










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.23 no.3 Buenos Aires Dec. 2010
ARTÍCULOS ORIGINALES
Relationship between overweight-obesity and periodontal disease in Mexico
Jorge A. Zermeño-Ibarra1, Soledad Delgado-Pastrana1, Nuria Patiño-Marín2, Juan P. Loyola-Rodríguez3
1Department of Periodontics.
2Laboratory of Clinical Investigation.
3Laboratory of Molecular Biology and Oral Microbiology. Faculty of Dentistry, Autonomous University of San Luis Potosí, México.
CORRESPONDENCE Dra. Nuria Patino-Marin. Laboratorio de Investigacion Clinica. Facultad de Estomatologia. Universidad Autonoma de San Luis Potosi. Mexico. Fuente de la selva 166. Col. Balcones del Valle CP 78280 San Luis Potosi SLP, Mexico. E-mail: nuriapaty@uaslp.mx
ABSTRACT
The aim of this study was to examine the association between overweight-obesity and periodontal disease in subjects who attended the clinic of Periodontics, Faculty of Dentistry, San Luis de Potosi, Mexico. This was cross-sectional study involving 88 subjects – 60 without overweight-obesity and 28 with overweight-obesity. The following clinical parameters were evaluated: dental bacterial plaque, index of calculus, gingivitis, probing depth and periodontal disease index (PDI). When comparing the group of subjects with overweight-obesity to the control, there were statistically significant differences in the variables calculus (p=0.0015), gingivitis (p=0.0050) and periodontal disease (p=0.0154). Regarding the logistic regression analysis, the dependent variable was subjects with and without overweight-obesity and the independent variables were sex, age and periodontal disease. We found statistically significant differences (p=0.0162) with OR=3.16 in periodontal disease. Periodontal disease showed statistically significant differences in the group of subjects with overweight-obesity. The oral health of subjects with overweight- obesity should be supervised and checked in order to prevent oral alterations.
Key words: Overweight; Obesity; Periodontitis.
RESUMEN
Relación entre sobrepeso-obesidad y enfermedad periodontal en México
El objetivo fue asociar el sobrepeso-obesidad con la enfermedad periodontal en sujetos que asistieron a la clinica de Periodoncia de la Facultad de Estomatologia de la Universidad Autonoma de San Luis Potosi (UASLP) Mexico. Se realizo un estudio transversal con un total de 88 sujetos, 60 con sobrepeso-obesidad y 28 sin sobrepeso-obesidad. Los siguientes parametros clinicos fueron evaluados en el estudio: placa dentobacteriana, indice de calculo, profundidad de bolsa y enfermedad periodontal (PDI). Al comparar el grupo de sujetos con sobrepeso-obesidad con el control se encontraron diferencias estadisticamente significativas en las variables calculo (p=0.0015), gingivitis (p=0.0050) y enfermedad periodontal (p=0.0154). En relacion con el analisis de regresion logistica, la variable dependiente fue sujetos sin y con sobrepeso-obesidad y las independientes fueron: sexo, edad y enfermedad periodontal. Encontramos diferencias estadisticamente significativa (p=0.0162) con un OR=3.16 en enfermedad periodontal. La enfermedad periodontal mostro diferencias al comparar el grupo de sujetos con sobrepeso-obesidad con el control. Es necesario la prevencion, supervision y revision del estado de salud bucal de los pacientes con sobrepeso y obesidad para prevenir alteraciones bucales.
Palabras claves: Sobrepeso; Obesidad; Periodontitis.
