










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.24 no.1 Buenos Aires abr. 2011
ARTÍCULOS ORIGINALES
Relationship among metabolic control, oral parameters and self-efficacy in diabetic patients
Carlos Serrano1, Graciela Pardo2, Luz A. Barrera3, Luisa Gamboa3, Angela Másmela3, Sandra Zorro3
1Department of Basic Science and Oral Medicine, School of Dentistry.
2Department of Psychology, School of Human Science, Universidad Nacional de Colombia.
3Former students, School of Dentistry, Universidad Nacional de Colombia.
CORRESPONDENCE Dr. Carlos Serrano Carrera 30 # 45-03, Building 210 Bogota, Colombia caserranom@unal.edu.co
ABSTRACT
The aim of the present study was to evaluate the relationship between patients’ answers to behavioral questionnaires on diabetes and oral health, oral parameters and metabolic control of diabetes. A cross-sectional study was conducted on fifty type 2 diabetic subjects selected according to specific criteria, mainly: diagnosis of type 2 diabetes mellitus occurred at least 6 months before the study, presence of ≥5 natural teeth and having at least two recent glycated hemoglobin (HbA1c) measurements. Three questionnaires were administered to the patients after a preliminary testing phase. The questionnaires were: Multidimensional Diabetes Questionnaire (MDQ), organized in three sections; Stress Evaluation Questionnaire for Diabetics, a single questionnaire; and Dental Self-efficacy, organized in three sections. Clinical parameters were O’Leary Plaque Index, and percentage of bleeding on probing. Diabetic metabolic control was calculated using HbA1c measurements. Reliability of questionnaires was analyzed using Cronbach’s α coefficient. Relationship among variables was tested by Pearson Correlation analysis. A p-value <0.05 was significant. Results: The mean age of the study sample was 52.2 years; 38 individuals were women (77%), and 12 were men (23%). The majority had only completed elementary education (55%). Mean plaque index score was 53.51% (SD 21.6), mean bleeding on probing was 36.33% (SD 23.65). Mean HbA1c value was 9.22% (SD 2.6). Dental self-efficacy for using dental floss and visiting a dentist was low, but it was high for tooth brushing. There was a significant correlation between the MDQ and HbA1c. Percentage of bleeding on probing had a correlation with self-efficacy for dental visits. The MDQ section I had a correlation with O’Leary Plaque Index, sections II and III had a correlation with self-efficacy for tooth brushing, section III had a correlation with self-efficacy for visiting a dentist. In conclusion, self-efficacy questionnaires for tooth brushing and visiting a dentist had a significant correlation with selfefficacy for diabetes control.
Key words: Behavior; Self-efficacy; Behavioral research; Diabetes mellitus; Oral hygiene.
RESUMEN
Relaciones entre control metabólico, parámetros clínicos y el modelo comportamental de auto-eficacia en pacientes diabéticos tipo 2
El objetivo del presente trabajo fue estudiar la relacion entre las respuestas a cuestionarios que evaluan teorias de comportamiento para diabetes y salud oral, parametros clinicos orales y el control metabolico de la diabetes mellitus tipo 2. Se realizo un estudio de tipo seccional en una muestra de cincuenta pacientes diabeticos tipo 2 seleccionados de acuerdo a criterios especificos, entre ellos: Diagnostico de diabetes mellitus tipo 2 ocurrido por lo menos 6 meses antes del inicio del estudio, presencia de por lo menos 5 dientes naturales y poseer dos examenes de porcentaje de hemoglobina glucolizada obtenidos durante el ultimo ano. Despues de un proceso de traduccion, adaptacion y prueba preliminar, los pacientes respondieron tres cuestionarios psicologicos que evaluan patrones de comportamiento especificos, los cuestionarios fueron: Cuestionario de Auto-eficacia Oral, organizado en tres secciones distintas; Cuestionario de Evaluacion de Estres en Diabeticos, compuesto por una sola seccion; y Cuestionario Multi-dimensional en Diabetes; organizado en tres secciones. En particular la seccion III del Cuestionario Multi-dimensional en Diabetes mide parametros asociados con auto-eficacia relacionados con la condicion diabetica. Los parametros clinicos medidos fueron el Indice de Placa segun O´Leary, y el porcentaje de hemorragia al sondaje. El control metabolico de la diabetes fue determinado a traves del porcentaje de hemoglobina glucolizada (HbA1c) La confiabilidad de los cuestionarios fue establecida por la prueba del Coeficiente-α de Cronbach. La relacion entre las variables se estudio a traves del Analisis de Correlacion