











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
CPAP therapy is the first-line treatment of moderate and severe sleep apneas of obstructive mecha nisms (OSA)1-2. Its efficacy depends on the compliance and intolerance of multifactor origin, which are frequent in the initial phases of treatment3-7.
A multidisciplinary team is essential to contribute to the treatment with continuous positive airway pressure (CPAP) in patients with sleep-related breathing disease. Personalized care and a precision medicine approach determine that the treatment should take into account the preferences and indi vidual responses to treatment8-13.
Various studies show that health professionals other than physicians may have a broad and diverse role during follow-up and clinical management of patients with OSA or patients who require CPAP or noninvasive ventilation (NIV)8-12. The education of patients and treatment follow-up are important tasks in this regard10-12, as well as the identification and resolution of the main secondary effects3,12,13.
On the other hand, the CPAP devices record data that allow for the evaluation of the patients’ per formance by monitoring compliance, leaks, the level of therapeutic pressure and residual events. This is a useful way of evaluating efficacy with time and through different interventions8-14 and the devices are crucial to the identification of intolerance.
With the aim of knowing the level of compliance, the consultation profile, and causes of intolerance, we proposed to analyze the behaviors determined in a Sleep Unit through a specialized consultation unit conducted by physiotherapists.
Objectives
- To know the level of compliance, the causes of intolerance to CPAP treatment and the behaviors determined for its resolution.
Materials and Methods
Study Design
Observational, retrospective, cross-sectional study in only one center.
We reviewed systematically collected data of outpatient consultations between January 2016 and January 2020, obtained from a medical office specialized in CPAP adaptation and follow-up that belongs to the Sleep Unit of a community hospital.
This study was approved by the Institutional Review Board of the Hospital Británico (CRIHB, for its acronym in Spanish) in accordance with the ethical principles of the Declaration of Helsinki and successive amendments (CRIHB #1030 protocol, approved on 15 August, 2020).
Population
The study included OSA patients older than 18 years who were evaluated in the sleep medicine spe cialized consultation unit coordinated by a respiratory physiotherapist. Patients were referred for monitoring of CPAP treatment, education and training in the use of the device or demonstration of how to use the interfaces.
We took into account the consultation of patients without previous experience and also those who had completed the adaptation; also, patients diagnosed with obesity hypoventilation syndrome, periodic breathing and those requiring other modes of treatment with positive pressure (ventilation with two levels of pressure, servo-controlled ventilation).
During the daily physiotherapist consultation, the indication of CPAP therapy or noninvasive ven tilation given by the respective attending pulmonologists was kept the same with no modification or intervention, as usually happens in our Sleep Unit.
Patients who didn’t need positive pressure treatment or suffered another sleep-related, non-respi ratory disease were excluded.
Information regarding compliance, efficacy and tolerance to CPAP/NIV therapy
The baseline Apnea-Hypopnea Index (AHI) was obtained from the polysomnography (PSG) or respiratory polygraphy (RP) records, and the Body Mass Index (BMI) was registered from the sleep study reports.
We took into consideration the information received during the patients’ consultation with regard to: reason for consultation, duration of therapy, mean use and percentage of nights with > 4 hours’ use in the last 30 days, and intolerance events related to the devices told by each patient (pressure, auto-perceived leaks and humidification level of inhaled air).
Objective follow-up data were obtained from the information downloaded from the devices’ memory (SD Card) by means of the following software: Encore™ Pro II Philips-Respironics™, ResScan™ of ResMed™, ResSmart™ of BMC Medical™, or else by means of the online Air View™ platform (remote monitoring) of ResMed™.
We confirmed the masks that were used and the main adverse effects or lesions related to the in terfaces.
Information about the effective pressure was obtained from the visual analysis of the pressure/time curve. When available, data regarding compliance, mean leaks and residual apnea-hypopnea index (rAHI) were registered in events per hour (ev/h).
Statistical Analysis
Data were presented as percentages of the categorical variables. Continuous variables with normal distribution are expressed as number and percentage (n; %) or mean and standard deviation; and variables without normal distribution are expressed as median and percentile (25-75%).
For the comparison of differences, we used the Mann-Whitney or Fisher tests or χ2, depending on the type of variables. For the comparison of different therapy pressures, we carried out a linear regression analysis. For the statistical analysis we used Graph Pad Prism-8.02™ software.
Results
244 patients were evaluated in 388 visits for four years. 165 patients were men (67%); age, 65.7 ± 11.6 years, BMI (kg/m2) 31.0 ± 5.4. Table 1 summarizes the characteristics of the study population.
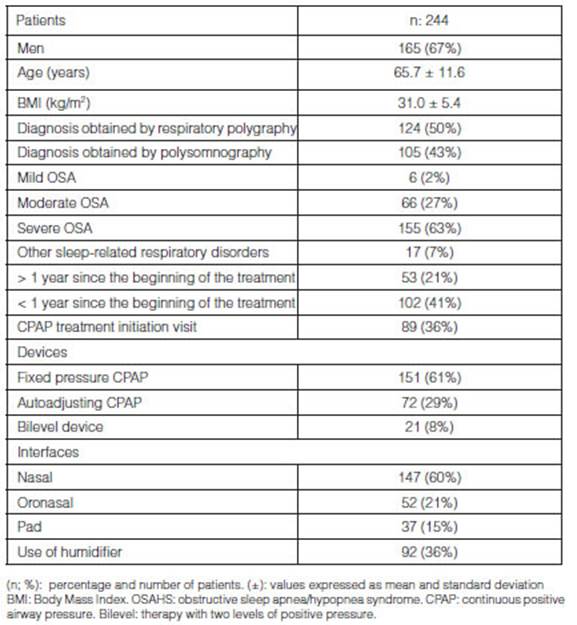
The diagnosis was established by polysomnography (43%), home respiratory polygraphy (50%) or both (6%). Six patients showed mild OSA (2%), 66 (27%) had moderate OSA and there were 155 cases (63%) of severe OSA. 7% were respiratory sleep-related diseases other than OSA.
At the moment of the consultation, 61% of patients used fixed pressure CPAP, 29% auto-adjusting CPAP and 8% bilevel devices. At the moment of the evaluation, 147 patients used nasal masks (60%); 52 oronasal masks (21%); 37 pads (15%), and 92 patients (36%) used thermohumidification systems.
53 (21%) patients had undergone more than 1 year of treatment with positive pressure devices; less than one year, 102 patients (41%); and 89 patients started treatment with kinesiological support (36%).
After analyzing the visits (more than one per patient), we found out that the reasons for consulta tion were mainly therapy control (239; 61%), intolerance (67; 17%) and CPAP calibration (51; 13%). Table 2 shows the reasons for referral and initial consultation.