INTRODUCTION
Obesity is defined by some authors as excess body fat in relation to lean body mass, which alters the subject’s health. Body Mass Index (BMI), defined as a subject’s weight in kilograms divided by the square of the subject’s height expressed in meters, is considered to be the most frequent measure of body fat. The World Health Organization (WHO) and the National Heart, Lung and Blood Institute (NHLBI) define overweight as BMI 25 to 29.9 and obesity as BMI ≥ 301,2. Waist circumference is also an indicator used to evaluate visceral abdominal fat. Excess waist fat is considered to be ≥ 88 cm for women and ≥ 102 cm for men. Prevalence of obesity has increased over a relatively short time2,3, doubling in adults and tripling in children and teenagers. Thirty-one percent (59 million) of US adults are obese and over 65% report BMI ≥ 25. Furthermore, 15.8% of children (6 to 11 years old) and l6.1% of teenagers (12 to 19 years) are obese. The United States are considered to reflect international prevalence of obesity and overweight, with the exception of Africa1. In Mexico, the National Survey on Health and Nutrition (Encuesta Nacional de Salud y Nutricion, ENSANUT 2006) reported that national prevalence of overweight and obesity among children aged 5 to 11 years was 26% for both sexes. Prevalence among adults was 71.9% in women over 20 years of age (population: 24,910,507 women in the country) and 66.7% among men (16,231,820 men)4. Predisposition to obesity is probably related to genetic, immunological, psychological, environmental and socioeconomic factors, and metabolic, nutritional (diet) and sedentary lifestyle characteristics, among others. An association between obesity and inflammation has been reported. Adipose tissue is a complex, metabolically active endocrine organ that excretes immunomodulating factors that play a part in regulating vascular and metabolic processes, associated to alterations such as high blood pressure, cardiovascular disease, osteoarthritis, respiratory disorders, diseases of the gall bladder, non-alcoholic fatty liver disease, hyperlipidemia, atherosclerosis, stroke, increased risk of cancer (colon, endometrium, prostate and breast), pancreatitis, hepatitis and diabetes mellitus1,2,5, reducing quality of life and associated to mortality. Flegal’s National Health and Nutrition Examination Survey reported 111,909 excess deaths in 2002 among obese subjects1,6.
Recently, obesity has been related not only to general chronic diseases but also to localized diseases such as those in the oral cavity. Studies have reported that periodontitis is associated to obesity and chronic diseases. Periodontitis (presence of bacteria) increases the synthesis of inflammatory cytokines (TNF- α, IL-6) which are related to obesity (adipose tissue) and chronic diseases (diabetes, cardiovascular disease, etc.), and vice versa, hormones and cytokines derived from the adipose tissue (obesity) are associated to periodontitis and chronic diseases1,2,7. An extensive review of the literature revealed few reports related to this association and no information for Mexican populations, so the aim of this study was to determine whether overweight-obesity is associated to periodontal disease in subjects who visited the Periodontics Clinic at the Faculty of Dentistry of the Autonomous University of San Luis de Potosi (UASLP), Mexico.
MATERIALS AND METHODS
A cross-sectional study was conducted from August 2008 to December 2009 on subjects who visited the UASLP Periodontics Clinic. A total 88 subjects who complied with selection criteria took part in the study – 28 subjects without overweightobesity and 60 with overweight-obesity. Subjects were selected using non-probability consecutive sampling and met the following criteria: Inclusionsubjects with and without diagnosis of overweight or obesity, aged 12 to 73 years, with permanent teeth, of either sex, who accepted to participate in the study. Exclusion criteria: pregnancy, edentulous patients or patients with evident genetic alterations. The examiner was calibrated for all the study variables. A general clinical and dental history was obtained and the following parameters were evaluated blind: 1. Body Mass Index (BMI): weight in kilograms divided by height squared. The overweight- obese group included subjects with BMI ≥ 25 Kg/m2 or ≥ 30 Kg/m2 for obese subjects) 2. Waist circumference: measured with a millimetric tape measure1,2. Frequency of dental bacterial plaque, calculus, gingivitis index, probing depth and periodontal disease index (PDI) were reported. The following teeth were evaluated: first upper right molar, upper left central incisor, first upper left premolar, first lower left molar, lower right central incisor and first lower right premolar8.