de Pearson. Valor p<0.05. Resultados: La edad promedio de la muestra del estudio fue de 52.2 anos, del total de 50 pacientes 38 individuos (77%) eran mujeres y 12 individuos (23%) eran hombres; la mayoria de los sujetos poseian solo educacion primaria (55%). El promedio del nivel de placa bacteriana era de 53.51% (DE 21.6), el promedio de porcentaje de hemorragia al sondaje era de 36.33% (DE 23.65). El promedio de los niveles de hemoglobina glucolizada era de 9.22% (DE 2.6), lo cual revela un mal control metabolico de la enfermedad. Los niveles de auto-eficacia oral para la utilizacion de seda dental y visita al odontologo fueron bajos, pero la auto-eficacia oral para el cepillado dental fue alta. Se encontro una relacion significativa entre los resultados del Cuestionario Multi-dimensional en Diabetes y los niveles de HbA1c. El porcentaje de hemorragia al sondaje se correlaciono con la auto-eficacia oral para visitar de forma regular al odontologo. El Cuestionario Multidimensional en Diabetes, seccion I se correlaciono con los valores de Indice de Placa de O´Leary; las secciones II y III se correlacionaron con la auto-eficacia para el cepillado dental, la seccion III tuvo una relacion significativa con la auto-eficacia para visitar al odontologo. Conclusion: Los resultados de los cuestionarios de auto-eficacia oral para el cepillado dental y la visita regular al odontologo tuvieron una correlacion significativa con la seccion del Cuestionario Multi-dimensional en Diabetes que mide auto-eficacia para el control de la diabetes.
Palabras clave: Modelo de Auto-eficacia; Investigacion Comportamental; Diabetes Mellitus; Higiene Oral.
INTRODUCTION
The prevalence of diabetes mellitus is increasing worldwide, affecting more than 170 million individuals around the world. In developed societies, diabetes mellitus has reached about 6% of the population, but developing countries could account for the greatest future increase in the prevalence of the disease1, 2. Approximately 90% of diabetic subjects can be classified as having type 2 diabetes, a disease characterized by insulin resistance and abnormal insulin secretion. Diabetic subjects present an increased prevalence of periodontal disease. A cross-sectional analysis of 4343 individuals included in the National Health and Nutrition Examination Study III (NHANES III) of U.S.A. calculated a 1.56 adjusted odds ratio for having severe periodontitis in diabetic subjects, this odds ratio increased to 2.90 when subjects with poorly controlled diabetes were separately analyzed3. A meta-analysis involving 3500 individuals demonstrated a significant association between diabetes and periodontitis4. An epidemiological study on the Pima Indian community, described as having the world’s highest incidence of type 2 diabetes mellitus, reported higher prevalence of periodontal disease in diabetics at different age ranges. Differences were greater at younger ages (15-34 years) than at older ages (≥55), where periodontal disease affected the majority of the population independently of diabetic status. Incidence of periodontal disease was approximately three times higher in diabetic subjects at a 2.6-year follow-up5.
Adherence to medical treatment, defined as the extent to which a person’s behavior coincides with medical advice, including medication-taking and lifestyle practices, is an important aspect of treatment for diabetes and periodontal disease. Diabetic subjects are asked to take medication, follow a meal plan, exercise, monitor blood glucose levels and make adjustments to their regimen when warranted 6. Meanwhile, periodontal patients are asked to perform daily removal of bacterial plaque by tooth brushing and interdental cleaning; it has been established that performance of professional mechanical therapy without proper plaque control does not contribute to improved periodontal status7, 8. Several psychological models have been formulated to explain health behavior of patients; they consider a person’s knowledge, beliefs, attitudes, feelings, values, psychomotor skills and previous behaviors9. Behavioral models applied to oral hygiene practices were summarized in five approaches by Inglehart and Tedesco10: self-efficacy theory, health belief model, theory of reasoned action, theory of planned action and relapse prevention model. A Cochrane collaboration systematic review concluded that there is tentative evidence that different psychological approaches can improve oral hygiene behavior of subjects, measured as self-informed tooth brushing and dental floss practices, and plaque and gingival bleeding scores11.