Compliance with positive pressure treatment (hours/night) was 4.6 ± 2.1, with a proportion of nights > 4 hours of use for 30 days before consultation of 67 ± 36%. 94 patients (38%) showed compliance with > 75% of the nights. (Table 3)

Table 3 Data of therapy and compliance as from the download of software in the devices (built-in software)
We didn’t find any difference in compliance when comparing the first and second year of CPAP use (4.5 vs. 5.0 hours/night) p > 0.13 (Figure 1). However, the percentage of nights using the device > 4 hours was higher relating to longer duration of therapy, evidencing this difference 600 days after start ing the treatment (Figure 2) p < 0.05.

Figure 1 Compliance ≥ 4 hours/night regarding duration of treatment with positive pressure (< 1 vs. ≥ 1 year).

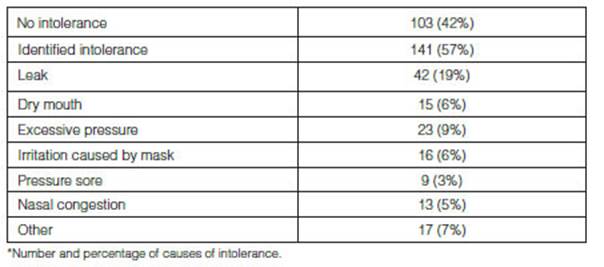
141 patients (57%) showed intolerance, most frequently leaks (42; 19%) and events related to the mask or thermohumidification (Table 4andFigure 3). In 138 cases (97%), the intolerance could be identified and resolved during the kinesiological consultation.

