possible total discomfort score was 50, with a potential range from 10 to 50. The higher scores were considered as more uncomfortable.
The study protocol was approved by the Ethic Committee of Inonu University.
Statistical analysis was performed using SPSS 17.0. Results were expressed as descriptive statistics. Data were analyzed with Pearson's chi-square for uncorrelated data and independent f-test for correlated data. As a method of analysis mean and standard deviation value were used. P values of <0.05 were considered significant.
RESULTS
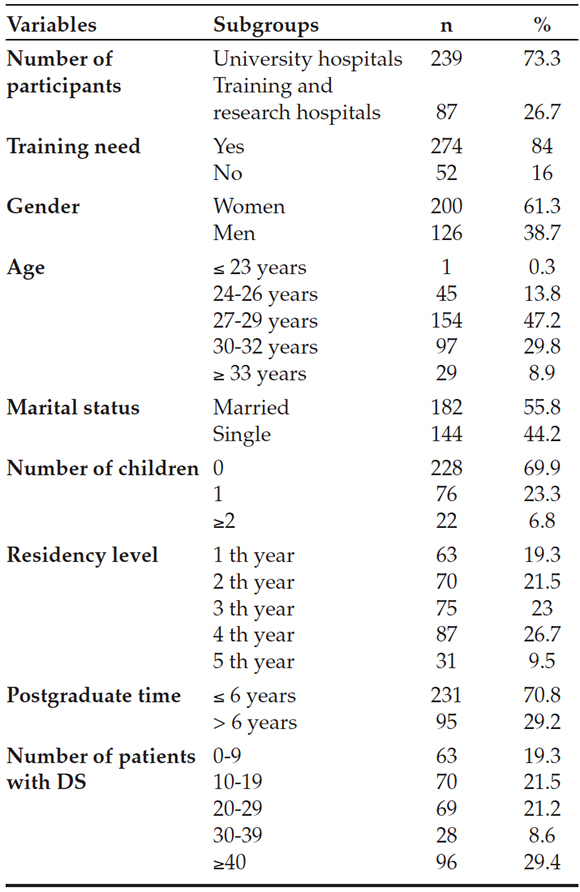
Mails were sent to 1000 residents and responded by 341 residents. By year 2015, there were a total of 2441 pediatric residents (1368 of them in university hospitals and 1073 of them in training and research hospitals). The response rate was 34.1%. Fifteen participants were removed because of inaccurate or missing data, and 326 responders were included in the study. There were 239 (73.3%) pediatric residents from university, and 87 (26.7%) were from training and research hospitals. Out of the total residents, 61.3% were women, and 19.3% were in their first years. Socio-demographic characteristics of the participants are presented in Table 1.
Table 1. Socio-demographic characteristics of pediatric residents (N: 326)
Total mean discomfort level was 30.22 ± 7.21 in DSI out of the highest score of 50. The mean score for ambiguous questions was 17.77 ± 3.73 and non-ambiguous questions 12.45 ± 4.19.
Average mean score for each item was 2.60. The question about the advice related to increased risk of heart problems got the lowest mean score (2.06 ± .96), and the question about overhearing of a mother of saying a colleague that ''Down children never amount to anything" got the highest mean score (4.16 ± 0.99). The mean scores of all items are shown on Table 2.
Table 2. Diagnostic Situation Inventory score items and scores of discomfort

Mean discomfort level (p= 0.033) and total ambiguous level (p= 0.008) were significantly higher in female residents than male residents with Pearson chi-square statistical method. Female doctors (176; 53.99%) stated more training than male (98; 30%) doctors (p= 0.014).
By independent T-test, being female (p= 0.014), having less residency level (p= 0.028), examining less number of patients with Down syndrome (p= 0.025) and having higher discomfort levels (p= 0.001) were found to be related with increased training requirement. The mean residency year was 2.79 ± 1.28 in the group who needed training, and it was 3.21 ± 1.17 in the group of who did not need training (p= 0.03). Using the same statistical method the mean number of examined patients with DS was 29.9 ± 1.50 in the group of who need training, and it was 35 ± 1.43 in the group of who don't need training (p= 0.03).
Most of participants from university hospitals (84.1%) and training and research hospitals (83.9%) indicated the need of additional training about delivering information to families who have newborns with Down syndrome.
DISCUSSION
This study demonstrated that pediatric residents from an eastern country are not comfortable when delivering information about newborns with Down syndrome to their families. Female residents, being in their first three years of residency and examining less than 30 patients with DS was associated with higher discomfort and increased training requirement.
DSI was developed in Kentucky University to improve the incompetencies of obstetrics-gynecology and pediatric residents when counseling the parents of babies with DS. The residents' knowledge and comfort levels were assessed by using pre and post-test with an education CD-ROM.7 After 6 years, DSI has been modified by Lunney et al. and has been accepted as a research with web-based tutorial. In that study, Lunney has found the mean discomfort levels of residents 23.05 with the highest discomfort level 35.8 The mean discomfort level of Turkish residents was 30.22 with the highest score 50. Probably the greater dissatisfaction among Turkish residents is the result of not getting any structured clinical training regarding delivering bad news to the families.
