











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide 1 and in Argentina. 2 The so-called "social gradient" (decrease in mortality and morbidity rates as social status increases) 3 has already been shown to occur in a wide range of conditions, including CVD. 4
In urban areas, population has easier access to health services, but environmental factors, such as pollution, noise, and daily stress, affect the cardiovascular health. 5 The peri-urban areas have the disadvantage of being a transitional and unstable territory in terms of social networks, which is associated with increased cardiovascular risk. 6,7 In addition, it has been conventionally described that the prevalence of CVD is lower in rural areas. 8 However, this concept is changing, 9 since a high prevalence of overweight was observed in different indigenous communities. 10,11 In Argentina, a 38% prevalence of metabolic syndrome has been found in the Toba community (indigenous people living in central Chaco). 12 More recently, we have found that the Quilmes community (rural indigenous people living in the middle and high mountains who still preserves pre-Inca traditions) in Tucumán has a prevalence of risk factors for CVD similar to that in urban areas. 13
The province of Tucumán, located in northwestern Argentina, with an area of 22 525 km², has rural areas with difficult access, densely populated urban areas (the capital city has 605 000 inhabitants in 91 km2) and strings of peri-urban areas surrounding the cities. In the urban and peri-urban areas of Tucumán, according to data from the National Institute of Statistics and Censuses (Instituto Nacional de Estadísticas y Censos, INDEC), the poverty rate was 42.7% in the second quarter of 2022. 14 However, the impact of the environment on CVD risk factors in women is still being studied. This view is consistent with the worldwide literature which indicates that there is a dichotomy between real and perceived CVD risk in women. 15,16
This study aimed to evaluate the cardiovascular risk profile in adult women from rural, peri-urban and urban areas of the province of Tucumán (Argentina) and to analyse their differences.
METHODS
An analytical cross-sectional study conducted in 3 population groups of women from different areas of Tucumán.
- Rural group: Women from Quilmes, a middle and high mountain area where pre-Inca traditions are still preserved, who participated in the Sonqo Calchaquí 2018 study 13 (n = 125).
- Peri-urban group: Women from Villa Muñecas, a peripheral neighbourhood located 3 km away from the city, who participated in a cardiovascular health activity organized by the Argentine Society of Cardiology (Sociedad Argentina de Cardiología, SAC), Tucuman District, on Women's Day in March 2021 (n = 50).
- Urban group: Women living in the city of San Miguel de Tucumán and performing desk jobs at the Municipality, who underwent a cardiovascular health registry in September 2019 (n = 112).
In this study, the following variables were assessed:
- Age: Expressed in years.
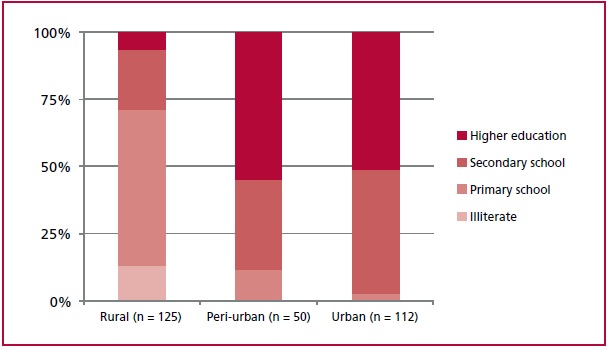
- Education level: Expressed as completed level (illiterate, primary school, secondary school or higher education).
- Presence of the following CVD risk factors: Smoking, dyslipidemia, hypertension (HT) or diabetes. Women were asked about the presence of said risk factors. A semiquantitative score was made according to the number of risk factors mentioned (0 to 4).
- Salt added to cooked food.
- Weight (kg): It was measured with a digital scale.
- Height (cm): It was measured with a portable height rod.
- Neck circumference (cm): It was measured with a non-expandable measuring tape. It was considered increased when it was greater than 34 cm. 17
- Waist circumference (cm): It was measured with a non-expandable measuring tape. It was considered increased when it was greater than 88 cm. 17
- Body mass index (BMI): It was calculated as weight in kg/(height in m2. Women were classified according to their nutritional status as follows: underweight (BMI <18.5); nor mal weight (BMI ≥18.5 and <25); overweight (BMI ≥25 and <30); obesity (BMI ≥30 and <35); severe obesity (BMI ≥35 and <40); and morbid obesity (BMI ≥40).
- Systolic blood pressure (SBP) and diastolic blood pressure (DBP) values were expressed in mmHg: It was measured with an Omron 7120® automatic digital sphygmoma nometer according to the applicable guidelines. 18 Pulse pressure (PP) was calculated as SBP - DBP and mean blood pressure (MBP) as DBP + (PP/3).
