Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
The use of the high-flow nasal cannula (HFNC) increased during the COVID-19 pandemic due to the high demand from patients with acute respira tory failure (ARF).
The use of high-flow oxygen therapy was a point of controversy among major critical care medical societies worldwide during the COVID-19 pan demic, especially due to concerns regarding the safety of the healthcare personnel and the delay in starting therapy.1
Therefore, the therapeutic measures tradition ally implemented to counteract COVID-19-related hypoxemia have included conventional oxygen therapy and invasive mechanical ventilation.
The use of oxygen (O2) through a conventional oxygen therapy mask has long been the first-line therapy for patients with acute respiratory failure (ARF).
However, this strategy is far from ideal because conventional oxygen therapy does not reduce respiratory effort or improve alveolar ventilation.
On the other hand, the gas delivered by conven tional devices is dry and cold, which can irritate the airways, disrupt mucociliary clearance, and cause discomfort to the patient.2
The use of the HFNC allows for improved oxy genation through various mechanisms, such as a reduction in the dilution of the oxygen administered with ambient air,3,4 a decrease in dead space,4,5 an in crease in circulating volume,5,6 and the generation of positive airway pressure (CPAP),6-8 resulting in a reduction of respiratory effort and respiratory rate.6-10
The use of the HFNC allows for the delivery of a gas flow of up to 60 L/min through silicone nasal cannulas, with the supplied gas conditioned to ideal temperature and humidity levels (37°C and 100 % relative humidity).
Several studies have demonstrated that us ing flow rates between 35 and 60 L/min results in mean expiratory pressures at the pharyngeal level of 2-3 cmH2O with the mouth open and 5-7 cmH2O with the mouth closed.11-12 Furthermore, it has been shown that the use of the HFNC in creases lung impedance at the end of expiration,5,6 a parameter correlated with lung volume. Alveolar recruitment is optimized,13 due to increased airway pressures.
Considering the positive outcomes observed with the early application of the HFNC in patients with moderate to severe COVID-19 pneumonia,14,15 and using the IROX index16,17 as a predictor of suc cess, this retrospective observational study aims to establish an objective relationship between treatment success and failure with the analyzed variables, offering a robust tool for managing the disease.
Faced with the high mortality observed during the first wave of the pandemic, there arose a need for more efficient approaches to treat hypoxemia in COVID-19 patients.18,19
The primary objective of this study is to deter mine whether the HFNC avoids orotracheal intu bation. As secondary objectives, the study aims to analyze whether the initial IROX, the IROX at 12 hours, the Delta IROX during the first 12 hours, and the start of HFNC treatment from the onset of symptoms serve as predictors of treatment success.
MATERIALS AND METHODS
Designs
This is a retrospective and descriptive study of patients attended at the Hospital Central, a regional hospital in the region of Cuyo, Argentina, who were admitted to the Emergency Department and Covid Intensive Care Unit.
The ARF is the inability of the respiratory system to fulfill its basic function, which is the gaseous exchange of oxygen and carbon dioxide between ambient air and circulating blood; with the presence of arterial hypoxemia (PaO2 below 60 mmHg), at rest, at sea level, and breathing ambient air, with or without hypercapnia (PaCO2 above 45 mmHg). We will refer to hypoxemia only in cases where the PaO2 is between 60 and 80 mmHg. With pulse oximetry, oxygen saturation values of 90 % to 95 % can be considered equivalent to a PaO2 of 60 to 80 mmHg (hypoxemia), and if they are 90 %, they are equivalent to a PaO2 of 60 mmHg (respiratory failure).21
The HFNC is a non-invasive respiratory support de signed to deliver flows between 30-60 L/min. It works by mixing air and oxygen, humidified and heated through a nasal cannula specifically designed for these therapeutics.2
The IROX is a variable used to evaluate the success or failure of a high-flow nasal cannula for respiratory failure; it is the ROX index (IROX) that combines oxygenation (SpO2/ FiO2) and respiratory work (RR). Its validity in COVID-19 pneumonia has a high sensitivity for predicting therapy failure and is associated with high mortality (45.4 %).16,17
The diagnosis of Covid-19 was made by nasopharyn geal swabbing by the on-call laboratory staff and referred to the molecular biology service of the Hospital Central, where the sample was analyzed by PCR (polymerase chain reaction through viral RNA) with the Schep SARS-CoV-2 Multi-FAST Kit.