A research group from Oulu University (Oulu, Finland) has performed an analysis of several psychological model questionnaires related to oral health behavior and metabolic control of diabetes; the models studied included: dental self-efficacy, attributions, self-esteem and the theory of reasoned action12-15. The authors suggested that oral health behavior and diabetes self-care have psychological factors in common. In particular, the report of Syrjala et al.12 focused on the self-efficacy model described by Bandura16; according to this model, individuals perform activities with which they feel they can cope and avoid activities they feel they can not manage; thus self-efficacy determines initiation and persistence with an activity. A dental self-efficacy questionnaire was developed containing seventeen questions, it was tested in a group of 31 non-diabetic patients and 21 diabetic patients before being applied12 . The aim of this project was to study the relationship among two behavioral model questionnaires for diabetes and one for oral health, oral clinical parameters and diabetic metabolic control. Behavioral models measure psychological aspects that could influence the performance of daily self-care activities for controlling both diseases.
MATERIALS AND METHODS
Study Design and Patient Population
A cross-sectional study was performed on a sample of fifty type 2 diabetic subjects being treated at the outpatient clinic of the Colombian Diabetic Association (Bogota, Colombia). Subjects that fulfilled the following inclusion criteria were invited to participate in the study, which included an oral examination, three different survey questionnaires and the collection of metabolic control data. Inclusion criteria:
• Type 2 diabetes mellitus diagnosis occurred at least six months before the study.
• Presence of at least 5 natural teeth.
• Had at least two measurements of glycated hemoglobin levels obtained during the past year (HbA1c), considering HbA1c examinations are taken at three-month intervals at this diabetes treatment clinic.
Exclusion criteria
• Type 2 diabetes mellitus related to pregnancy, alcoholism or pancreatitis.
The study was approved by the ethical committee of the Dental School, Universidad Nacional de Colombia, and the Colombian Diabetic Association. All subjects signed an informed consent statement prior to inclusion in the study.
Data Collection
Demographic data collected from subjects included: age, gender, marital status and educational level. Educational level was categorized as: elementary education, secondary education, technical qualification and university education. The O’Leary Plaque Index17 and percentage of bleeding on periodontal probing were measured in all present teeth at six surfaces per tooth: mesiobuccal, midbuccal, distobuccal, mesiolingual, midlingual and distolingual. The O’Leary Plaque Index was chosen as it includes using a disclosing solution for detecting presence/absence of plaque, facilitating the examination procedure. Percentage of bleeding on periodontal probing was determined as gingival bleeding in a period of 10 second after probing. Diabetic metabolic control was assessed by an average of at least two glycated hemoglobin levels obtained during the previous year under diabetic treatment.
Questionnaires
Three different questionnaires were administered to all patients; assistance was provided to answer any possible doubt regarding questions. A first questionnaire was related to oral health self-efficacy; the other two questionnaires were related to diabetes; one was about cognitive and social factors, and the other was about stress associated with diabetic status. Original English versions of all questionnaires were translated into Spanish by two licensed translators from the Foreign Language Department, School of Social Science, Universidad Nacional de Colombia. Translated versions were refined by two expert associate professors from the Department of Psychology and the Dental School. Questionnaires were evaluated in an independent group of 10 type 2 diabetic subjects; further modifications were performed based on feedback from questionnaire application on patients.
The first questionnaire evaluated was the Dental Self-efficacy Questionnaire (DSelf-efficacyQ) designed by Syrjala et al.12 which consisted of seventeen questions: five regarding self-efficacy for tooth brushing; five for self-efficacy for approximal cleaning and seven regarding self-efficacy for visiting a dentist. Table 1 provides an example of item questions. Two questions described in the original report related to work interference were eliminated, because of their close similarity to other questions (Table 2). Four possible answer scores were given to questions: completely confident (4 points), fairly confident (3 points), fairly confident not to (2 points) and completely confident not to (1 point).