- Heart rate and O2 saturation were measured with an An Mat® pulse oximeter.
Statistical Analysis
The results were compiled in a Microsoft Excel 2010 spreadsheet and expressed as percentage (%) or mean ± standard error, as required. The statistical analysis was performed with GraphPad Prism 5.02 software. Student’s t-test, ANOVA with Newman-Keuls’ post-test, Pearson’s correlation (r) or chi-square test (2) were used, as required. Results were considered significant with a <5% probability (p <0.05).
RESULTS
The average age of the studied women was 48.9 ± 0.9 years, with no differences among the 3 groups: (rural: 50.2 ± 1.8 years, peri-urban: 47.7 ± 1.9 years, urban: 48.1 ± 1.0 years, p = NS).
Education level of the studied women is shown in Figure 1. Illiterate women were reported only in the rural group. The percentage of women with higher education level was greater in the urban and peri-urban groups than in the rural group (p <0.001).
Anthropometric and hemodynamic values are shown in Table 1. Weight and height values were lower in the rural group than in the other two groups, but the average BMI was elevated in all the studied population, with no differences among the 3 groups.

Neck circumference was smaller in the urban group, but waist circumference was similar in the 3 groups. Although SBP and DBP values, on average, remained within the normal rank, they were higher in the peri-urban and urban groups than in the rural group, and PP values were higher in the urban group than in the peri-urban group. Heart rate values were also higher in the urban group, and O2 saturation was lower in the rural group.
When nutritional status was evaluated, 27.9% of women showed normal weight; 29.7% was overweight and the remaining 42.4% had some level of obesity (26.5% obesity; 10.6% severe obesity and 5.3% morbid obesity). No underweight women were found. The nutritional status distribution was similar in the 3 groups (p = NS).
Increased neck circumference was observed in 62% of the women in the rural group, in 79% in the peri-urban group and in 41% in the urban group (p <0.001) and increased waist circumference was observed in 69% of the studied women, with no significant differences among the 3 groups.
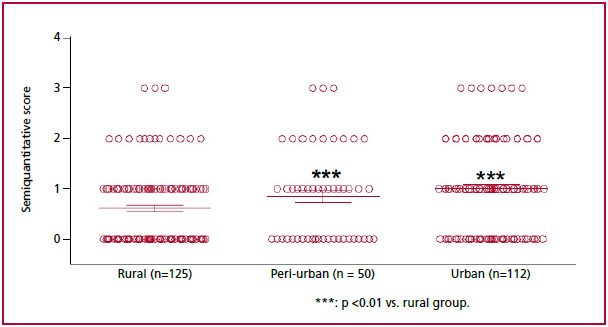
The number of risk factors for CVD, according to the semiquantitative score, was higher in the urban group (Figure 2A). The proportion of women with no risk factor was higher in the rural group (53%) than in the peri-urban (44%) and urban (33%) groups (p <0.001). When each risk factor was analysed separately, HT was the most prevalent (30%), followed by dyslipidemia (25%), smoking (23%) and diabetes (6%). The urban group reported a higher percentage of smoker women (p <0.001). Similar percentages for the other risk factors were found in the 3 groups (Figure 2B).
Addition of salt to cooked meals was observed in 47% of women. There were no significant differences regarding this in the 3 groups.
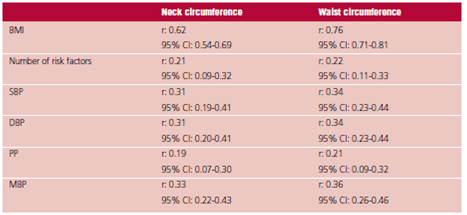
A positive correlation was found between neck and waist circumferences (r 0.65; 95% CI: 0.57-0.71; p <0.001). At the same time, neck and waist circumferences were positively correlated with BMI, the number of CVD risk factors and blood pressure (BP) (Table 2).
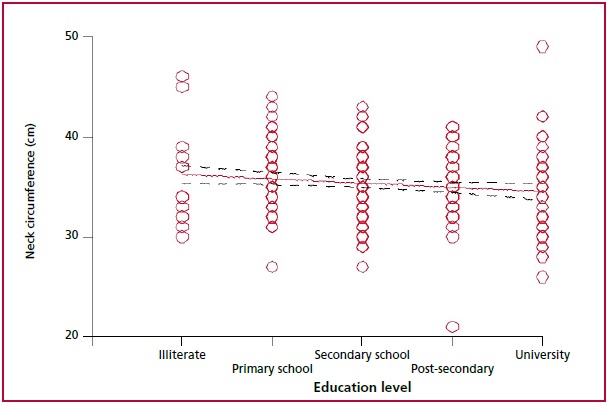
Education level was positively correlated with heart rate (r 0.21; 95% CI 0.09-0.31; p <0.001) and O2 saturation (r 0.38; 95% CI 0.27-0.47; p <0.001) and negatively correlated with neck circumference (Figure 3) and PP (r -0.1470; 95% CI: -0.26 to -0.03; p <0.05). Age was positively but poorly correlated with neck circumference, waist circumference, the number of risk factors, SBP and DBP, but was not correlated with BMI (r: 0.06; 95% CI: -0.05-0.18; p = NS).
