











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Cardiovascular disease (CVD) is the leading cause of death in women and its prevalence has increased over the past decades. Despite this fact, women are less likely to receive guidance or preventive treatment to reduce it. 1
The effect of cardiovascular risk factors (CRF) as hypertension (HT), diabetes (DBT), hypercholesterolemia (HC), smoking, excess weight and sedentary lifestyle on cardiovascular health is well known, but the evidence shows that the magnitude of their impact exhibits sex-related variations. 2 In addition, women are exposed to unique sex- and gender-specific CRF as low socioeconomic status, certain psychosocial factors, gender-based violence, low education level, and environmental pollution. 3-6
Nowadays, most of the information on CRF and CVD in women comes from international studies, and although the national survey of risk factors (NSRF) 7 and the study published by the Heart and Women Area of the SAC in 2006 8 collected local information, there are no current data on women's perception of their own risk.
Through this survey on women's perception, awareness and management, the Heart and Women Area of the Argentine Society of Cardiology (SAC) sought to establish a diagnosis of the situation of self-perception of CRF and CVD, detect their prevalence and investigate the level of perception and awareness of women on CRF and CVD to define the most vulnerable groups to guide specific actions.
METHODS
We conducted an observational, cross-sectional study in July 2021, using a voluntary, anonymous, and self-administered online survey. A form was created on the RedCap platform and was accessed via a link distributed through social media and WhatsApp by members of the Heart and Women Area, with broad participation of the regional SAC districts. The information collected included age range, CRF, CVD, and risk perception (Appendix 1). In this self-administered survey, women reported if they perceived they had HTN, DM, dyslipidemia, or a history of CVD (myocardial infarction, percutaneous coronary intervention, coronary artery bypass graft surgery or a positive stress test). Hypercholesterolemia was considered independently of the last time cholesterol levels were tested. Similarly, we inquired about pregnancies and bad obstetric history (miscarriage, fetal death, gestational hypertension, gestational DM, and preterm birth before 37 weeks). Sedentary lifestyle was considered when the exercise time reported was less than 150 min per week. Former smoker was considered after 1 year of having quit smoking. Predefined categories of weight and waist circumference data were provided.
Women >18 years and older from different geographic locations in Argentina were included, and female doctors were excluded.
Statistical analysis
The population was divided into two groups according to age, ≤ 45 years, and > 45 years, to explore differences in the main variables in two different generations.
Qualitative variables are presented as frequencies and percentages. Discrete variables were analyzed using the chi square test or Fisher's exact test. For continuous variables, the t test or the Mann-Withney test were used. ANOVA and the Kruskal-Wallis test were used for comparisons among 3 groups or greater. A p value < 0.05 was considered statistically significant.
RESULTS
Conventional risk factors
A total 3338 women participated in the survey. Table 1 shows the baseline characteristics of the women surveyed; 34.8% were < 45 years and half of them (50.1%) belonged to the age range between 46-65 years.

In response to body measurements, 34.1% reported a weight > 70 kg and this answer was more common in women > 45 years than in younger women (38% vs. 29%, p < 0.01). A waist circumference > 80 cm was reported by 43.6% of respondents and was more common in women > 45 years (48% vs 35%, p < 0.01) (Figure 1).

Among conventional CRF, 12.1% did not know their blood pressure (BP) values and 24.2% considered that they had hypertension (HTN). When they were asked about their BP values, 6.1% responded their systolic BP was > 140 mm Hg (1.4% corresponded to the group that did not perceive they had HTN). Considering both criteria (reported HTN and elevated BP values), 25.6% of all the survey respondents had HTN, more frequent in the age group > 65 years (37.6%) (Figure 1).
Elevated total cholesterol (ETC) levels, > 200 mg/ dL were reported by 19.6% of the survey respondents while 29.2% did not know their values. Of the patients with ETC levels, 16.7% were taking lipid-lowering agents and 10.1% followed diet and exercise. Among women who were following an indication to manage ETC levels (diet, exercise or medication), 37% had values > 200 mg/dL despite these measures. On the other hand, 23% of women with TC levels > 200 mg/ dL did not follow any recommendation. Elevated TC levels were more common in > 45 years (31%) compared with those ≤ 45 years old (18%), p < 0.01.
Diabetes was reported by 5.4% and most survey respondents knew their blood glucose values (only 2.6% were not aware of them).
A waist circumference > 80 cm was more common in women with HTN (33.3% vs 16.7%), ETC levels (22.2% vs. 17.6%) and DBT (8.6% vs. 3.0%). Excess weight was associated with HTN (35.6% vs. 18%) and DM (10.6% vs. 2.8%).
Women with systolic blood pressure >140 mm Hg were more likely to have DM (16.5% vs. 5.2%), waist circumference > 80 cm (68.3% vs. 43.2%), and weight > 70 kg (60% vs. 33.5%).
