











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
It is known that mechanical ventilation (MV) produces per se injuries in the pulmonary fibrous skeleton.1 This damage is associated with lung compliance resistance, and the adjustment of tidal volume (TV), inspiratory flow, PEEP level and respiratory rate (RR); the latter being related to the amount of times the lung is subjected to an abnormal breathing pattern per unit of time,2 generating an inflammatory process with positive feedback (ventilator-induced lung injury vortex [VILI Vortex]).3,4
The status asthmaticus (SA) is developed with high airway pressures, where the resistance ele ment is the most important one. Even though the driving pressure (DP) is not a problem, baro trauma is also developed. In order to control the consequences of the reduction in T V and RR (hypercapnia and respiratory acidosis), an extra corporeal CO2 remover is added (ECCO2R), which achieves decarboxylation using low blood flow and low sweep flow.5-7
The mechanical power (MP) is divided into its three components, and the magnitude of the “resistive power” is described as being the one re sponsible for the MP. The reduction of the RR and TV interrupts the dynamic hyperinflation cycle, thus reducing intrathoracic pressure, correcting acidosis, allowing for the attenuation of hypoxic pulmonary vasoconstriction (HPV) and reducing the postload of the right ventricle.
We present the case of an asthmatic patient with life-threatening risk who evolved with refractory hypercapnia, mixed acidosis with blood hyperten sion and barotrauma, and was treated with arte riovenous ECCO2R (Novalung®).
CASE REPORT
20-year-old male with known asthma who arrived at the Emergency Service (ES) of the regional hos pital of Antofagasta; he had been referred from To copilla. He complained of breathing difficulty one day before admission. Then he showed tachypnea (30 rpm), with circumoral cyanosis and respiratory muscle fatigue. Due to this condition, he received orotracheal intubation and was subjected to MV deeply sedated and with neuromuscular blockade. He received norepinephrine due to the hemody namic compromise.
He was admitted to the emergency service with an APACHE II score of 11 points. MV was first delivered via volume-controlled mode with a TV of 350 mL, RR 24, I:E ratio = 1:3, PEEP 3 cmH2O (intrinsic PEEP = 18 cmH2O) and FiO2 of 50%. The patient showed high inspiratory pressure (90 cmH2O), so nebulization with salbutamol and Berodual® (fenoterol 0.25mg/mL + ipratropium bromide 0.5 mg/mL) was intensified. The aus cultation revealed a bilateral decrease in breath sounds, with generalized wheezing. Respiratory monitoring showed a plateau pressure (Pplat) of 17 cmH2O and a static compliance of 30 mL/ cmH2O. Initial arterial blood gases: pH = 7.18, PCO2 = 50.5 mm/Hg, PaO2 = 89.3 mmHg, HCO3 = 18.2 mEq/L. Negative PCR test for COVID-19.
At the ICU, the patient continued with severe bronchospasm, desaturation up to 63% with in creasing doses of noradrenaline (from 0.06 μg/kg/ min to 0.2 μg/kg/min) and hypothermia tendency. Control tests showed lactic acidosis (10.2 mMol/L) with pH of 7.17 and HCO3 of 18 mEq/L. On the third day, the subject had palpable cervical crack ling sounds, and the chest scan showed cervical subcutaneous emphysema and pneumothorax (Figure 1). Thus, a pleural tube was placed and the ventilatory schedule was modified. Methylprednisolone boluses were included (500 mg x three times). The TV was reduced to 3.4 mL/kg of predicted body weight, RR was reduced to 10 rpm, inspiratory time to 0.72 s, minute ventilation (VE) to 2.6 L/min and the I:E ratio to 1:7, without PEEP. With this pattern, the Pmax decreased to 48 cmH2O and the iPEEP reached 6 cmH2O. Due to the hypercapnia, it was associated with arte riovenous ECCO2R (Novalung®). Aminophylline was included. No fever or evidence of septic focus detected.