DISCUSSION
The main result of this study is that, regardless of the area where the studied women live (rural, peri-urban or urban), they had increased BMI, large waist circumference and high percentage of obesity. When observing the anthropometric values in the 3 populations, women in the rural group showed lower weight; however, as they also were smaller in height, they had a BMI similar to that of the other two groups, suggesting that these differences could be racial rather than nutritional.
It should be noted that 42.4% of the studied women had some level of obesity. According to the 4th National Risk Factor Survey (Encuesta Nacional de Factores de Riesgo, ENFR), 2 the prevalence of obesity in Argentina was 33.4%, and 26.9% in Tucumán, without discriminating by sex. The level of obesity observed in this study, which is higher than that reported by the ENFR, 2 could be due to the fact that in the rural and peri-urban groups, we studied women who attended health services (which could be biased, since women with a lower BMI may not have attended health services), and in the urban group, we studied women who worked in offices -and therefore had a higher degree of sedentary lifestyle. The high prevalence of obesity is worsened by the fact that 5.3% of women are morbid obese. In addition, the increased waist circumference values indicate central (abdominal) fat distribution. Central obesity is associated with a poor quality diet and lack of physical activity. 19 Furthermore, there is a direct relation between central fat distribution and CVD onset. 20 The presence of central obesity indicates risk for CVD in the studied women, regardless of the area where they live. This view is supported by the fact that neck circumference -although, on average, had not increased- had changed in more than half of the women, and its value was positively correlated with BMI, waist circumference, BP and a number of CVD risk factors. In this regard, it has been indicated that an increased neck circumference is associated with metabolic alterations 21 and higher mortality, even with normal BMI. 22 Based on the negative correlation between education level and neck circumference, we could assume that higher education level is associated with better diet choice or access to a healthier diet. In this regard, no differences were observed in the addition of salt to food, so the diet of the 3 groups should be investigated in future studies.
Women in urban areas have higher prevalence of smoking, a fact that could dilute the protection suggested by lower values of the neck circumference. In contrast to our findings, in a study conducted in the USA it was found that in urban areas, where the education level is higher, the prevalence of smoking is lower than in rural areas, 23 and in a study conducted in China it was observed that education level was inversely related to smoking. 24 The positive association between heart rate and education level suggests greater stress in women with a higher level of education, a fact that may be associated with increased smoking in this population. In a population of recycling workers, it was shown that elevated heart rate is associated with a higher degree of stress, 25 and under laboratory conditions it was shown that stress increases cigarette consumption in both men and women. 26
Historically, regarding CVD risk factors, the prevalence of CVD and diabetes has been higher in urban than in rural populations. 8 Nowadays, this difference is controversial. Decreased survival and increased CVD have been reported in indigenous communities in several areas, including Australia, New Zealand, and the United States. 9 More recently, our working group found that in the Quilmes community, both men and women have a prevalence of CVD risk factors similar to that in urban areas. 13 Interestingly, this trend is replicated in the studied women of this population, which supports the hypothesis raised in the previous paragraphs: regardless of the environment, the levels of obesity and the cardiovascular risk profiles in women are similar.
It should be highlighted, among other points, that the BMI is within the overweight rank in the rural and peri-urban groups and within the obesity rank in the urban group;
neck circumference is higher in the rural and peri-urban groups; the percentage of women without risk factors is higher in the rural group; and smoking is higher in the urban group. However, the fact that the distribution of body fat is similar (central type) in the 3 groups would indicate a high risk for CVD in the entire studied population and a different impact of the risk factors in the 3 groups, which suggests that the preventive approach should also be differentiated.
Furthermore, although BMI did not change with increasing age, we observed a correlation between age and waist and neck circumferences, SBP, DBP, and the number of risk factors. It has been shown that fat body mass increases and lean body mass decreases with aging, 27 which could explain why BMI is maintained over time.
CONCLUSIONS
Regardless of the environment (urban, peri-urban or rural), women in Tucumán are overweight or obese and have other risk factors for CVD, which could significantly affect their cardiovascular health in the future. Although in all cases women should be made aware of the benefits of a healthy diet and preventive lifestyle including weight control, physical activity and stress reduction, in rural and peri-urban areas more emphasis should be given to improve the level of education and access to healthcare systems, while in urban areas the priority is to work on other aspects, such as smoking cessation.

