










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.24 no.1 Buenos Aires Apr. 2011
ARTÍCULOS ORIGINALES
Microleakage of a self-adhesive resin cement after post cementation
Veridiana Camilotti, Admilton Fritsche Consalter, Max Dobrovolsk, Virginia Bosquirolli, Priscila R.D. Busato, Marcio J. Mendonça
Operative Dentistry and Prosthodontics Area, Dental School, Western Paraná State University, Brazil
CORRESPONDENCE Professor Ms. Veridiana Camilotti Unioeste - Colegiado de Odontologia R. Universitaria, 2069 – Jd Universitario Cascavel-PR- 85.819-110 Brazil e-mail: vericamilotti@hotmail.com
ABSTRACT
The aim of this study is to evaluate the microleakage a self-adhesive cement recently marketed Rely X U100 (3M ESPE). Thirty roots of bovine teeth with 14 mm long were restored with selfadhesive cement and Glassix fiber post DC3 (FGM). Roots were randomly divided into three groups (n=10) according to the technique of placement of the cementing agent: G1 – Centrix syringe; G2 – Lentulo drill and G3 – Manual technical. After cementation, provisional restorations were fabricated with composite resin (Opallis/FGM) without the use adhesive system. After they were finished, polished and thermo cycled by 1000 cycles, in water at temperature of 5oC and 55oC, 30 seconds in each bath. For microleakage test each group of roots was immersed in recipients with Rodhamine B dye solution buffered at 2%, during 24 hours. After this time, the samples were washed in tap water, sectioned and evaluation of dye leakage. The values of infiltration were obtained by the qualitative method (scoring) and statistical analysis using Kruskal-Wallis test and also by the quantitative method (Image Tool) and statistical analysis using ANOVA one way. For both tests, no significant difference between the techniques of placement of the self-adhesive cement. Based on these findings, micro-infiltration was present in all groups, and the placement technique did not influence the degree of micro-leakage, both for the qualitative analysis as to the quantitative.
Key words: Dental cements; Tooth root; Dental leakage.
RESUMO
Micro-infiltração marginal de um cimento resinoso auto-adesivo
O objetivo deste estudo foi avaliar a capacidade de selamento marginal do cimento resinoso auto-adesivo Rely X U100 / 3M ESPE, recentemente introduzido no mercado. Trinta raizes de dentes bovinos com 14 mm de comprimento foram restauradas com cimento resinoso auto-adesivo e pinos pre-fabricados de fibra de vidro DC3 (Fiber post/ FGM). As raizes foram aleatoriamente divididas em tres grupos (n=10) de acordo com a tecnica de insercao do agente de cimentacao: G1 - Broca lentulo; G2 - Seringa Centrix e G3 - Tecnica Manual. Apos a cimentacao, foram confeccionadas restauracoes provisorias com resina composta (Opallis DA2/FGM) sem utilizacao de sistema adesivo. As raizes foram impermeabilizadas com esmalte de unha azul, deixando exposta a linha de uniao resina/dente. Em seguida, foram submetidas a ciclagem termica com 1000 ciclos entre 50 e 550C. Para o teste de micro-infiltracao, as raizes foram armazenadas em solucao de corante Rodhamina B por 24 horas. Apos este periodo, as raizes foram limpas e seccionadas no sentido longitudinal para avaliacao da infiltracao do corante. Os valores da infiltracao foram obtidos pelo metodo qualitativo (escores) e a analise estatistica foi realizada atraves do teste Kruskal-Wallis e tambem pelo metodo quantitativo (Image ToolR) e a analise estatistica realizada pelo teste ANOVA (one-way). Para ambas as analises, nao houve diferenca significativa entre as tecnicas de insercao do cimento resinoso auto-adesivo. Com base nos achados, a micro-infiltracao esteve presente em todos os grupos avaliados, e a tecnica de insercao nao influenciou o grau de micro-infiltracao marginal, tanto para a analise qualitativa como para a quantitativa.