Sample
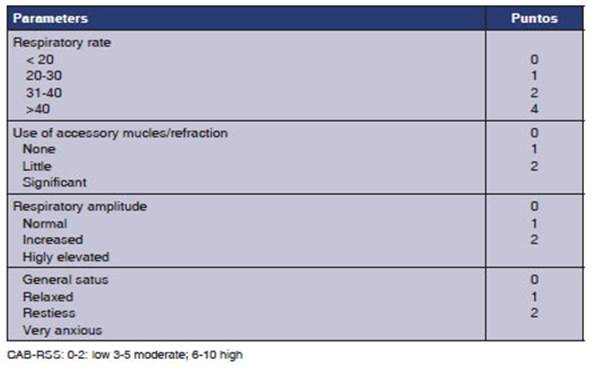
In the period between October 2020 and March 2021, with confirmed Covid 19 and suspicious symptoms. The sample included patients older than 15 years, and collaborators who tolerate the device and follow the operator’s indica tions within their psychophysical limitations. The Cabrini Respiratory Strain Scale (CAB-RSS) (Annex 1) was used as a guide for orotracheal intubation criteria with a CAB-RSS score of 3 to 5; patients without orotracheal intuba tion criteria, with poor clinical prognosis for intubation and confirmed diagnosis of COVID-19 by rapid test or nasopharyngeal swab. Patients with criteria of imminent need for OTI (orotracheal intubation) and CAB-RSS scale of less than 2 or greater than 6 were excluded.
Variables
In patients who met the inclusion criteria, the following variables were analyzed during the first 24 hours: age, sex, comorbidities, initial IROX, and IROX at 1, 2, 4, 6, 12 hours after starting treatment with HFNC, success or failure of treatment in relation to the days elapsed between the date of symptom onset and the start of treatment with the high-flow nasal cannula.
The data were collected in individual patient spread sheets and shared by means of a drive between on-call kinesiologists in each area from Monday to Sunday, and then analyzed using the Access program.
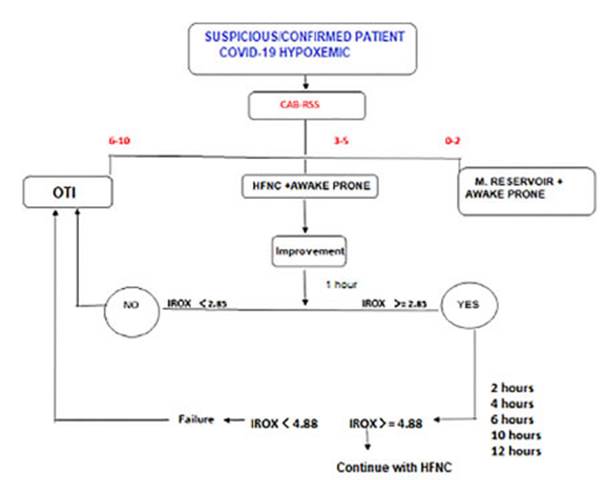
On admission, the patient was clinically evaluated with the CAB-RSS scale; if he/she showed signs of hypoxemia and a score of up to 2 on this scale, conventional oxygen therapy was continued with eventual prone decubitus positioning. If the CAB-RSS score was between 3 and 5, the HFNC was placed and the patient was put in prone decubitus position. After the placement of the HFNC and eventual change of decubitus, clinical signs were evaluated thoroughly during the first 12 hours with IROX. If the IROX was equal to or lower than 2.85 in the first place, it suggested OTI; if the IROX was equal to or higher than 3.85, treatment was continued and evaluations were performed in the following hours. If IROX was lower than 4.88 at 6 hours after initia tion, it was considered as treatment failure; and if it was higher, treatment was continued (Figure 1).
