










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.24 no.3 Buenos Aires Dec. 2011
ARTÍCULOS ORIGINALES
Influence of lateral excursion on vestibular cervical dental abfraction
Sandra P. Palomino-Gómez1, Fabiano Jeremias1, Livia S. Finoti2, Gerson Paredes-Coz3, Dirceu B. Raveli1
1 Department of Orthodontics and Pedriatric Dentistry, Araraquara Dental School, UNESP – Univ Estadual Paulista, Araraquara, SP - Brazil.
2 Department of Oral Diagnosis and Surgery, UNESP – Univ Estadual Paulista, Araraquara, SP - Brazil.
3 Department of Restaurative Dentistry. School of Dentistry, UNMSM – National University of San Marcos, Lima - Perú.
CORRESPONDENCE Dr.Dirceu B. Raveli Departamento de Odontologia Infantil, Facultad de Odontologia de Araraquara Universidad Estadual Paulista – UNESP, Rua Humaita, 1680 Araraquara – Sao Paulo – Brasil CEP: 14801-903 e-mail: draveli@foar.unesp.br
ABSTRACT
A study was performed to evaluate the influence of mandibular lateral excursion, group function and canine guidance on vestibular cervical dental abfraction (VCDA). Thirty-six individuals of both sexes, aged 20 to 45 years, with full natural dentition with at least one tooth with VCDA were selected at the San Marcos University Clinic. We evaluated number of teeth with VCDA per side (left and right), tooth type and lateral excursive movement (canine guidance or group function) affecting it. The results showed no statistical difference (p>0.05). The tooth type most often showing VCDA was the first lower premolar, with 30.8% on the right side and 36.4% on the left. Moderate positive correlation was found between age and VCDA (R = 0.40). It is concluded that group function during lateral excursion may contribute to presence of VCDA.
Keywords: Tooth wear; Dental occlusion; Risk factors.
RESUMEN
Influencia de los movimientos excursivos laterales sobre abfracción dentaria cervico vestibular
Se realizó una investigación para evaluar la influencia de los movimientos excursivos laterales mandibulares; función de grupo y guía canina sobre abfracción dentaria cervico vestibular (ADCV). Se seleccionaron 36 individuos de ambos sexos entre 20 a 45 años de edad, con dentición natural completa que presentan como mínimo un diente con ADCV, en la Clínica Universitaria de la UNMSM. Se evaluó el número de dientes con ADCV por cada lado (derecho e izquierdo), tipo de diente, y movimiento excursivo lateral (guia canina o función en grupo) que lo influye. Los resultados denotaron no significancia estadísticas (p>0,05), el tipo de diente con mayor frecuencia a presentar ADCV fue el primer premolar inferior, 30,8% del lado derecho y 36,4% del lado izquierdo. Se encontró correlación positiva moderada entre edad y ADCV (r=0,40). Se concluye que la excursion lateral función en grupo puede contribuir a la presencia de ADCV.
Palabras clave: Desgaste de los dientes; Oclusión dental; Factores de riesgo.
INTRODUCTION
In the past, all non-carious cervical lesions were attributed to toothbrush abrasion or acid erosion, but more recently a third etiology has been introduced, which Grifo calls dental abfraction. Abfraction involves gradual micro-breakage of the dentin structure at cervical level due to forces originating at a distance, usually at the point of contact between two teeth due to premature contacts and occlusal interferences. They are wedge shaped, cervical lesions on the vestibular surface, often flat and extended, or sometimes with rough fold-like and wave-like surfaces1. Lateral forces produced during mastication may cause lesions at sites located far from the point where the force is exerted, so that their true etiology is ignored by patients and often by dentists. The problem is usually corrected by crowns, veneers or composites, which fail because they deal with the consequence rather than the cause2. It is important to understand the etiology of this type of lesion in order to prevent it. All dentists, not only specialists, should know how to treat them. Cervical-vestibular non-carious lesions have a range of morphologies. We selected a “wedge-shaped“ lesion because it is typical, unmistakable, and has the highest degree of progression3. Further studies should be conducted on incipient stages of this type of lesion in order to prevent them from progressing.
The aim of this study is to determine the influence of lateral canine guidance and group function on cervical-vestibular dental abfraction lesions in subjects in age group 40 ± 3-5 years of age.