Palavras-chaves: Cimento resinoso; Raiz dental; Micro-infiltracao.
INTRODUCTION
At present, aesthetic restorations of endodontically treated teeth has been a great challenge in odontological clinical practices. Great coronary destructions frequently require the use of intraradicular dowels for better fixation of restoring material, as well as for a better dissipation of forces during mastication1. Cementation procedures represent an important step for the use of intraradicular dowels in clinical practice. Different resinous cement agents are available on the marketplace. They have recently been classified into two groups, according to the mode of preparation of dentin, prior to cementation2. A (conventional) group uses acid etching and an adhesive system for the preparation of both enamel and dentin. The other group is made up of cementation agents recently introduced in the odontological market and are known as self-adhesive resinous cements. These materials were designed for making up for some deficiencies in conventional resinous cements and glass-ionomer cements, as well as for adding some positive features to these different cements to combine them into one single product.
The formulation of self-adhesive resinous cements includes a combination of components of glassionomer and of conventional resinous cement3. Consequently, it is possible to obtain a chemical bonding in the dental substrate without previously having to resort to the hybridization technique with an adhesive system. Adhesion of self-adhesive cements is based on an acid monomer (methacrylate esters of phosphoric acid) capable of demineralizing and seeping into dentin, resulting in mechanical retention. There may also be a chemical reaction of the phosphate radical with the hydroxyapatite of tooth tissues with the vitreous particles of fluorine-aluminosilicate4. During chemical reactions, water is formed, which helps in the neutralization of the reaction itself, increasing pH from 1.0 to 6.0. The polymerization reaction of the material takes place via free radicals and can be triggered off by exposing it to visible light or via the oxy-reduction mechanism3. It is important to underscore that the process of noninternal adhesion of the radicular canal involves great technical sensitivity and that the radicular morphology has differences regarding the coronary dentin. This makes adhesion become a differentiated process on many occasions. All these considerations are relevant considering the large number of problems that may bring about failure of the final restoration. Thus, due to the short number of steps required, self-adhesive cements are an alternative for dowel cementation practices2,5.
Besides the type of resinous cement, marginal sealing between radicular walls, dowel and cement agent has also been the focus of multiple research studies as failures in marginal sealing might jeopardize the marginal integrity and the durability of the Odontological clinical procedure5-7 In this regard, it is important to watch the forms of placement of the resinous cement, as they can affect the sealing of dowel-cement-radicular dentin, and cause marginal leakage all over the adhesive interface8. The most common forms of transferring cementation into the radicular canal are by using a lentulo bur, with a centrix syringe or applying the cement onto the post surface9.
Thus, the purpose of this in vitro research is to make a qualitative and a quantitative comparison of the degree of marginal microleakage between the walls of the radicular canal, the cement and the dowel, by using placement techniques of a selfadhesive resinous cement.
MATERIALS AND METHODS
Teeth Preparation
Thirty bovine incisors were selected. The inclusion criteria for each tooth were as follows: having a minimum length of 14 mm. No curves and cracks on the surface. After the teeth were selected, they were kept in saline solution at room temperature. The crown of each tooth was separated from the root through a perpendicular section along the long axis of the tooth at the cement enamel junction by means of a j. dandy disk mounted on the micromotor assembly under abundant refrigeration conditions. With the removal of the coronary portion, direct access to the radicular canal was obtained. The biomechanical preparation of the radicular canal was done by manual technique, and by using Kerr & Hedstron files. As irrigation agents, sodium hypochlorite solution at 5% and EDTA at 17% were used. After preparation, the canal was stopped by means of lateral condensation with gutta-percha and cement filler Sealer 26 (Dentsply).