In addition, women with diabetes had more prevalence of HTN (57% vs. 22.7%), waist circumference > 80 cm (68% vs. 41.8%) and weight > 70 kg (65% vs 32%). These differences were statistically significant in all the cases (p < 0.01).
Sex-specific risk factors
The obstetric history was also explored. Among survey respondents, 82.1% had been pregnant at least once, and 26.9% of them reported at least one of the following complications: HTN (8.2%), preterm birth (7.9%), miscarriage (7.4%) and gestational diabetes (4.9%). Only 37% underwent cardiology monitoring one year after the index delivery (vs. no monitoring p < 0.01). A bad obstetric history was more commonly associated with HTN (34% vs. 24%, p < 0.01), DM (7% vs. 5%, p = 0.04) and current CVD (14% vs. 11%, p < 0.01).
Oral contraceptives or hormone therapy was used by 15.2%, and most of these women (65%) belonged to the younger age group. Hormone therapy was less common in women with HTN (11.8% vs. 26.2%), ETC levels (13.5% vs 21%), waist circumference > 80 cm (35% vs 45%), and weight > 70 kg (26% vs 35%). All these differences were statistically significant (p < 0.01).
Cancer was reported by 7.9% and 91.4% had not been evaluated by a cardiologist during or after cancer therapy. A history of cancer was found in 11% of women > 45 years vs. 2% in younger women (p < 0.01). Hypertension was more common in women with a history of cancer (35% vs. 23%).
Habits, behavioral factors, and emotional sphere
Among survey respondents, 45.8% had a history of smoking and 11.3% were current smokers. Smoking was significantly associated with a waist circumference > 80 cm, sedentary lifestyle, and alcohol intake (13% vs. 7%).
We also explored habits as exercise, diet, and medical check-ups. A sedentary lifestyle was reported by 44.3%, and 57.4% admitted lack of adherence to a healthy and balanced diet. Sedentary lifestyle was more common in women aged 45 or less (42% vs 50%, p < 0.01). Women who exercised had significantly lower prevalence of HTN (21.7% vs. 26.8%), DM (4.4% vs. 7%), smoking habits (9% vs. 13.3%), waist circumference > 80 cm (38% vs. 50.1%) and weight >70 kg (27% vs 42.5%).
Most women had undergone cardiovascular assessment (87%), but this was less common in younger women.
Data on irritability, alcohol intake and sleep were collected to explore the emotional and behavioral spheres; 62.6% became easily irritable, mostly women up to 55 years of age (74%), and nearly half of them reported regular alcohol intake (48.6%). Sleeping difficulty was more common among women who reported regular alcohol intake (19% vs. 13.5% p < 0.01). Sleep disorders were reported by 49.5% and there was a significant association between ETC levels and weight > 70 kg. Sleep disorders were more common in women > 45 years.
Awareness and perception of cardiovascular disease
Among survey respondents, 10.9% had CVD, which was more common in those > 55 years. A history of myocardial infarction was the most common disease reported (51.1%), followed by revascularization procedures (30.4%) and indication of medical treatment after an exercise stress test (28.6%). Stroke was reported by 9.8% of the respondents.
When awareness of cardiovascular risk was explored, more than 50% responded that cancer was the main cause of death in women (62%) and gynecologic tumors were the most common causes reported (breast cancer in 53.9% and ovarian cancer in 7.5%). Only 34.9% considered CVD as the main cause of death in women. There were no differences by age on this question.
DISCUSSION
The present survey shows an increase in self-reported CRF compared to the data obtained in the previous survey conducted by the Heart and Women Area in 2006. 8 These findings are in line with the results of the fourth NSRF. 7 A matter of concern is the increased prevalence of CRF in the female population at the expense of excess weight, HTN, DM, and ETC levels over the 15-year period. We observed several CRF in women > 45 years, in those with known CVD, and a combination of CRF in those who did not know they had CVD, thus increasing the cardiovascular risk (Figure 1). When HTN was analyzed, some women did not know their BP levels (12%) and another group of women (4.7%) who did not consider themselves to be hypertensive had elevated values (> 140 mm Hg), which demonstrates the lack of awareness of this important CRF. Something similar occurred with cholesterol levels: 29.2% were unaware of their values, and among those who recognized that they had ETC, 37% had not reached the therapeutic targets (<200 mg/dL) despite drug treatment or hygiene and dietary measures.
In the participating population the prevalence of a history of pregnancy was high (81.2%) and 26.9% reported complications. In line with previous series, a bad obstetric history was more commonly associated with HTN, DBT and future CVD (Figure 2). 3,5,9-11 The guidelines on cardiovascular prevention in women highlight the need for periodic cardiovascular monitoring in women with bad obstetric history due to the association with atherosclerotic CVD and CVD-related mortality. Reassessment of the cardiometabolic profile is recommended one year after the index pregnancy 12-15 to screen for HTN, DM and ETC and to encourage women to return to their pre-pregnancy weight. In the population surveyed, only 37% of the women with complications of pregnancy underwent cardiovascular monitoring one year later, which highlights that women and probably their health care professionals were not aware of this risk. Something similar occurred in patients with a history of cancer, as most of them (91.4%) had not been evaluated by a cardiologist during or after cancer treatment.