MATERIALS AND METHODS
The study population was made up of 36 subjects aged 20-45 years with at least one tooth with VCDA. Right and left quadrants were evaluated, and type of excursive lateral movement determined. Subjects were selected at San Marcos University Clinic (UNMSM) according to the following inclusion criteria: 28 live natural permanent teeth on continuous arches; absence of restorative treatment involving cusps; Angle’s bilateral molar and canine class 1 relationship; no prior orthodontic treatment or occlusal adjustment; no signs or symptoms of bruxism; no contact in back teeth on the non-working side during lateral excursions; no manifest anxiety verified by Zung’s index4; no periodontal disease; no severe temporomandibular dysfunction according to Helkimo’s index5. Exclusion criteria were: no permanent tooth extracted except for third molars, patients under treatment for TMJ dysfunction, interference by premature contacts on the balance and working side, patients with open or skeletal bite, patients with growth syndromes or anomalies.
The clinical examination was done on a dental chair with good lighting. Dental abfraction lesions were diagnosed using a probe, seeking wedge-shaped subgingival and/or supragingival lesions at the cementoenamel junction. When VCDA was diagnosed, a data sheet was completed, recording the tooth with abfraction, lateral excursive movement (group function or canine guidance), for which the patient was asked to move his/her mandible to the right until edge to edge contact of canines, recording the working side. The same was done for the left side. The data were put into the SPSS software, and the statistical tests Chi square, Z-score and Pearson correlation at a 5% significance level were used to test our hypotheses.
RESULTS
We evaluated 72 quadrants: 36 right and 36 left, on 36 subjects with full natural dentition, of both sexes (20-45 years old), to determine the influence of the lateral occlusal pattern on teeth with vestibular-cervical dental abfraction. The results are described below. Regarding the ratio between presence of VCDA and lateral excursive movement on the right side, 78.6% of the subjects had group function and 21.4% had canine guidance, while in those without VCDA, group function and canine guidance were both 50%. On the left side with VCDA, 38.5% had canine guidance and 61.5% had group function, while among those without VCDA, 60% had canine guidance and 40% had group function (Table 1). The differences were not significant (p>0.05).
Table 1: Percentage of VCDA according to type of lateral excursive movement.

Regarding the number of teeth with VCDA and type of excursive movement, on the right side, the subjects with group function had an average 1.9 ± 1.48 teeth with VCDA, while those with canine guidance had an average 1.5 ± 1.43 teeth with VCDA. On the left side, subjects with a group function occlusal pattern had an average 1.8 ± 1.33 teeth with VCDA, while those with canine guidance had an average 1.3 ± 1.4 teeth with VCDA (Table 2). The differences were not significant (p>0.05). The relationship between number of teeth with VCDA and age was analyzed with the Pearson coefficient, and was found to be moderately associated (r=0.40) (Fig. 1).
Table 2: Number of teeth with VCDA per side according to type of lateral excursive movement.


Fig. 1: Relationship between number of teeth with vestibular cervical dental abfraction and age.
On the right side, a total 20 first lower premolars had VCDA (36.8%), of which 4 (26.7%) were canine guided and 16 (32%) had group function (Table 3). On the left side, a total of 20 first lower premolars had VCDA (36.4%), of which 8 (38.1%) were canine guided and 12 (35.3%) had group function (Table 4).
Table 3: Type of tooth most often affected by VCDA in occlusal patterns on the right side.
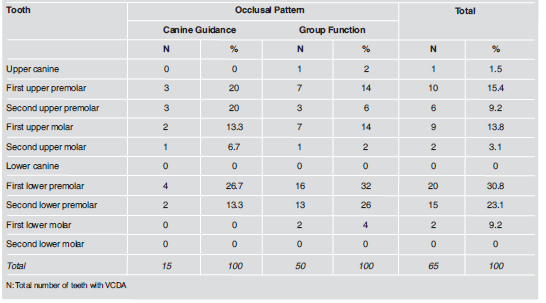
Table 4: Type of tooth most often affected by VCDA in occlusal patterns on the left side.

DISCUSSION
Human teeth are susceptible to various changes throughout life, including non-carious cervical lesions, of which a range of forms are often found in clinical practice3. Dental abfraction was the last of these to be recognized following clinical experience and evidence collected for decades leading to an understanding of the role of occlusion in its etiology6. The new hypothesis claims that occlusal load generated during mastication and bruxism produces complex vectors that may be axial and non-axial forces7,8. Axial forces consist of compression and dissipation within the periodontium causing shortening and barreling of the crown of the tooth (compressive stress), while non-axial forces create levering states that concentrate forces near the fulcrum (extensional stress). This concentration may disorganize chemical bonds of the crystalline structures of enamel and dentin7,9.
