










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.25 no.2 Buenos Aires Oct. 2012
ARTÍCULOS ORIGINALES
Prevalence of actinic cheilitis in a population of agricultural sugarcane workers
Ana M.O. Miranda1, Léo G. Soares1,2, Thiago M. Ferrari3, Denise G. Silva1, Márcio E.V. Falabella1,4, Eduardo M.B. Tinoco1,2
1 Universidade do Grande Rio Prof. José de Souza Herdy, Dental School, Duque de Caxias, Brazil.
2 Universidade Estadual do Rio de Janeiro, Dental School, Rio de Janeiro, Brazil.
3 Universidade Estadual de Maringá, Dental School, Maringá, Brazil.
4 Universidade Federal de Juiz de Fora, Dental School, Juiz de Fora, Brazil
CORRESPONDENCE Dr. Leo Soares Praca Garcia, 99 – centro. Paraiba do Sul RJ, Brazil. CEP 25850-000 dr_leog@hotmail.com
ABSTRACT
Actinic cheilitis (AC) is a pre-malignant inflammatory reaction of the lips caused by continuous exposure to solar rays. The aim of this study was to assess the prevalence of AC in a population of sugarcane workers in Brazil. 1,539 individuals who were exposed to the sun during working hours and 150 individuals who were not exposed were screened for clinical signs of AC. The sample was classified according to years of exposure to the sun, ethnicity, gender, smoking and severity of the lesion. A 9.16% (n= 141) prevalence of AC was observed among the population which had been exposed to the sun. The prevalence of AC lesions was significantly higher among individuals who had been exposed to the sun for more than 10 years than among those who had been exposed for less than 10 years, and among Caucasians and males than non-Caucasians and females. It was concluded that the severity of the lesions was associated with time of exposure to the sun.
Keywords: Actinic cheilitis; Neoplasms; Lip.
RESUMO
Prevalência de queilite actínica em uma população de trabalhadores cortadores de cana de açúcar
A queilite actinica (QA) e uma reacao inflamatoria premaligna dos labios causada pela exposicao continua aos raios solares. O objetivo deste estudo foi avaliar a prevalencia de QA em uma populacao de trabalhadores cortadores de cana no Brasil. 1.539 individuos que foram expostos ao sol durante as horas de trabalho e 150 individuos que nao foram expostos foram selecionados para sinais clinicos de QA. A amostra foi classificada de acordo com anos de exposicao ao sol, etnia, genero, tabagismo e gravidade da lesao. A prevalencia de 9,16% (n = 141) do QA foi observada entre a populacao que havia sido exposta ao sol. A prevalencia de lesoes QA entre os individuos que tinham mais de 10 anos de exposicao ao sol foi significativamente maior que individuos que tinham menos de 10, e entre os caucasianos e os homens mais do que os naocaucasianos e mulheres, respectivamente. Foi concluido que a gravidade das lesoes foi associada com o tempo de exposicao ao sol.
Palavras-chave: Queilite actinica; Neoplasias; Labios.
INTRODUCTION
Continuous exposure to solar rays without protection may cause several irreparable forms of damage to human skin. Actinic cheilitis (AC) is an inflammatory reaction of the lips caused by continuous exposure to solar rays1, which is frequently found in Caucasian males over 50 years of age. Its occurrence is more common on the lower lip2, with symptoms such as scaling, drying, cracks, atrophy, ulcers and dysplasia. It is defined as a degenerative condition of the lining epithelium caused by ultraviolet radiation of the sun on the lips3. Diagnosis of the AC is based mainly on clinical and histopathological findings. Due to a higher incidence of the solar rays on lower lips, they are more frequently affected than the upper lips. Initially, the lips are rough and dry; later stretch marks or small perpendicular grooves can appear within the bordering area of the skin and the lips. In severe cases, diffuse edema on the lips may cause loss of the border area between the lips and skin4. The histopathological appearance shows an increase in the keratin layer with orthokeratosis, atrophy of the cells in the prickly layer, and inflammatory infiltrate in the connective tissue producing loss of collagen5. Generally, no symptom is perceived with this condition, although a persistent sensation of dryness, burning, itching and pain can occur6. In its acute form, which is less common and results from intense exposure to the sun, AC may involve the presence of ulcers, blisters and crust. Usually the condition is self-limiting and subsides after the etiologic agent ceases7. The chronic form appears due to continuous daily exposure to the sun and is most commonly found in individuals with very long-term exposure to the sun, such as field workers and fishermen8.
AC can develop into squamous cell carcinoma of the lips9 and it is estimated that 95% of the cases of lip cancer originate from it. The appearance of erythematous areas, cracks, ulceration and bleeding on the injury are important signs of probable cancer10. There is disagreement regarding the need for biopsies in cases of AC, even though some authors report that in moderate and severe cases, biopsies are recommended. Some authors have found no correlation between clinical appearance and histological aggressiveness, and therefore suggest that biopsies should be performed in all cases due to the great risk of malignization3. Markpoulos et al.5 described 65 cases of AC, where all the individuals were Caucasians, and observed that 11 were squamous cell carcinomas. Among the factors that influence the development of AC are the frequency of exposure to the sun, intensity of the sun rays and the degree of pigmentation of the skin. In recent years, the extensive use of fossil fuel in the world has led to environmental problems with worldwide consequences. The search for alternative technologies has stimulated the growth and development of sugarcane plantations, which provide the primary components for the production of ethanol. Ethanol is believed to be less harmful to the environment than fossil fuel products and the cultivation of sugarcane has received increasing attention in many countries, including developing countries like Brazil. Large areas of sugarcane plantations are now seen throughout the country, and the number of field workers recruited has increased accordingly. Therefore the incidence of AC among populations at high risk for this condition can be expected to increase dramatically if no specific programs to diagnose and prevent AC are planned9.
The aim of this study was to assess the prevalence of actinic cheilitis in a rural population of agricultural sugarcane workers in Paranacity, Brazil.
MATERIAL AND METHODS
A cross-sectional study was conducted among workers at a private sugarcane mill in Paranacity, Brazil, in order to assess the frequency and distribution of actinic cheilitis. 1539 individuals, 978 (63.54%) male and 561 (36.46%) female, mean age 34.56 years (}9.50), were recruited from a total population of 1950 workers, representing almost 79% of the workers at the mill. The individuals recruited were clinically examined between August and September 2008, when they attended their periodic medical examinations. All those individuals were field workers and experienced long exposure to solar rays during working hours. A control group consisting of 150 workers from the same company, who did administrative work only and had never worked under constant exposure to the sun, was recruited for comparison purposes. The study was approved by the Unigranrio Research and Ethics Committee and all individuals signed an informed consent. All individuals were clinically examined by the same trained examiner, who had an intra-individual kappa coefficient of 0.87. Individuals with suspected AQ lesions were photographed using a digital camera (Nikon Coolpix S560, Nikon Inc., Japan) and clinically reexamined on another day by the same examiner in order to confirm the diagnosis. The lesions were classified as mild, moderate or severe, according to Silva et al.11.
a) mild: presence of dryness and scaling (Fig. 1).
b) moderate: presence of dryness and exacerbated scaling, accompanied by cracks. (Fig. 2).
c) severe: hardening of the lip, loss of limits between skin and semi mucosa, presence of ulcers and crusts, beyond the alterations that occur in the mild and moderate cases (Figs. 3 and 4).