Cementation of Prefabricated Dowels
Twenty-four hours after stopping of the canals, the radicular canal was prepared with burs Length # 2 and 3 (Maillefer/Caulk/DentsplyR) with a depth of 10 mm, and a remaining 4 mm apical sealant with gutta-percha. The length of each dowel measured 10 mm inside the radicular canal and was cut at 3 mm above the cement enamel junction. The jutting portion of the dowel was sectioned with a diamond instrument # 1014 (KG Sorensen) prior to the cementation procedure. All the dowels were cemented with Rely X U100/3M ESPE as cementation agent, as per manufacturer’s instructions. The teeth were rinsed with saline solution and dried with absorbent paper. Immediately after this, a portion of the cement was set on a glass dish and was left to agglutinate for 10 seconds. Then, the teeth were randomly assigned to three groups, according to the placement technique to be used: G1 – Lentulo Bur; G2 – Centrix Syringe, and G3 – Manual Technique. After placement of selfadhesive resinous cement, the fiberglass dowel was set into the radicular canal. The excess of cement was removed with a disposable brush. The cement was photo activated for 40 seconds. (LED Freelight 2/ 3M ESPE with 800 mW/cm2) directly on the root cervical face. All the cementation procedures were undertaken by the same operator. Immediately afterwards, the teeth were temporarily restored with composite resin (Opallis A2/FGM) with no adhesive procedure and were photo activated for 40 seconds. Thirty minutes after the cementation procedure, the roots were kept in saline solution at 37°C, for seven days. Teeth were thermocycled for 1,000 cycles between 5 and 55°C (MSCT/Sao Carlos), and a dwelling time of 30 seconds.
Marginal Microleakage Tests
All the roots had their apexes sealed with sticky wax and were externally waterproofed with a layer of fluid resin (Araldite) and two layers of regular nail enamel (Blue) up to 1 mm from the edge of the restoration. Immediately after this, they were immersed in a solution of Rodhamine B at 2% at room temperature for 24 hours. After the dye was removed, the teeth were sectioned with parallel sectioning along their long axis, and their halves were analyzed by qualitative and quantitative methods.
Qualitative Analysis of the Marginal Microleakage
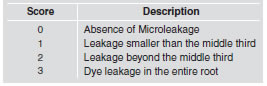
The qualitative analysis of leakage of the dye was undertaken by means of three gauged testers. For the assessment, the portion of the root with a highest degree of infiltration was selected. The penetration of the dye throughout the tooth-cement-dowel interface was measured by means of a scoring method (Table 1). The microleakage was analyzed in the cervical third, the middle third and the apical third of each root. After sectioning of all the roots, a picture of each root was taken with a digital camera, Canon Rebel XT, on a tripod, with a 3 X optical zoom, 100 macro lens, to decrease the distance between lens/object. All the images were taken under the same lighting conditions and with a ruler in mm close to the apical portion of the roots. These images were transferred to a digital archive and the leakages were measured using the Image ToolR program. This software enables magnifying an image by 2X, 4X, and 8X. After magnifying an image by 4 X, pixels (units or points that make up an image) become too obvious and thus jeopardize the quality of the image. Hence, magnifying images by 8X is limited to situations where there may be doubts regarding the dye markings and when gauging the program. The gauging of the program was undertaken to determine an equivalence between a given amount of pixels and a given distance, thus enabling the conversion of a stroke seen on a screen into a definite metric unit. For this, images were zoomed in to the maximum level and marked with lines with the help of the software. One line was equivalent to the space between two lines in the ruler, that is, one millimeter. Thus, all measures that were taken were given in millimeters. For this procedure, the portion of the root with the highest degree of infiltration was selected.
Table 1: Description of the Scores.
RESULTS
Qualitative Analysis
The values of the scores that were obtained (Table 2 and Fig. 1) were subjected to the Kruskal-Wallis statistical analysis test (p<0.05). It was possible to determine that there were no statistical differences between the cement placement techniques under analysis.
Table 2: Microleakage U100 Scores.


Fig. 1: Graphic representation of resulting scores (p<0.1659).
Marginal microleakage measures obtained via Image ToolR were statistically analyzed by ANOVA test (one-way), with a 95% degree of confidence. Such values are detailed in Table 3 and Fig. 2. It was possible to find out that there had been no statistically significant differences among the manners of placement of the self-adhesive resinous cement.