The effects of these forces during static or cyclic activity are always present when the tooth makes contact. Average tooth contact per 24 hours is 9 minutes for chewing and 17.5 minutes for swallowing (swallowing is done 1.5 times a day, with dental contact). There is dental contact only during mastication, swallowing, parafunction10. Heyman reported “tooth flexure occurs as a result of the inevitable interocclusal contact” 11. Tooth surfaces on the working side are guides for lateral jaw movements, producing patterns12,13. The two most common lateral occlusal patterns are canine guidance and group function13-17. These patterns diverge in philosophy and technique18.
Manns reports “The electromyographic activity of the masticatory muscles undergoes variation depending on its type of lateral occlusal pattern”, with reference to the fact that the activity of the elevator muscles is reduced more by canine guidance than by group function, claiming that this is due to the large number of neuronal units innervating the canine periodontium, which is represented in the upper brain centers, requiring a lower lateral mechanical stimulus to trigger the inhibitory response that protects teeth from lateral overloading18. This study evaluated the relationship between the lateral occlusal pattern and teeth with abfraction. A higher percentage of patients was found with VCDA and group function on both the right and the left sides. The highest percentage was on the right. This may be due to the fact that canine guidance dissipates damaging lateral forces better than group function does18. Samplonius found that 30% of 20 premolars with VCDA studied had group function.
In our study, the difference in percentages between the right and left sides is due to the fact that most people masticate unilaterally, more frequently on the right side19-23. Confirming the influence of the occlusal pattern on the presence of abfracted teeth, calculation of the average number teeth with VCDA was found to be higher on both left and right sides in subjects with group function. When there was canine guidance, the average was lower on both sides. Dawid also found multiple wedge-shaped lesions in patients with group function24. However, Wood found that the reduction of occlusal load with adjustment of lateral movement in patients with group function did not produce a significant impact on the progression of these lesions1. Several authors have suggested that prevalence of vestibular cervical dental abfraction increases with age, possibly due to increased fragility of enamel and dentin1,20,25,26. This study found a moderate positive correlation between age and number of teeth with VCDA. Lower first premolars most frequently had VCDA. Heyman suggests that the higher incidence on lower premolars is due to the greater lingual inclination of the crowns and smaller crown diameter at cervical level26. Samplonius19 found the highest frequency of VCDA on first upper right premolar. This may be due to the small sample used (n=20). Reyes20 evaluated 46 patients and found VCDA in most of them. Confusion in the use of terms for describing these lesions reflects the participation of secondary factors in their development, including toothbrush abrasion due and acid erosion, which play an active part in the propagation of abfraction27-31
CONCLUSIONS
The frequency of lateral excursive movements with VCDA was higher with group function. The frequency of group function in subjects with vestibular cervical dental abfraction was higher for the right side. The teeth with the highest frequency of vestibular cervical dental abfraction were the first lower premolars on the right and left sides. Age is moderately correlated to VCDA.
REFERENCES
1. Wood ID, Kassir ASA, Brunton PA. Effect of lateral excursive movements on the progression of abfraction lesions. Oper Dent 2009;34:273-279. [ Links ]
2. Piotrowski BT, Gillette WB, Hancock EB. Bradley T, Willian B, Everett B. Examining the prevalence and characteristics of abfraction like cervical lesions in a population of U.S. veterans. J Am Dent Assoc 2001;132:1694-1701. [ Links ]
3. Levitch LC, Bader JD, Shugars DA, Heymann HO. Non-carious cervical lesions. J Dent 1994;22:195-207. [ Links ]
4. Zung WWK, Cavenar JO,Jr. Assessment scales and techniques. In: Kutash IL, Schlesinger LB, editors. Handbook on stress and anxiety. San Francisco: Jossey-Bass; 1980. p. 348-363. [ Links ]