Table 1: Example of item questions.

Table 2

The second questionnaire was the Multidimensional Diabetic Questionnaire (MDQ) designed by Talbot et al.18 This questionnaire aims at a comprehensive diabetes behavior evaluation; hence it is described as multidimensional. The original MDQ consists of 41 questions organized in three sections; the first section studies general perception of diabetes and related social support and comprises 16 items; the second section focuses on social incentives in relation to self-care activities and comprises 12 items; the third section was designed to assess self-efficacy expectations as well as outcome expectations and comprises 13 items; examples of questions are provided in Table 1. The patient’s answers to the MQD questionnaire sections I and II were scored on a 7-point rating-scale (0 to 6); for the first section, higher scores mean an increased level of perceived interference; for the second section an increased score indicates greater levels of positive and misguided reinforcement behavior. MQD questionnaire section III answers were evaluated on a 0 to 100 point rating scale, meaning 0 feeling “not confident” and 100 feeling “very confident” about performing activities related to diabetic control; thus assessing self-efficacy for diabetic control, or feeling more confident of a positive outcome when performing daily activities for diabetic control. Two questions were eliminated from the questionnaire after expert revision because they were considered redundant (Table 2). The third questionnaire was the Diabetic Stress Questionnaire (DStressQ), designed by Hershbach et al.19. It assesses situations that are sources of stress for diabetic patients using 45 questions. Patients are asked to measure the level of stress that specific situations could cause them on a 5-point rating scale, ranging from “a slight problem” to “a very big problem” (Table 1).
Statistical Analysis
The three questionnaires were evaluated for internal consistency using the Cronbach’s α reliability coefficients. Means and standard deviations were calculated for data description. Correlation among the three types of variables was tested by the Pearson Correlation analysis. A p-value < .05 was considered to indicate significance. SPSS for Windows was used for statistical analysis.
RESULTS
Sample Description
The study population included fifty type 2 diabetic patients with a mean age of 52.2 years, ranging from 25 to 65 years; they were predominantly women, with 38 women and 12 men. Twenty-seven patients had only completed elementary education, 10 had high school education and 13 had technical or university education. More than half of the patients (30) were married; other patients were single, among whom 14 were widowed.
Clinical Parameters
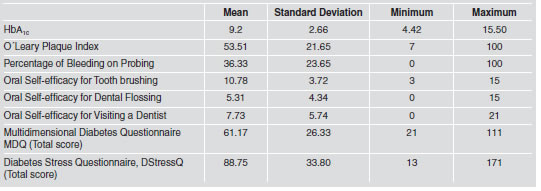
Mean glycated hemoglobin level was 9.22% (SD 2.66), showing a poor metabolic control of diabetes. The O’Leary Plaque Index and percentage of bleeding on probing were equally high with mean values of 53.51% (SD 21.65) and 36.33% (23.65), respectively (Table 3).
Table 3: Description of Clinical Parameters and Questionnaire Results (n=50)
Questionnaires
Evaluation of the three questionnaires revealed high Cronbach α reliability coefficients, with values ranging from 0.81 up to 0.97 (Table 4). These high values indicate good intercorrelation among questionnaire items measuring a single defined construct.
Table 4: Cronbach α Reliability Coefficient of questionnaires

Questionnaire Results
Levels of oral self-efficacy were low, with a mean score of 9.22 (SD 2.66). Results for the other two questionnaires, the MDQ and the DStressQ, showed moderate levels of interference for adherence to diabetic treatment and stress related to daily situations faced by a diabetic patient. The mean MDQ score was 61.17 (SD 26.33); the mean value for the DStressQ was 88.75 (SD 33.80) (Table 3).