Within the group with > 1 year of treatment (n; 53), 36 patients showed intolerance (67%), though 34 (64%) complied with the therapy more than 4 hours/night and 30 (56%) complied with > 4 hours of use, > 75% of the nights, within 30 days before consultation. (Table 5)

Finally, 194 behaviors were determined for the resolution of intolerance events detailed in Table 6.

Discussion
This work exposes the complexity of OSA patients’ follow-up during treatment with positive airway pressure.
In our population, one third of patients with CPAP required interventions related to the device or the mask, or needed guidance to follow the treatment, or solve the intolerance or the treatment’s adverse effects.
In OSA patients who are in the adjustment or follow-up phase, the work model of our unit takes into account the participation of the respiratory physiotherapist with bi-directional referral to and from the pulmonologist. Mid-term follow-up (the first six months) is the period in which the main second ary effects are produced, which, if adequately resolved, determine success in terms of acceptance and maintenance of therapy in the long-term12. The role of the non-medical staff at the Sleep Unit may be a control point in the semiology of the patient and his/her equipment, and include sleep lab technicians, nurses and physiotherapists.
In this cohort of patients, compliance was acceptable (near 70%), with a mean use > 4 hours/night similar to that described in other works, both national and international16-20. However, thanks to specialized consultations it was possible to identify frequent events of intolerance and create positive feed-back that lets the patient and the attending staff interact in order to solve them3.
The most predominant reason for consultation was referral for treatment adherence control. Objec tive data about compliance are fundamental for making decisions during follow-up11-14; but the clinical evaluation allowed for the identification of intolerance events, a predictive factor for treatment with drawal, even in patients who consulted about daily data download from the device.
It has been suggested that in our country the poor contact with the reference hospital complicates CPAP treatment continuity21. There is low quality preliminary evidence regarding the granting of equipment, thus the monitoring clinical work is hierarchically organized in reference units22.
Also, other frequent clinical problems were identified: allergic or irritable rhinitis, insomnia and bad sleep hygiene, which motivated referrals to the respective attending physicians, ensuring multi disciplinary work3,12,13.
Published data exposed the fact that the first 2-4 weeks after the start of treatment with positive pressure are crucial for favoring adherence, since it is during this period that intolerance is frequently identified3. However, we could identify lower adherence in patients with > 1 year of CPAP (tradition ally considered as adapted to therapy), as described by Morrone et al, who showed 67% compliance > 5 hours/night after 1-year follow-up in a protocolized environment15. Surprisingly, in this series, the differences in the compliance profile could be seen after 600 nights of treatment, exposing the need to continue follow-up and analysis of intolerance beyond the first year.
Procedures during the stages of adaptation, titration, and monitoring of compliance and efficacy of positive pressure require specific instruments3,14 (software management, knowledge of different therapy devices, use of masks, knowledge of cognitive-behavioral strategies, understanding of sleep question naires, standardized clinical behavioral protocols, etc.), which turn the kinesiological consultation into a current discipline that is part of those conforming the multidisciplinary team that must offer solutions for OSA and related disorders23.
Finally, our work is retrospective and includes the typical limitations of this type of design. Also, attendance to this model of specific consultation depends on medical referral, representing a bias and a limitation that complicates interpretation and doesn’t allow the extrapolation of results to other systems of organization.
Conclusions
Two thirds of OSA patients evaluated in a clinical interview by physiotherapists use positive pressure more than 4 hours per night, and half of the patients show intolerance even after the period of adaptation.
The specialized kinesiological consultation may contribute to the identification and resolution of difficulties, applying a protocol based on education and training, interface selection and mid- and long-term follow-up.