Dental bacterial plaque: reported as absent (level 0, without plaque) or present (dental plaque interproximal and/or marginal and/or present on 1, 2 thirds or more of the vestibular and/or palatinal-lingual surfaces)9. Calculus index: evaluated as absent (without calculus) or present (supra and/or sugingival calculus)9. The Loe & Silness (1963) gingivitis index was obtained and reported as absent (without inflammation) or present (gingival inflammation)10. Probing depth: recorded as the distance from the gingival margin to the bottom of the pocket using a calibrated periodontal probe graduated in mm (Hu- Friedy), considering a healthy sulcus < 3mm11,12. Periodontal disease index (PDI)9 was reported, which is a combination of the PMA (papillary marginal epithelium attachment) index and the PI (periodontal index), and evaluated as absent (healthy tissues) or present13,14. Data were reported as mean ± standard deviation, range, frequencies and percentage. To establish differences between groups, we used the Chi Square (X2) test for qualitative variables and the U. Mann Whitney test for qualitative variables. A binary multivariate logistic regression analysis was performed to estimate the association between overweight-obesity determined by BMI and periodontal disease. For the analysis, the dichotomous dependent variable was established as: 1- with overweight- obesity and 0- without overweight-obesity. The independent variables were: sex, age and periodontal disease. The Hosmer-Lemeshow goodness of fit statistic was used to check the fit of the model. Analyses were performed with JMP V 4.0 and Stat View software with an alpha level set at p < 0.05.
RESULTS
The study included 88 subjects who visited the UASLP Periodontics Clinic (about 800 subjects per year visit the clinic, so the sample represents 11.0 % of the population per year). Table 1 shows study subjects’ anthropometric and oral measurements. Subjects were aged 12 to 73 years, of either sex (60% female) with an average body mass index of 26 ± 4 and waist circumference 87 ± 11. With regard to the variables evaluated in the mouth, 92% had bacterial plaque, 83% had calculus, 91% had gingivitis and 58% had periodontal disease, with an average probing depth of 3±0.4, ranging from 2 to 5 mm. Table 2 shows anthropometric and oral measurements, with the sample divided into two study groups – subjects with and without overweight-obesity. In the study there were 28 subjects without overweight-obesity aged 12 to 73 years, of both sexes (68% female) and 60 subjects (48 overweight and 12 obese) with overweight-obesity, of both sexes (57% female) aged 17 to 67 years.
Table 1: Anthropometric and oral measurements of all study subjects.
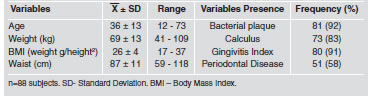
Table 2: Age, body mass index, waist index, bacterial plaque, calculus and probing depth in subjects with and without overweight-obesity.

On comparing the study groups we found statistically significant differences (p<0.05) in the variables weight, body mass index and waist circumference. In the group of subjects without overweight-obesity, 3.5% (n =1) had diabetes and high blood pressure, while in the group of subjects with overweight-obesity, 13.3% (n=8) had diabetes and 3.3% (n=2) had high blood pressure. Regarding the mouth variables, the highest frequencies and percentages are reported in the group of patients with overweight-obesity, with statistically significant differences in the variables calculus (p=0.0015), gingivitis index (p=0.0050) (Fig. 1) and periodontal disease (p=0.0154) (Fig. 2). In the multivariate analysis using subjects with and without overweight- obesity as a dependent variable, periodontal disease was associated to subjects with overweight-obesity (OR=3.16; CI 95% = 3.11–4.80, p=0.0162).

Fig. 1: Frequency of Gingivitis Index in groups of subjects with and without overweight-obesity. * Statistical test: Chi Square. Comparison of groups shows statistically significant differences p=0.0050.

Fig. 2: Frequency of periodontal disease in groups of subjects with and without overweight-obesity. Statistical test: Chi Square (X2). *Comparison of groups shows statistically significant differences p=0.0154
DISCUSSION
Obesity is the result of complex interaction among genetic, immunological, nutritional, psychological, environmental and socioeconomic factors, among others. Prevalence of overweight and obesity has increased in recent years, and they are considered as factors associated to other chronic diseases related to the reduction in quality of life and increase in mortality1,2,15. In addition to relating obesity to general chronic diseases, several authors have also performed studies to identify the association between overweight and/or obesity and alterations in the mouth (local diseases) such as periodontal disease12,16. In this study, subjects with overweightobesity were associated with the gingivitis index (p=0.0050) and periodontal disease (p=0.0154) (OR = 3.16; CI 95%=3.11–4.80, p=0.016).