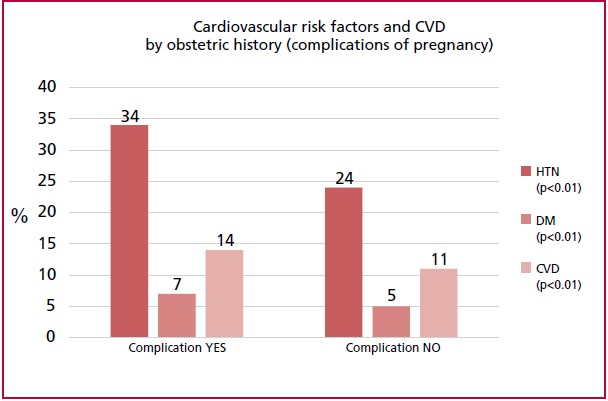
Fig. 2 Cardiovascular risk factors and cardiovascular disease (CVD) during follow-up according to obstetric history
The use of oral contraceptives was more common in young women (65% < 45 years) and the prevalence of HTN, ETC levels and excess weight was lower in those using oral contraceptives. As this treatment is prescribed by obstetricians and gynecologists, these results could be due to a selection of the method of contraception indicated, based on the woman's cardiometabolic risk profile.
Regarding smoking habits, the implementation of the anti-smoking law 26 687 in 2011 has had a favorable impact on smoking reduction. 16 In the current survey, 11.3% of the respondents smoked versus 29.3% in the previous survey in 2006, and these data agree with the fourth NRFS which showed a reduction in tobacco use. 7
Women tend to be less active, and, probably because of cultural issues, girls are less encouraged to engage in sports; in the population surveyed, there was a high proportion of sedentary women, particularly among those ≤45 years. This could be due to the fact that younger women play many roles and activities related to parenting, household chores and work activities, and have less time available to adhere to healthy guidelines. Women who exercised regularly had less excess weight, HTN, DBT and irritability, and better quality of sleep. Irritability (62.6%) and regular alcohol intake (56.5%) were also more common in young women.
The importance of sleep in the prevention of CVD has recently been recognized. 17-19) Fragmented sleep or sleeping less than 7 hours has been associated with subclinical atheromatosis in multiple territories and with increased cardiovascular morbidity and mortality. 20 In the population surveyed, 49.5% reported sleep disorders that were more common in those who drank alcohol, and in those with ETC levels and excess weight.
Cardiovascular disease was reported by 10.9% of the survey respondents and was more common in women > 55 years; myocardial infarction was the most common CVD. Women with CVD also had more associated comorbidities (HTN, DM) and excess weight.
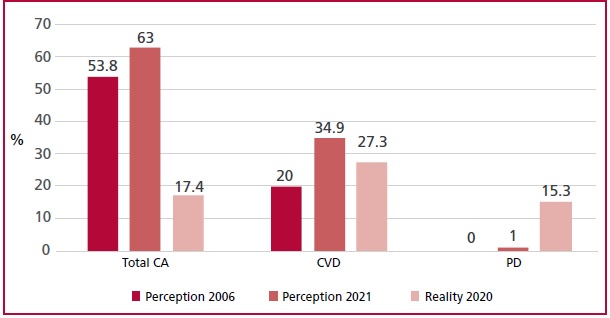
As for the cause of death, women still have the erroneous perception that cancer is the main etiology. In the previous survey conducted in 2006, 53.8% of women considered tumors as the main cause of death and only 20% considered CVD. Fifteen years later, the discrepancy between perception and reality persists, since 62% considered cancer and 34.9% considered CVD as the main cause of death, while according to the vital statistics published by the Ministry of Health in 2020, 21 17.4% of deaths were due to cancer and 27.3% to CVD (Figure 3). This discrepancy between perception and reality could be associated with the gynecologic cancer prevention campaigns carried out by the societies of gynecology of our country and, in some way, exposes the lack of effective communication by the cardiology community about CRF that have an impact on cardiovascular health and CVD.
CONCLUSION
Women's own perception of their risk is clearly low, and the data collected from the population surveyed suggests poor CRF control. Younger women show the greatest difficulty in the adherence to healthy behaviors, receive less counseling about their risk, and therefore constitute the most vulnerable population. Actions should be taken to spread the information and thus reduce the gap between perception and reality of CVD in women.
Study limitations
The non-probabilistic sampling design (social media/ WhatsApp/contacts) generates a response bias, with lower probability of participation of those women with less access to these resources and without contact with physicians in the SAC area. Although the survey was distributed nationwide by representatives of SAC regional districts, the lack of residency data does not allow us to know the representation of all the regions of Argentina. The distribution by social media did not allow us to corroborate participants' sex and age. As body measurements were collected by ranges, it was not possible to calculate excess weight by body mass index.