Correlation among
Variables Individuals reporting high self-efficacy for tooth brushing also reported high self-efficacy for dental flossing and self-efficacy for visiting a dentist, 0.37 (p<0.01) and 0.30 (p<0.05), respectively. Similar to the previous result, self-efficacy for dental flossing was correlated with self-efficacy for visiting a dentist, with a correlation coefficient 0.52 (p<0.01). Those individuals reporting high self-efficacy for visiting a dentist showed a lower percentage of bleeding on probing with a correlation coefficient of -0.26 (p<0.05); for tooth brushing and dental flossing questionnaire results, there was no correlation with percentage of bleeding on probing. The O’Leary Plaque Index did not significantly correlate with any section of the oral self-efficacy questionnaire. The total score for the MDQ correlated with HbA1c levels, with a coefficient of 0.29 (p<0.05); on the contrary, the DStressQ did not correlate with HbA1c.. The two diabetic questionnaires did not correlate with each other. Oral and diabetic variables showed four different correlations. Self-efficacy for tooth brushing had a correlation with the MDQ, sections II and III, with correlation coefficients of 0.33 and 0.27 (p<0.05) respectively; in particular section III measures selfefficacy for diabetic control. Similarly self-efficacy for visiting a dentist had a correlation with MDQ section III, with a correlation factor of 0.30 (p<0.05). The O’Leary Plaque Index examination was inversely correlated with the MDQ, section I, correlation factor -0.28 (p<0.05), this meaning lower plaque scores in subjects reporting a higher frequency of positive reinforcement or interference of diabetes with daily activities (Table 5, Table 6).
DISCUSSION
The onset of gingival inflammation is related to inadequate supragingival plaque control; as a result, establishment of optimal self-performed plaque control is an important goal of periodontal therapy7. Motivation, knowledge, provision of oral hygiene instructions, type of oral hygiene aids and manual dexterity determine the effectiveness of mechanical plaque control by self-care20. Regarding diabetic treatment, individuals are expected to be engaged in a series of self-care activities; adherence to treatment defined as the extent to which a person’s behavior coincides with medical advice recognizes personal motivation and knowledge as important factors for performance of self-care activities 5. Similar behavior that leads to plaque control could lead to adequate diabetic control; this was the reason for analysis of correlations between oral health and diabetic parameters in a small sample of subjects. The present study was designed as a baseline assessment in order to identify significant parameters that could be included in a health promotion program for diabetic patients. Considering an examination time of approximately one hour per patient, which included a full-mouth oral examination and assisted administration of 104 questions, in addition to limited financial funding, a total of 50 patients could be included in the study. In spite of the sample size, significant correlations were found between self-efficacy for oral health and self-efficacy for diabetic control.
Statistical analysis among clinical parameters showed no correlation between HbA1c levels, the O’Leary Plaque Index and Percentage of Bleeding on Probing; all three parameters were elevated in the population studied. Several references have shown increased gingival inflammation in diabetics, in some cases related to poorer metabolic control, compared with control groups 21-24. Considering that no control group was included, and that the majority of individuals demonstrated equally poor oral conditions and diabetic metabolic control, finding significant correlations could be difficult. Analysis of the relationship between psychological questionnaires and clinical parameters showed there was a correlation between the MDQ and HbA1c levels; however, there was no correlation between the DStressQ and HbA1c. With regard to the lack of correlation for the sample studied, one must consider difficulties in adapting questionnaires originally developed in samples of diabetic subjects in Finland, Canada and Germany; countries with possible differences in attitudes, beliefs and behavior compared to Colombia. This adaptation process would require further instrument refining and testing, present results could serve as an initial step for future application of questionnaires. The study by Syrjala et al.12 using the DSelf-efficacyQ on 149 insulin-dependent subjects reported an inverse correlation between visible plaque index scores and tooth brushing self-efficacy, and the visible plaque index and dental visiting self-efficacy; but not correlation with approximal cleaning self-efficacy. In contrast, our results did not show a correlation between the O’Leary Plaque Index and any of the three components of the DSelf-efficacyQ; a significant inverse correlation was found for percentage of bleeding on probing and self-efficacy for dental visiting. Another finding of Syrjala et al.12 was that HbA1c was lower in subjects reporting higher self-efficacy for tooth brushing, more frequent tooth brushing reporting and lower visible plaque index; in contrast to the present findings. An interesting finding of the present study was a correlation between self-efficacy for tooth brushing and self-efficacy for diabetic control (MDQ, section III), and between self-efficacy for visiting a dentist and selfefficacy for diabetes control (MDQ, section III); thus showing how self-efficacy behavioral models applied to different diseases could lead to similar scores.