Monitoring HFNC placement in patients was performed through the ROX index (IROX), which is defined as the ratio between pulse oximetry/ fraction of inspired oxygen (SpO2 /FiO2) and respiratory rate (RR). Roca et al20 identi fied patients at high risk of HFNC failure when this index was < 4.88 at 12 hours. The cutoff values were different, as were the cutoff times for predicting failure. A recent meta-analysis was able to evidence in the subgroup using an IROX > 5 greater discriminatory accuracy in predicting failures compared to a cutoff value ≤ 5. 17
HFNC treatment was started with high flows of 50-60 L/min, adjusting the FiO2 to maintain the SpO2 between 92 %-96 %. The temperature was automatically regulated by the equipment. Patients were put in prone decubitus position from the beginning, and were alternated with lateral decubitus positions depending on their tolerance. Patients were monitored by noninvasive measurement of heart rate and blood pressure, oxygen saturation and respiratory rate. The FiO2 was gradually reduced while maintaining the target SpO2. The flow was also decreased gradually depending on patient tolerance and respiratory rate reduction.
The failure of the HFNC is defined as the escalation to invasive mechanical ventilation (IMV) or death. Standard indications for orotracheal intubation (OTI) included the following: respiratory rate (RR) of more than 35 breaths/ min, obvious activity of accessory respiratory muscles or paradoxical abdominal breathing, progressively increase of PaCO2, hemodynamic instability, and inability to protect the airways or inability to obtain saturation above 93 % with a FiO2 of more than 80 %.
For the implementation of the HFNC, a patient interface was used, which consisted of a flexible nasal cannula ins tead of face masks, allowing the patient to be independent in functions such as eating, drinking, talking and sleeping easily without interrupting therapy, and is available in several sizes adapted according to the patient’s anatomy (AquaNaseE); high flow and precise O2 system allowing to deliver a flow between 0 to 60 L/min and FIO2 from 21 % to 100 % (Neumovent tecme TS, Leistung Luft 3, R203P14, R219P86), humidifierheater system with or without tempe rature control (Fisher&paykel, AquaVENT AMHH2600A), non-condensing tubing (Armstrong Medical AquaVent).
Statistical analysis
For the statistical analysis we had the IBM SPSS software platform, which was used by a professional external to the study. The results are presented for categorical variables such as count and their proportion within the category. Numerical variables, whether they are continuous or discrete, are observed as appropriate to their distribution, such as mean and standard deviation or median and inter quartile range.
To compare the association between categorical varia bles, we used the Student’s t-test or Mann-Whitney U test for numerical variables depending on their distribution. For non-parametric variables, we used the Kolmogorov- Smirnov test. The chi-squared test was used for comparing qualitative variables. A value of p < 0.05 in two-tailed tests was considered to be statistically significant.
RESULTS
A total of 154 patients were reviewed, and a sample of 72 patients who had been consecutively selected and had completed the data collection form was included. 82 patients were excluded due to miss ing data (Figure 2). 50 % of the patients avoided orotracheal intubation. The population’s charac teristics are presented in Table 1.