These results match data published by other researchers12,17-21. It has been reported that obesity defined by BMI, waist circumference and high percentage of fat was significantly associated to the increase in periodontitis among adults in Jordan12. Some authors have classified the different obesity indicators (BMI and the waist and hip index) into degrees of affection (low, medium and high). They found that only subjects with high BMI and waist-hip index were associated to periodontitis17. Studies relating obesity to periodontitis in different age groups have also been reported. Ekuni et al., evaluated 618 young Japanese subjects aged 18 to 24 years with BMI IMC <30 kg/m2, and found that age and BMI were associated to the periodontal index. The logistic regression analysis revealed that the risk of Periodontitis increases by l6% per increase of 1 kg/m2 in BMI (OR = 1.16, 1.03-1.31 (CI 95%) p<0.05)18. Another study evaluated 513 mine laborers in India aged 18 to 54 years, reporting a 57% risk of periodontitis per increase of 1 kg/m2 in BMI19. Associations among variables have also been reported in older populations. In a study on 298 men aged 60 to 70 years, an association was found between obesity and periodontitis (OR=1.77, p=0,004) observed on at least two teeth without including the interproximal surfaces with loss of epithelial insertion level ≥ 5 mm20. These findings match those of studies reporting only an association between overweight and obesity and periodontitis in young subjects (18 to 34 years old), and did not find an association in subjects older than 34 years (35 to 90 years)21.
Some possible explanations of the relationship between overweight/obesity and inflammatory processes (periodontitis) are mentioned below. The adipose cells secreted by the adipose tissue, such as adipocytes, preadipocytes and macrophages secrete adipokines locally or in the systemic circulation of liver, muscle and endothelium. Adipokines act as hormonal- type proteins (e.g. leptin and adiponectin), as cytokines (e.g. tumor necrosis factor α (TNF- α), interleukin 6 (IL-6), as proteins that participate in vascular hemostasis (e.g. plasminogen activator inhibitor 1 (PAI-1), tissue factor), as blood pressure regulators (e.g. angiotensinogen), angiogenesis promoters (e.g. vascular endothelial growth factor VEGF) and as receptors in acute phases (e.g. C-reactive peptide)1,2,20. Possible mechanisms for the association between obesity and periodontal disease have been published. 1. Obese rats with high blood pressure have been found to be associated to periodontal disease due to a thickening of the intima of blood vessels, with a reduction in blood flow17. 2. A high cholesterol diet is associated with proliferation of the epithelium of the junction with increased bone resorption in rats with periodontitis22. 3. The adipose tissue secretes cytokines (TNF-α, IL-6) associated to inflammatory processes (periodontitis)1,2,17,23. 4. PAI-1 is significantly expressed in visceral fat, causing blood clotting and reducing blood flow17. 5. Leptin stimulates the immunological system, favoring cytokine production and phagocytosis, it has also been reported that it takes part in bone formation2,5,23. On the other hand, there are reports that do not identify any association among the variables of interest. On e of them included 706 subjects aged 30 to 65 years from southern Brazil, and the authors reported an association between obesity and periodontitis in females, but found no association between overweight and periodontitis in both sexes24. It has been reported that in a Scandinavian population of 878 women and 719 men, with a total 1597 subjects aged 20 to 95 years, no association was found between loss in the level of epithelial insertion and obesity measured by BMI25.
Papers published on research into overweight-obesity and its association with periodontitis are based on cross-sectional studies, like this one, therefore longitudinal or intervention studies should be conducted to evaluate more objective measures of obesity (adiposity) and including representative sample sizes of general populations with the aim of providing greater understanding of the relationship between periodontal disease and obesity in different populations1.
ACKNOWLEDGMENTS
This study was supported by Faculty of Dentistry. Autonomous University San Luis Potosi (UASLP).