The different results of the present study compared to the study of Syrjala et al.12 report could be a consequence of very different sample characteristics. In the study by Syrjala et al.12, the subjects were predominantly type 1 diabetics, in contrast to the subjects of the present sample, who were type 2 diabetics. Moreover, the mean ages for the two study samples were markedly different: 34 years compared to 52 years in our study. Probably related to differences in mean age, subjects in the Finish study had an average of 25 teeth, in contrast to high values of lost teeth in the current study. Education level was different comparing the two samples: in the study by Syrjala et al.12, most subjects had undergone some form of professional or non-professional education; while in our sample, most subjects had only elementary education. A similarity between both samples was a poor metabolic control of diabetes, for Syrjala et al.12 mean HbA1c level was 8.5%, for the Colombian Diabetic Association sample mean HbA1c was 9.2%.
The patients who visit the Colombian Diabetic Association can be characterized as belonging to low- to middle-income class, and having a low education level. Many of them visit the Association because they lack coverage from health insurances companies at which regularly employed individuals and their families are registered. Large U.S. epidemiological studies have found that socio-economic status (SES) variables were associated with diabetes25, 26 and periodontitis27, 28. A similar relationship among lower SES, poor diabetic control and worse periodontal condition has been found in developing countries such as Pakistan29. Regarding the relationship between the different variables measured in the present sample, the socio-economic status of patients should be considered. Originating from a lower SES, patients in the current study could be prone to more severe periodontal disease and poorer metabolic control than other diabetic subjects with higher SES. Having patients with a wider range of periodontal status and metabolic control, the correlation with behavioral questionnaires answers might differ.
CONCLUSION
The oral health and diabetic behavior questionnaires studied and the clinical parameters showed several correlations; in particular significant correlations were found between self-efficacy for: tooth brushing, visiting a dentist and diabetic control
1. Zimmet P, Alberti KG, Shaw J. Global and Societal Implications of the Diabetes Epidemic. Nature 2001;414:782-787. [ Links ]
2. King H, Ausbert KG, Herman WH. Global burden of diabetes, 1995-2025: Prevalence, Numerical Estimates and Projections. Diabetes Care 1998;21:1414-1431. [ Links ]
3. Tsai C, Hayes C, Taylor GW. Glycemic Control of Type 2 Diabetes and Severe Periodontal Disease in the US Adult Population. Community Dent Oral Epidemiol 2002;30:182-192. [ Links ]
4. Mealy BL, Moritz AJ. Hormonal Influences: Effects of Diabetes Mellitus and Endogenous Female Sex Steroid Hormones on the Periodontium. Periodontol 2000 2003;32:59-81. [ Links ]
5. Nelson RG, Shlossman M, Budding LM, Pettitt DJ, Saad MF, Genco RJ, Knowler WC. Periodontal Disease and NIDDM in Pima Indians. Diabetes Care 1990;13:836-840. [ Links ]
6. Mac Nabb WL. Adherence in Diabetes: Can We Define It? and Can We Measure It?. Diabetes Care 1997;20:215-218. [ Links ]
7. Westfelt E. Rationale of Mechanical Plaque Control. J Clin Periodontol 1996;23:263-267. [ Links ]
8. Magnusson I, Lindhe J, Yoneyama T, Liljenberg B. Recolonization of a Subgingival Microbiota Following Scaling in Deep Pockets. J Clin. Periodontol 1984;11:193-207. [ Links ]
9. Schou L. Behavioral Aspects of Dental Plaque Control Measures: An Oral Health Promotion Perspective. In: Lang, NP., Attstrom, R., Loe, H. editors. Proceedings of the European Workshop on Mechanical Plaque Control. Berlin. Quintessence Books, 1998;287-299. [ Links ]