Table 3: Average of Microleakage Values (mm) and Standard Deviation.


Fig. 2: Graphic representation of Microleakage Values (mm).
DISCUSSION
Knowledge about materials prescribed for aesthetic dowel cementation is crucial for avoiding problems related to incompatibility and for increasing the clinical life of this type of adhesive restorations. All cements currently available on the marketplace have limitations, which must be taken into account at the moment of picking one cement10. The higher the number of steps required for a cementation procedure, the higher the chances of error during the relevant procedure. Thus, for this study, a self-adhesive resinous cement was selected due to the small number of steps required for the procedure, which significantly decreases the percentage of clinical failure11. Aiming at decreasing the presence of marginal microleakage, the use of adhesive materials is becoming increasingly frequent12. Microleakage may be defined as the passage of bacteria, fluids, molecules and ions from the wall of the cavity to the material used for restoration13, 14. There are several ways of demonstrating that there is presence of marginal microleakage by using radiation-marked microorganisms, chemical tracers, compressed air, SEM markers and, the most common one, organic dyes15, 16 .
Apart from their low cost, organic dyes, like the one used in this study, are the oldest methods for spotting marginal infiltration in vitro without need of chemical reaction or radiation, as is the case with chemical tracers. Yet, among their disadvantages, there is subjectivity in the quantification of penetration of dyes13 and the need to destroy the specimen used for the assessment 17, 18. The organic dye known as Rhodamine B was selected because of its good penetrating capacity, its lower coefficient of variability and its molecular dimensions of around a few nanometers. Although microorganisms have greater magnitudes, enzymes and toxins, metabolized by them, have dimensions similar to those of the dye solution19, 20.
The correlation between clinical success and in vitro study of microleakage tests was made by Torabinejad et al .21 who mention that in vitro test experiments have brought about incorrect results because simulation of in vivo conditions is limited. The exact significance of the degree of infiltration remains unknown. The same applies to how much of the infiltration is significant. Hence, it would be wise to use materials and techniques that promote a more effective sealing. The greatest difficulty encountered in in vitro studies, as is the case in this study, is the need for reproducing the clinical conditions such materials are subjected to in laboratories. One of these conditions is related to intraoral thermal shifts, which take place and bring about volumetric alterations, thus enabling the infiltration of bacteria and of other elements in the tooth-restoration interface. In specific literature, it is observed that most studies try undertaking thermal cycling, where specimens alternatively pass through solutions containing dyes, saliva or water at different temperatures and, thus, reproduce the shifts taking place at clinical level, as it was done in this study 22, 23. Nevertheless, literature shows absence of standardization as to the number of cycles specimens should be subjected to for better replicating clinical conditions. This can be clarified by the study undertaken by Veronezi et al 24 in which it was observed that there are no statistically significant differences among the values in marginal microleakage when specimens are subjected to different numbers of thermal cycles. The authors state that the major cause of cracks and, consequently, of micro-infiltration, is contraction by polymerization of resinous materials and that thermal shifts can affect the marginal adaptation of such resinous materials to the cavity walls, and can thus have some effect on the span of the micro-space that is formed. We should bear in mind that microleakage tests assess the initial capability of cavity sealing, but that they do not predict microleakage patterns through time.
For microleakage analysis, the sectioning technique of specimens was used as this technique is useful for measuring the degree of dye penetration down the dowel length17, 18.In this study, after the sectioning procedure, the portion of the root having the greatest degree of dye infiltration was selected for both qualitative and quantitative analyses. Qualitative methods are the most widely used because they are easy to carry out and because only a few pieces of equipment are needed, such as, slide projectors, magnifying glasses or low power microscopes. In case of discrepancies, our assessment may be carried out to reach consensus25. On the other hand, for the quantitative method, it is necessary to use a computer software26 and devices for copying images, so that infiltration is measured in metric units or in percentages. In this study, both methods were used, with no differences in their results whatsoever. This may be clarified by the small infiltration of dye for the different forms of cement placement being tested.