In the study of Lunney 97% of residents have declared that training is necessary, on the contrary 84% of Turkish residents have wanted training. Because of knowledge and discomfort levels of residents were assessed with pre-tests and post-tests within an educational programme in Lunney's study, residents might have been more willing to get training.8
In this study, female residents had higher discomfort levels than males, and they were found to be more willing to get training. The gender difference is not mentioned in the research of Lunney's.8 Studies have shown that female physicians have different communication skills than males. Having better patient management of female doctors due to good communication are known.9 In a meta-analytic review, Roter et al. found that female doctors engage in more positive talk (such as encouragement), ask more psychosocial questions, discuss more about emotions and demonstrate more partnership building behaviours.10
By providing appropriate communication and assisting others with health and community care services, pediatricians may increase strong attachment with the patients and his/her family. Families seek up-to-date, accurate, balanced information.5,11,12 If families get knowledge from reliable healthcare givers, they can feel more optimistic about having a baby with DS. Optimistic feelings encourage healthy parent child relationship and optimal emotions, growth and development.13
The post-tests in Lunney and Ferguson researches' have shown that the comfort levels of residents have increased with the educations by CD-ROM or web-based tutorial7. Our survey differed from the original in that we could not test the knowledge level of residents about DS due to a technical impossibility. For example, all of our surveys and their results are subject to self-reporting and responder bias. Furthermore, physicians who have a specific interest in DS may be more likely to respond better than those with less interest. Response rate was 34.0%. This may be sufficient number of participant for the web-based research across the country.
This study represents a first step in understanding Turkish pediatricians' attitude and willingness to have an education in delivering diagnosis to the families with DS. Communication is a learned skill and not a personality trait.14-16 In order to provide a good life and adaption to the diagnosis for families, first and foremost pediatricians have to be knowledgeable about DS and interventions.5 There is a substantial need of receiving a formal training to improve pediatricians' comfort levels in delivering diagnosis of DS. Pediatric residency programs must incorporate delivering bad news to the families with DS into pediatric training beyond knowledge provision to achieve trainees' competence and skill development.5
Further research examining which educational interventions are most influential in changing physician attitude in delivering bad news may help prompt more widespread adoption in medical education. Web-based tutorials,8 simulation-based17 and competency-based communication skills18 workshop/curriculum were reported to be helpful and have been studied to be effective models among pediatric residents.
Having higher comfort levels when communicating will be useful for not only DS but also the other diagnosis like spina bifida, autism and fragile X syndrome.8
CONCLUSION
This study showed that pediatrics residents had a high level of discomfort when communicating with parentes of newborn with Down Syndrome. Female residentes had a discomfort level significantly higher than male residentes.
There is a necessity of receiving a formal
training to improve Turkish pediatricians' comfort levels in delivering diagnosis of DS in medical schools and applying it to continuing medical education.
1. Parker SE, Mai CT, Canfield MA, Rickard R, et al. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 2010;88(12):1008-16. [ Links ]
2. Skotko BG. Prenatally diagnosed Down syndrome: mothers who continued their pregnancies evaluate their health care providers. Am J Obstet Gynecol 2005;192(3):670-7. [ Links ]
3. Carr J. Six weeks to twenty-one years old: a longitudinal study of children with Down's syndrome and their families. Third Jack Tizard memorial lecture. J Child Psychol Psychiatry 1988;29(4):407-31. [ Links ]
4. Skotko B. Mothers of children with Down syndrome reflect on their postnatal support. Pediatrics 2005;115(1):64-77. [ Links ]
5. Skotko BG, Kishnani PS, Capone GT; Down Syndrome Diagnosis Study Group. Prenatal diagnosis of Down syndrome: how best to deliver the news. Am J Med Genet A 2009;149A(11):2361-7. [ Links ]
6. Rosas-Blum E, Shirsat P, Leiner M. Communicating genetic information: a difficult challenge for future pediatricians. BMC Med Educ 2007;7:17. [ Links ]
7. Ferguson JE 2nd, Kleinert HL, Lunney CA, Campbell LR. Resident physicians' competencies and attitudes in delivering a postnatal diagnosis of Down syndrome. Obstet Gynecol 2006;108(4):898-905. [ Links ]
8. Lunney CA, Kleinert HL, Ferguson JE 2nd, Campbell L. Effectively training pediatric residents to deliver diagnoses of Down syndrome. Am J Med Genet A 2012;158A(2):384-90. [ Links ]
9. Jefferson L, Bloor K, Birks Y, Hewitt C,et al. Effect of physicians' gender on communication and consultation length: a systematic review and meta-analysis. J Health Serv Res Policy 2013;18(4):242-8. [ Links ]
10. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. JAMA 2002;288(6):756-64. [ Links ]
11. Lynch EC, Staloch NH. Parental perceptions of physicians' communication in the informing process. Ment Retard 1988;26(2):77-81. [ Links ]
12. Hedov G, Wikblad K, Annerén G. First information and support provided to parents of children with Down syndrome in Sweden: clinical goals and parental experiences. Acta Paediatr 2002;91(12):1344-9. [ Links ]
13. Van Riper M, Ryff C, Pridham K. Parental and family well-being in families of children with Down syndrome: a comparative study. Res Nurs Health 1992;15(3):227-35. [ Links ]
14. Simpson M, Buckman R, Stewart M, Maguire P, et al. Doctor-patient communication: the Toronto consensus statement. BMJ 1991;303(6814):1385-7. [ Links ]
15. Kurtz SM. Doctor-patient communication: principles and practices. Can J Neurol Sci 2002;29(Suppl 2):S23-9. [ Links ]
16. Mehta PN. Communication skills--talking to parents. Indian Pediatr 2008;45(4):300-4. [ Links ]
17. Greenberg LW, Ochsenschlager D, O'Donnell R, Mastruserio J, et al. Communicating bad news: a pediatric department's evaluation of a simulated intervention. Pediatrics 1999;103(6 Pt 1):1210-7. [ Links ]
18. Silva DH. A competency-based communication skills workshop series for pediatric residents. Bol Asoc Med P R 2008;100(2):8-12. [ Links ]