5. Helkimo M. Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Sven Tandlak Tidskr 1974; 67:101-121. [ Links ]
6. Lyttle HA, Sidhu N, Smyth B. A study of the classification and treatment of noncarious cervical lesions by general practitioners. J Prosthet Dent 1998;79:342-346. [ Links ]
7. Lee WC, Eakle WS. Stress-induced cervical lesions: Review of advances in the past 10 years. J Prosthet Dent 1996;75:487-494. [ Links ]
8. Tsiggos N, Tortopidis D, Hatzikyriakos A, Menexes G. Association between self-reported bruxism activity and occurrence of dental attrition, abfraction, and occlusal pits on natural teeth. J Prosthet Dent 2008;100:41-46. [ Links ]
9. Takehara J, Takano T, Akhter R, Morita M. Correlations of noncarious cervical lesions and occlusal factors determined by using pressure-detecting sheet. J Dent 2008;36:774-779. [ Links ]
10. Graehn G, Muller HH. Keilformige defekte an tierzahnen. Dtsch Zahn Mund Kieferheilkd Zentralbl 1991;79:441-449. [ Links ]
11. Heyman H, Sturdivant J, Bayne S. Examining tooth flexure effects on cervical restorations: a two-year clinical study. J Am Dent Assoc 1991;122:41-47. [ Links ]
12. Ramfjord SP, Ash MM. Oclusion. 2da ed. Mexico: Nueva Ed Interamericana;1980. [ Links ]
13. Gross MG. La oclusion en odontologia restauradora. 1ra ed. Barcelona: Labor; 1986. [ Links ]
14. Thornton L. Anterior guidance: Group function/canine guidance: A literature review. J Prosthet Dent 1990;64:479-482. [ Links ]
15. Korioth KT. Frecuencia de contactos dentarios oclusales durante la posicion mandibular de intercuspidacion y dos posiciones laterales funcionales en individuos con denticion natural completa. Tesis para optar el Titulo de Cirujano dentista ,Tesis UPCH 1984. [ Links ]
16. Abdullah A, Sherfudhin H, Omar R, Johansson A. Prevalence of occlusal tooth wear and its relationship to lateral and protrusive contact schemes in a young adult Indian population . Acta Odonto Scand 1994;522:191-197. [ Links ]
17. Vasudeva G, Bogra P, The effect of occlusal restoration and loading on the development of abfraction lesions: A finite element study. J Conserv Dent. 2008;11:117-120. [ Links ]
18. Manns A, Chanc C, Millares R. Influence of group function and canine guidance on electromyographic activity of elevator muscles. J Prosthet Dent 1987;57: 494-501. [ Links ]
19. Samplonius A. Tipo de contacto oclusal, Desarmonias oclusales y su relacion con la abfaccion cervical ACV en premolares de adultos jovenes Abril 1995. Tesis UNMSM, para optar El Titulo de Cirujano Dentista. [ Links ]
20. Reyes E, Hildebolt C, Langenwalter E, Miley D. Abfractions and Attachment Loss in Teeth With Premature Contacts in Centric Relation: Clinical Observations. J Periodontol 2009; 80:1955-1962. [ Links ]
21. Balbanela CH. Masticacion y desarrollo craneal. Acta Odont Ven 1991;29:103-108. [ Links ]
22. Martinez-Gomis J, Lujan-Climent M, Palau S, Bizar J, Salsench J, Peraire M. Relationship between chewing side preference and handedness and lateral asymmetry of peripheral factors. Arch Oral Biol. 2009;54:101-107. [ Links ]
23. Larena AJ. Modificaciones anatomicas del aparato estomatognatico condicionadas por el habito masticatorio y su relacion con el Sindrome de Disfuncion Craneo Mandibular. Tesis de doctorado, Gran Canaria-Espana 1995. <http://www.step.es/~jlarena/pepeing.htm> [consulta:1 Julio 2010]. [ Links ]
24. Dawid E, Meyer G, Schwartz P. The etiology of wedgeshaped defects: A morphological and function-oriented investigation. J Gnathology. 1991;10:49-55. [ Links ]
25. Fuller J, Wallace J. Citric acid consumption and the human dentition. JADA 1977;95:80-84. [ Links ]
26. Heyman H, Sturdivant J, Bayne S. Examining tooth Flexure effects. JADA 1991;122:41-46. [ Links ]
27. Spranger H. Investigacion sobre la genesis de las lesiones “en cuna” en La region cervical de los dientes. Quintessence Int 1995;26:149-154.
28. Lee W, Eakle S. Stress-induced cervical lesions: Review of advances in the past 10 years. J Prosthet Dent 1996;75: 487-494. [ Links ]
29. Braem M, Lambrechts P, Vanherle G. Stress induced cervical lesions. J Prostet Dent 1992;67:718-722. [ Links ]
30. Goel V, Khera S, Ralston J, Chang K. Stresses at the dentino enamel junction of human teeth-A finite element investigation. J Prosthet Dent 1991;66:451-459. [ Links ]
31. Bader JD, McClure F, Scurria MS, Shugars DA, Heyman HO. Case-control study of non-carious cervical lesions. Community Dent Oral Epidemiol 1996;24:286-291. [ Links ]