Figure 1 Presence of barotrauma most probably by high pcak pressures of the airway secondary to severe bronchial obstruction, before being connected to Novalung® and using ultra protective MV. This damage was produced despite the use of a TV of 6 mL/ kg of ideal body weight and low levels of positive end-expiratory pressure (PEEP).
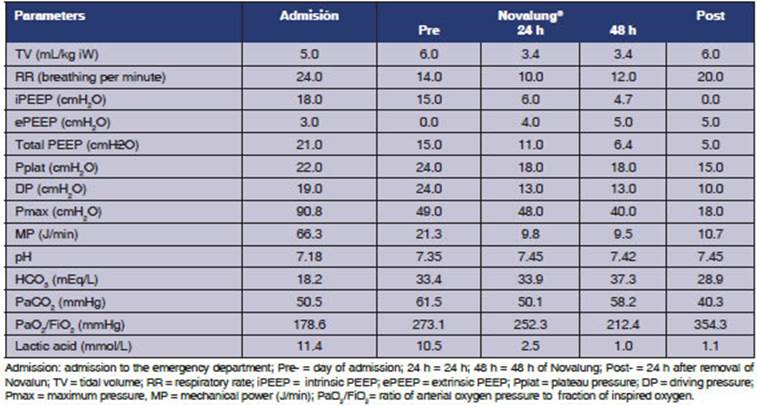
Once the patient was connected to Novalung®, we applied the volume-controlled mode with a TV of 300 ml and a RR of 10 rpm. The Novalung® blood flow was maintained between 1.2 L/min and 1.6 L/min, and the sweep flow was adjusted between 6 L/min and 7 L/min. Table 1 shows the PaO2/FiO2 ratio, the PaCO2 and pH on the day the Novalung® device was connected. Twenty-four hours after being connected to Novalung®, the maximum pressure (Pmax) of the airways was reduced and oxygenation remained unaffected. The most important modifications were a drop in the iPEEP and Pmax (Figure 1).
The patient remained connected to Novalung® for ten days and showed good evolution. 72 h after removing the Novalung® device, the patient was extubated. Ventilatory parameters before extuba tion: Pplat = 15 cmH2O; DP = 10 cmH2O; Pmax = 18 cmH2O and MP of 10 J/min, without iPEEP. Gasometric parameters: pH = 7.44, PaCO2 = 39.6 mmHg, PaO2 = 71.9 mmHg. Give the patient’s stability, he was discharged from the ICU 120 h after extubation, having solved the bronchospasm.
DISCUSSION
The most important finding was to identify the resistive mechanical power as the leading cause of barotrauma in a patient with SA. A significant correlation was observed between the iPEEP and Pmax of the airway. Both decreased drastically when we were able to reduce the RR and TV and extend the expiratory time (I:E ratio = 1:7) after installing the Novalung® device.
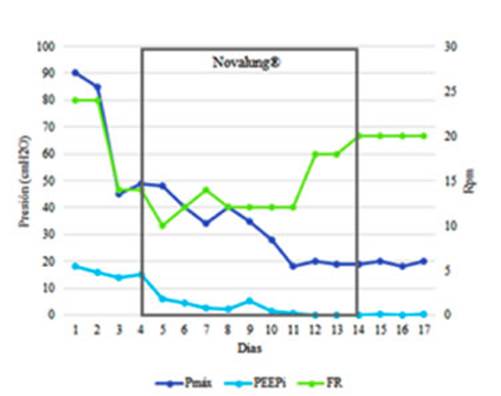
Graphic 1 drastic Pmax decrease when reducing the RR after controlling the PaCO2 with ECCOR Novalung®. Time of use of Novalung® shown in grey.
After introducing this device, the RR could be reduced from 24 rpm to 10 rpm. Thus, the iPEEP was reduced from 15 cmH2O to 6 cmH2O. This change reduced pulmonary hyperinflation and probably reduced the intrathoracic pressure, im proving venous return and cardiac output; this was reflected in the improvement of clinical perfusion, diuresis, and the correction of lactic acid. Acidosis control should reduce the HPV and postload of the right ventricle8 (Table 1).
When we analyzed the specific components of the MP, such as the static elastic power (associated with PEEP), the dynamic elastic power (associ ated with TV) and the “resistive power” (native airway), we observed that the drop in the MP was caused mainly by the reduction of the resistive component, theoretically the most important one in status asthmaticus. In our case, this component reached more than 80% of the total MP on the first day (Figure 2).
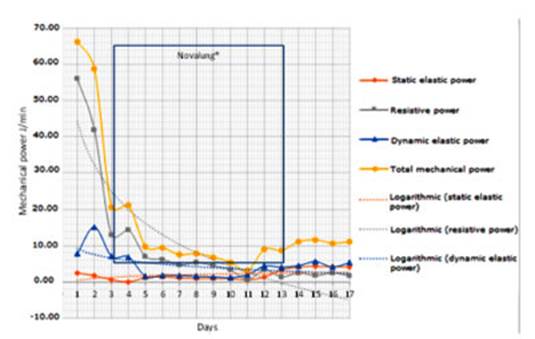
Graphic 2 representation of the three components of mechanical power in relation to itself and its respective logarithm tendencies. A significant decrease in resistive power (grey line) after beginning with Novalung® (framed in blue).
When the exhalation of gas is incomplete be cause the next inspiration begins before the lung is completely empty, air trapping occurs and the expiratory time constant (τ) may reach values near 0.9 s.9 For that reason, the expiratory time must be extended. The reduction of the TV and RR also reduced the minute ventilation (VE), which is the main cause of dynamic hyperinflation.9 Twenty-four hours after the installation of the Novalung® device, we observed the impact that the reduction in the RR and the TV had on the “resistive power”, which decreased from 58 J/min to 14.6 J/min.
These patients often show increased respira tory effort and are dehydrated, and develop lactic acidosis, worsening respiratory acidosis. All these elements were present in our patient on admission, so he received crystalloids, norepinephrine and low levels of PEEP (Table 1).
The MP considers all the elements to be in cluded in the Otis equation. The DP and RR are the most aggressive for the pulmonary fibrous skeleton.10 On the other hand, the peak flow is also an important variable for the development of alveolar epithelial damage (Figure 3). There fore, the decrease in the inspiratory flow avoids the disruption of the respiratory epithelium. This phenomenon has been shown in an in vitro model of Tschumperlin.11 In our patient, as a consequence of the reduction in the RR, the expiratory and in spiratory time could be simultaneously extended and so the peak flow could be reduced.

Graphic 3 Despite the use of Novalung® (framed in blue), ultra-protective TVs were achieved. Also the RR was reduced, and so the peak inspiratory flow decreased.
The impact of the MP has been studied in rela tion to the acute respiratory distress syndrome (ARDS), but there aren’t enough studies that re late it to asthmatic decompensation.12-14 However, regardless of the specific damage patterns, the dynamic elastic power (ARDS) or resistive power (status asthmaticus), the mechanical power is inevitably transferred to the pulmonary fibrous skeleton in each mechanical cycle.
The resistive component of the MP must always be analyzed in patients with airway obstruction. When analyzing the components separately, the resistive component (grey line) clearly stands out as the main MP generator in this type of patients (Figure 2).
CONCLUSION
In short, when patients evolve with high airway pressures, despite the existence of a suitable plateau pressure, we must consider the resistive component of the MP as the origin of barotrauma (bronchial obstruction). Through simple formulas we can predict the impact of mechanical ventilator variables on asthmatic patients.10 The ECCO2R systems are a safe tool to be associated with ultra-protective MV in severe asthmatic patients.