Results did not show statistically significant differences between the placement techniques of cement, irrespective of the microleakage analysis method used. Placement of cement by means of centrix syringes may be the most appropriate one. This is because this technique might promote a decrease in the number of bubbles and cracks in the layer of cement27. Bubbles can cause flaws in the bonding of the dowel and the cement. Besides, as mentioned by D’Arcangelo et al 9, the use of centrix syringes or lentulo burs will promote the highest values of resistance of the bonding. The use of lentulo burs as per manufacturers’ instructions is discouraged because it accelerates the hardening process of cement. Based on the results of this research, the lentulo bur technique did not bring about any benefit to the material as to its capability for preventing marginal microleakage. Thus, no reason was found for not following manufacturers’ instructions of use of this material. Results found in this study may be ascribed to the bonding quality promoted in the cervical third, which was always similar, irrespective of the placement technique used. As the cervical region has an easy access and a greater number of dentinal tubules, this region is more prone to having better sealing results28. In previous studies, it has already been mentioned that self-adhesive resinous cement (Rely X U100/ 3 M ESPE) brings about low levels of marginal microleakage compared to other resinous cements5,29. This might explain the results found in this study as marginal microleakage was so low that there were no statistically significant differences between the method of assessment and the forms of placement of the cement.
Although with low values, microleakage was observed in all the groups, irrespective of the placement technique and of the type of analysis used. Nevertheless, the longitudinal behavior must not be determined only by means of this test. Hence, more studies must be carried out involving mechanical tests for better reproducing intraoral conditions.
CONCLUSIONS
According to the results of this research, the following facts were observed:
• Microleakage was present in all the placement techniques;
• The degree of marginal microleakage was not altered by the resinous cement placement technique;
• There were no differences in the microleakage results, both for the qualitative and for the qualitative analyses that were undertaken.
ACKNOWLEDGEMENTS
The authors thank the CCBS/Unioeste for finantial support.
REFERENCES
1. Manning KE, Yu DC, Yu HC, Kwan EW. Factors to consider for predictable post and core build-ups of endodontically treated teeth. Part I: Basic theoretical concepts. J Can Dent Assoc 1995; 61: 696-701, 703, 705-707. [ Links ]
2. Radovic I, Monticelli F, Goracci C, Vulicevic ZR, Ferrari M. Self-adhesive resin cements: a literature review. J Adhes Dent 2008;10:251-258. [ Links ]
3. Gerth HU, Dammaschke T, Zuchner H, Schafer E. Chemical analysis and bonding reaction of RelyX Unicem and Bifix composites a comparative study. Dent Mater 2006;22: 934-941. [ Links ]
4. Yoshida Y, Van Meerbeek B, Nakayama Y, Snauwaert J, Hellemans L, Lambrechts P, Vanherle G, Wakasa K. Evidence of chemical bonding at biomaterial-hard tissue interfaces. J Dent Res 2000;79:709-714. [ Links ]
5. De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P, Van Meerbeek B. Bonding of an auto-adhesive luting material to enamel and dentin. Dent Mater 2004; 20: 963-971. [ Links ]
6. Raskin A, D’Hoore W, Gonthier S, Degrange M, Dejou J. Reliability of in vitro microleakage tests: a literature review. J Adhes Dent 2001;3:295-308.
7. Aranha AC, Domingues FB, Franco VO, Gutknecht N, Eduardo Cde P. Effects of Er:YAG and Nd:YAG lasers on dentin permeability in root surfaces: a preliminary in vitro study. Photomed Laser Surg. 2005; 23:504-508. [ Links ]
8. Vichi A, Grandini S, Davidson CL, Ferrari M. An SEM evaluation of several adhesive systems used for bonding fiber posts under clinical conditions. Dent Mater 2002;18: 495-502. [ Links ]
9. D’Arcangelo C, D’Amario M, Vadini M, Zazzeroni S, De Angelis F, Caputi S. An evaluation of luting agent application technique effect on fibre post retention. J Dent 2008; 36:235-240.