1. Ritchie CS. Obesity and periodontal disease. Periodontol 2000 2007;44:154-163. [ Links ]
2. Pischon N, Heng N, Bernimoulin JP, Kleber BM, Willich SN, Pischon T. Obesity, inflammation, and periodontal disease. J Dent Res 2007;86:400-409. [ Links ]
3. Low S, Chin MC, Deurenberg-Yap M. Review on epidemic of obesity. Ann Acad Med Singapore 2009;38:57-59. [ Links ]
4. Barquera S, Campos-Nonato I, Hernandez-Barrera L, Flores M, Durazo-Arvizu R, Kanter R, Rivera JA. Obesity and central adiposity in Mexican adults: results from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51:S595-603. [ Links ]
5. Saito T, Shimazaki Y. Metabolic disorders related to obesity and periodontal disease Periodontol 2000 2008;18: 162-170. [ Links ]
6. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight and obesity. JAMA 2005;293:1861-1867. [ Links ]
7. Ylostalo P, Suominen-Taipale L, Reunanen A, Knuuttila M. Association between body weight and periodontal infection. J Clin Periodontol 2008;35:297-304. [ Links ]
8. Ramfjord SP. Indices for prevalence and incidente of periodontal disease. J Periodontol 1959;30:51-61. [ Links ]
9. Ramfjord SP. The periodontal disease index (PDI). J Periodontol 1967;38:602-610. [ Links ]
10. Loe H & Silness J. Periodontal disease in pregnancy. Acta Odontol Scand 1963;21:533-551. [ Links ]
11. Patino-Marin N, Martinez F, Loyola-Rodriguez JP, Tenorio- Govea E, Brito-Orta MD, Rodriguez-Martinez M. A novel procedure for evaluating gingival perfusion status using laser-doppler flowmetry. J Clin Periodontol 2005; 32:231-237. [ Links ]
12. Khader YS, Bawadi HA, Haroun TF, Alomari M, Tayyem RF. The association between periodontal disease and obesity among adults in Jordan. J Clin Periodontol 2009;36:18-24. [ Links ]
13. Russell AL. A system of classification and scoring for prevalence surveys of periodontal disease. J Dent Res 1956;35:350. [ Links ]
14. Schour I, Massler M. Survey of gingival disease using the PMA index. J Dent Res 1948;27:733-739. [ Links ]
15. Patino Marin N, Loyola Rodriguez JP, Medina Solis CE, Pontigo Loyola AP, Reyes Macias JF, Ortega Rosado JC, Aradillas Garcia C. Caries, periodontal disease and tooth loss in patients with diabetes mellitus types 1 and 2. Acta Odontol Latinoam. 2008;21:127-133. [ Links ]
16. Wood N, Johnson RB, Streckfus CF. Comparison of body composition and periodontal disease using nutritional assessment techniques: Third National Health and Nutrition Examination Survey (NHANES III). J Clin Periodontol 2003;30:321-327. [ Links ]
17. Saito T, Shimazaki Y, Koga T, Tsuzuki M, Ohshima A. Relationship between upper body obesity and periodontitis. J Dent Res 2001;80:1631-1636. [ Links ]
18. Ekuni D, Yamamoto T, Koyama R, Tsuneishi M, Naito K, Tobe K. Relationship between body mass index and periodontitis in young Japanese adults. J Periodontal Res 2008; 43:417-421. [ Links ]
19. Kumar S, Dagli RJ, Dhanni C, Duraiswamy P. Relationship of body mass index with periodontal health status of green marble mine laborers in Kesariyaji, India. Braz Oral Res 2009;23:365-369. [ Links ]
20. Linden G, Patterson C, Evans A, Kee F. Obesity and periodontitis in 60-70-year-old men. J Clin Periodontol 2007;34:461-466. [ Links ]
21. Al-Zahrani MS, Bissada NF, Borawskit EA. Obesity and periodontal disease in young, middle-aged, and older adults. J Periodontol 2003;74:610-615. [ Links ]
22. Saxlin T, Suominen-Taipale L, Leiviska J, Jula A, Knuuttila M, Ylostalo P. Role of serum cytokines tumour necrosis factoralpha and interleukin-6 in the association between body weight and periodontal infection. J Clin Periodontol 2009;36:100-105. [ Links ]
23. Tomofuji T, Kusano H, Azuma T, Ekuni D, Yamamoto T, Watanabe T. Effects of a high-cholesterol diet on cell behavior in rat periodontitis. J Dent Res 2005;84:752–756.
24. Dalla Vecchia CF, Susin C, Rosing CK, Oppermann RV, Albandar JM. J Periodontol. Overweight and obesity as risk indicators for periodontitis in adults. J Periodontol 2005;76:1721-1728. [ Links ]
25. Kongstad J, Hvidtfeldt UA, Gronbaek M, Stoltze K, Holmstrup P. The relationship between body mass index and periodontitis in the Copenhagen City Heart Study. J Periodontol 2009;80:1246-1253. [ Links ]