10. Inglehart M, Tedesco LA. Behavioral Research Related to Oral Hygiene Practices: A New Century Model of Oral Health Promotion. Periodontol 2000;1995;8:15-23. [ Links ]
11. Renz A, Ide M, Newton T, Robinson PG, Smith D. Psychological Interventions to Improve Adherence to Oral Hygiene in Adults with Periodontal Diseases. Cochrane Database Syst Rev 2007;18:CD005097. [ Links ]
12. Syrjala AMH, Kneckt MC, Knuuttila ML. Dental Self-efficacy as a Determinant to Oral Health Behavior, Oral Hygiene and HbA1c Level Among Diabetic Patients. J Clin Periodontol 1999; 26:616-621. [ Links ]
13. Kneckt MC, Syrjala AMH, Knuuttila ML. Attributions to dental and diabetes health outcomes. J Clin Periodontol 2000; 27:205-211. [ Links ]
14. Kneckt MC, Keinanen-Kiukaanniemi SM, Knuuttila ML, Syrjala AMH. Self-esteem as a Characteristic of Adherence to Daibetes and Dental Self-care Regimens. J Clin Periodontol 2001;28:175-180. [ Links ]
15. Syrjala AMH, Niskanen MC, Knuuttila ML. The Theory of Reasoned Action in Describing Tooth-brushing, Dental Caries and Diabetic Adherence Among Diabetic Patients. J Clin Periodontol 2002;29:427-432. [ Links ]
16. Bandura, A. Self-efficacy: Toward a Unifying Theory of Behavioral Change. Psychol Rev 1977;84:191-215. [ Links ]
17. O’Leary TJ, Drake RB, Naylor JE. The Plaque Control Record. J Periodontol 1972;43:38.
18. Talbot F, Nouwen A, Gingras J, Gosselin M, Audet J. The Assessment of Diabetes-Related Cognitive and Social Factors: The Multidimensional Diabetes Questionnaire. J Behav Med 1997;20:291-312. [ Links ]
19. Herschbach P, Duran G, Waadt S, Zettler A, Amm C, Marten-Mittag B. Psychometric Properties of the Questionnaire on Stress in Patients with Diabetes (QSD-R). Health Psychol 1997;16:171-174. [ Links ]
20. Axelsson P, Albandar JM, Rams TE, Prevention and Control of Periodontal Diseases in Developing and Industrialized Nations. Periodontol. 2000, 2002;29:235-246. [ Links ]
21. Gusberti F, Syed S, Bacon G, Grossman N, Loesche W. Puberty gingivitis in insulin-dependent diabetic children. I. Cross-sectional observations. J Periodontol 1983;54:714-720, [ Links ]
22. de Pommereau V, Dargent-Pare C, Robert JJ, Brion M. Periodontal Status in Insulin-Dependent Diabetic Adolescents. J Clin Periodontol 1992; 19: 628-632. [ Links ]
23. Karjalainen KM, Knuuttila ML. The Onset of Diabetes and Poor Metabolic Control Increases Gingival Bleeding in Children and Adolescents with Insulin-Dependent Diabetes Mellitus. J Clin Periodontol 1996;23:1060-1067. [ Links ]
24. Cutler CW, Machen RL, Jotwani R, Iacopino AM. Heightened Gingival Inflammation and Attachment Loss in Type 2 Diabetics with Hyperlipidemia. J Periodontol 1999;70: 1313-1321. [ Links ]
25. Brown AF. Patient, System and Clinician Level Interventions to Address Disparities in Diabetes Care. Curr Diabetes Rev 2007;3:244-248. [ Links ]
26. Robbins JM, Vaccarino V, Zhang H, Kasl SW. Socioeconomic Status and Type 2 Diabetes in African American and Non-Hispanic White Women and Men: Evidence from the Third National Health and Nutrition Examination Survey. Am J Public Health 2001;91:76-83. [ Links ]
27. Borrell LN, Burt BA, Warren RC, Neighbors HW. The Role of Individual and Nieghborhood Social Factors on Periodontitis: The Third National Health and Nutrition Examination Survey. J Periodontol 2006;77:444-453. [ Links ]
28. Borrel LN, Crawford ND. Social Disparities in Periodontitis Among United States Adults 1999-2004. Community Dent Oral Epidemiol 2008;36:383-391. [ Links ]
29. Javed F, Nasstrom K, Bechimol D, Altamash M, Klinge B, Engstrom PE. Comparison of Periodontal and Socioeconomic Status Between Subjects with Type 2 Diabetes Mellitus and Non-diabetic Control. J Periodontol 2007;78: 2112-2119. [ Links ]