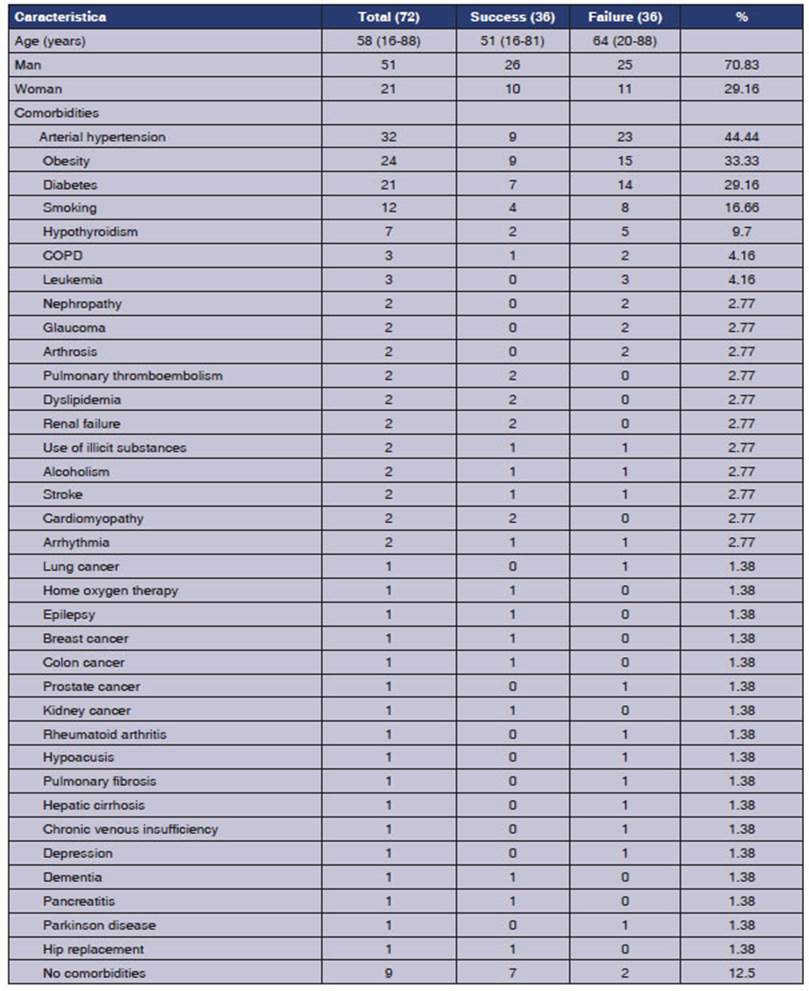
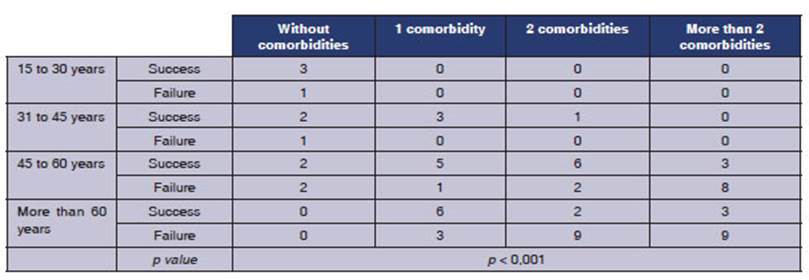
It was observed in the group of patients that those who experienced failure were older adults with two or more comorbidities, with a significant p-value of p < 0.001 (Table 2).
The initial IROX is significantly different be tween both groups, with a mean of 7.10 (95 % CI 6.41-7.79), a median of 6.78, and a standard devia tion of 2.94. The comparison of the initial IROX between the success group and the failure group yielded a mean ± of 6.24 ± 2.32, with a p-value of 0.006 (Figure 3).
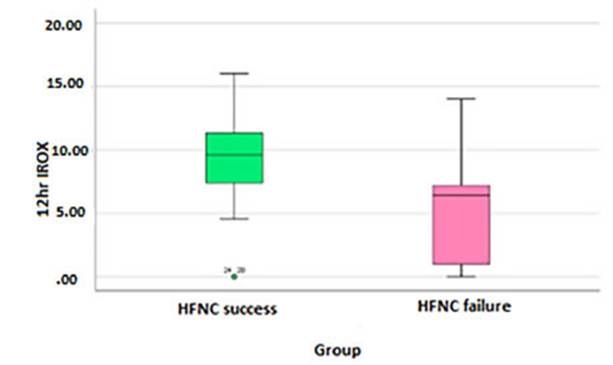
The IROX score at 12hr is significantly different between both groups, with a mean of 7.26 (95 % CI 6.25-8.27), a median of 7.18, and a standard deviation of 4.29 with a p < 0.001 (Figure 4).