10. Maia LG, Vieira LCC. Cimentos resinosos: uma revisao de literatura. J Braz Dent Estet 2003; 2:248-262. [ Links ]
11. Miranda CB, Carvalho CF, Barros JV. Alteracao de cor de cimentos resinosos duais ativados com e sem o emprego da luz. Innov Implant J Biomater Esthet 2009; 4:25-31. [ Links ]
12. Orellana N, Ramirez R, Roig M, Giner L, Mercade M, Duran F, Herrera G. Comparative study of the microtensile bond strength of three different total etch adhesives with different solvents to wet and dry dentin (in vitro test). Acta Odontol Latinoam 2009; 22:47-56. [ Links ]
13. Kidd EA. Microleakage in relation to amalgam and composite restorations. A laboratory study. Br Dent J 1976 16;141:305-310. [ Links ]
14. Taylor MJ, Lynch E. Microleakage. J Dent 1992; 20:3-10. [ Links ]
15. Arias VG, Campos IT, Pimenta LA. Microleakage study of three adhesive systems. Braz Dent J 2004;15:194-198. [ Links ]
16. Raiden G, Cuezzo V, Gallegos P, Posleman I, Costa L. Influence of filling procedures and the partial removal of filling on the seal of root canals filled with gutta-percha and glass ionomer cement. Acta Odontol Latinoam 2007; 20:83-66 [ Links ]
17. Youngson CC, Holguin SM. Early in vitro marginal microleakage associated with different lining materials under Class II amalgam restorations. Eur J Prosthodont Restor Dent 1992;1:73-77. [ Links ]
18. Nelsen RJ, Wolcott RB, Paffenbarger GC. Fluid exchange at the margins of dental restorations. J Am Dent Assoc. 1952;44:288-295. [ Links ]
19. Wibowo G, Stockton L. Microleakage of Class II composite restorations. Am J Dent 2001;14:177-185. [ Links ]
20. Going RE, Massler M, Dute HL. Marginal penetration of dental restorations by different radioactive isotopes. J Dent Res 1960; 39:273-284. [ Links ]
21. Torabinejad M, Lee SJ, Hong CU. Apical marginal adaptation of orthograde and retrograde root end fillings: a dye leakage and scanning electron microscopic study. J Endod 1994; 20:402-407. [ Links ]
22. Wendt SL, McInnes PM, Dickinson GL. The effect of thermocycling in microleakage analysis. Dent Mater 1992; 8:181-184. [ Links ]
23. Rossomando KJ, Wendt SL Jr. Thermocycling and dwell times in microleakage evaluation for bonded restorations. Dent Mater 1995;11:47-51. [ Links ]
24. Veronezi MC, Pazim MSL, Zago PH. Influence of superficial sealant on the marginal leakage of resin composite restorations. J Dent Res 2000; 79: 355. [ Links ]
25. Zanata RL, Navarro MF, Ishikiriama A, da Silva e Souza Junior MH, Delazari RC. Bond strength between resin composite and etched and non-etched glass ionomer. Braz Dent J 1997;8:73-78. [ Links ]
26. Briso AL, Campos IT, Sundfeld RH, Rodrigues Junior AL, Pimenta LA. Microleakage of adhesively bonded cervical amalgam restorations. Am J Dent 2002 Jun;15:173-176. [ Links ]
27. Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod 2004; 30:289-301. [ Links ]
28. Siviero M, Maivazoglou MU, Camargo SEA, Camargo CHR, Valera MC. Analysis topographical, diametrical and quantitative of dentinal tubules in root channels of human teeth. Cienc Odontol Bras 2006; 9:35-43. [ Links ]
29. Hikita K, Van Meerbeek B, De Munck J, Ikeda T, Van Landuyt K, Maida T, Lambrechts P, Peumans M. Bonding effectiveness of adhesive luting agents to enamel and dentin. Dent Mater 2007;23:71-80. [ Links ]