The time elapsed between symptom onset (SO) and the start of the HFNC doesn’t have a statis tically significant relationship with a p-value of 0.133, mean of 8.76 (95 % CI 7.47-10.05), a median of 8 and a standard deviation of 5.254. (Graph 3).
The Delta IROX (initial IROX/IROX at 12hr) wasn’t statistically significant with a p-value of 0.092, mean value of 0.16 (95 % CI 0.76-1.07), a median of 1.19 and a standard deviation of 3.9 (Figure 5).
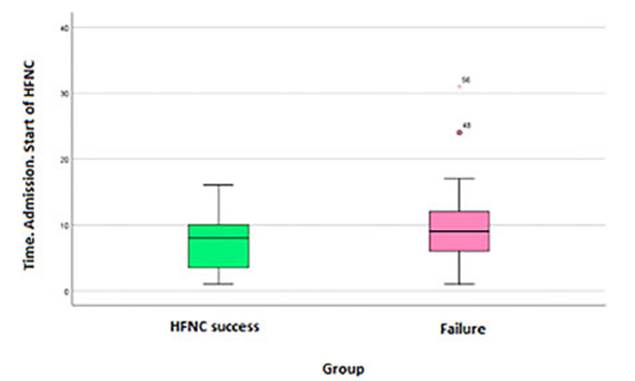
Figure 5 Relationship of symptom onset and start of HFNC between the success group and failure group.

DISCUSSION
After several months of the pandemic, a high mortality rate was observed in patients who were under invasive ventilation; early intubation in COVID-19 is not correlated with a favorable prog nosis, as noted by Plotnikow et al18 and Farkas et al.19 The use of the HFNC reduces the need for early intubation in adult patients with acute respiratory failure. This helps to prevent the as sociated risks of invasive mechanical ventilation, such as delirium, cognitive decline, ICU-acquired weakness, and secondary infections.
High-flow oxygen therapy through the HFNC is an innovative technique that combines O2 and compressed air, allowing the delivery of high con centrations of O2 at flow rates exceeding the peak inspiratory flow in patients with high ventilatory demands.
This oxygenation strategy is particularly com fortable for the patient due to the nasal cannula that provides humidified and warm gas, similar to physiological conditions. It also allows functional independence for activities like oral feeding, com municating, sitting up, and changing decubitus position without complications, as noted by Mel lado-Artigas et al.21
The IROX has been suggested as a tool to predict the outcome of the HFNC in patients with ARF. In the initial phase (within the first hour of HFNC treatment), we have demonstrated that the IROX is capable of distinguishing between the success and failure of HFNC treatment in COVID-19 patients, but not with the threshold value sug gested by Roca et al,9 since we have shown better prediction accuracy with a higher threshold value.
The time elapsed between the SO and the start of the HFNC treatment was not found to be sig nificant. This data may reflect a direct relation ship with a lower severity index at the beginning of treatment. The average IROX in patients who started HFNC treatment late (after 10 days). The success or failure of treatment could be related to the initial level of hypoxemia and respiratory mechanics involvement, regardless of the number of days since symptom onset.
Older adults, defined as those aged 60 years or older with two or more comorbidities, accounted for half of the total failures. This information is useful for hospital management, so that HFNC can be used with critical care units or units nearby for older patients, and in regular wards or peripheral hospitals in the case of the other group of patients.
Limitations
In the first place, this is a retrospective analysis, but it was based on prospectively collected data. Due to the retrospective nature, the standard ization of intubation was not decided a priori. Furthermore, it’s a single-center study, which means we cannot compare different population characteristics in the same region. Additionally, these results cannot be extrapolated to other non- SARS-CoV-2-related conditions that also cause acute respiratory failure due to a lack of evidence.
CONCLUSION
Our work demonstrates that the HFNC is a valu able tool for avoiding orotracheal intubation in patients with ARF caused by SARS-CoV-2 pneu monia.
The initial IROX and the IROX at 12 hours are predictors of the therapy’s success.
It would be interesting to investigate the value of this method in other etiologies of ARF.