Fig. 1: Patient with light Actinic Cheilitis with dryness and scaling.

Fig. 2: Patient with moderate Actinic Cheilitis with dryness and exacerbated scaling, accompanied by cracks.

Fig. 3: Patient with severe Actinic Cheilitis with hardening of the lip and presence of crusts.

Fig. 4: Patient with severe Actinic Cheilitis with loss of limits between skin and semi mucosa.
In addition, data on ethnicity, number of years of exposure to the sun and smoking were recorded during the clinical examination for comparison purposes. All lesions classified as moderate and severe were referred for biopsies and received follow-up treatment. Means, proportions and 95% confidence intervals (95% CI) were calculated, and differences between proportions among groups were calculated using Fischer´s exact test (p<0.05).
RESULTS
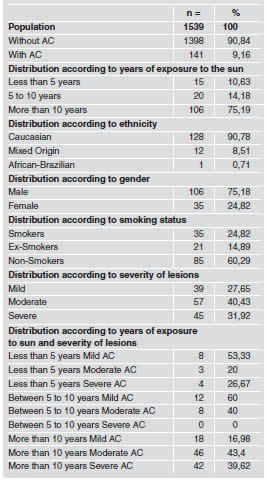
Prevalence of AC among individuals in the study population according to years of exposure to the sun, ethnicity, gender, smoking and severity of the lesion is shown in Table 1. AC prevalence of 9.16% (n= 141) was found in the population which had been exposed to the sun during working hours, while no case was found among the 150 individuals in the control group (p<0.05); 43.98% (n=677) of the individuals examined were Caucasians, 8.05% (n=124) were African-Brazilians, and 47.97% (n=738) could not be classified as belonging to either group because they were of mixed ethnicity, such as Amerindian and Asian. The prevalence of AC lesions among individuals who had more than 10 years of exposure to the sun was significantly higher (p<0.05) than among individuals who had less than 10 years of exposure. Among the individuals with AC lesions, 90.78% (n=128) were Caucasians, 0.71% (n=1) was African-Brazilian and 8.51% (n=12) were of mixed origin. The prevalence of AC among Caucasians and males was significantly higher (p=0.007; p<0.001) than among non-Caucasians and females respectively (Table 1). Individuals with more than 10 years of exposure to the sun had significantly higher frequencies of mild, moderate and severe AC lesions than individuals with less than 10 years of exposure to the sun (p<0.05).
Table 1: Frequency of AC lesions.
DISCUSSION
Brazil is the world's second largest producer of ethanol fuel and the world's largest exporter12. Brazil and the USA lead the industrial production of ethanol fuel, accounting together for 89% of the world's production in 2009. The sugarcane plantation industry has experienced enormous expansion in recent years, although it has been linked to labor abuse in some areas, according to the Brazilian government13. Some researchers have also argued that sugarcane expansion has displaced ranchers and small farmers to ecologically sensitive regions, including the Amazon, resulting in deforestation and forest degradation. In Brazil, 1 million men and women work in the sugarcane/sugar/ethanol industry. Most of them have permanent jobs at plantations, mills and distilleries. Around 200,000 have temporary (6- month) jobs cutting cane during harvest time. An average man can cut 8-12 tons of burnt cane stalks per day, a job that can take many hours14-16. As a result, this disadvantaged population is exposed to the sun 8-16 hours per day for many years, and is considered at high risk for the development of AC lesions.
Several cross-sectional studies17-19 have described the prevalence of AC in specific populations as ranging from 0.45 - 43.2%, and Caucasian males, and individuals with long-term exposure to the sun have been described as the most affected groups. Most of these studies used convenience samples which consisted of fishermen, workers and individuals seeking dental treatment and direct comparison between these studies is not possible at all. Variations between the reported prevalence can also be explained by the different sample sizes, ethnic and geographical origin of population screened, and different classification criteria of AC cases. In our study, where the prevalence of AC was 9.16%, we decided to screen a rural population of workers from a private sugarcane mill in the south of Brazil, since they represented a population at risk for AC. Although the sample comprised almost 79% of the workers from the mill, it cannot be considered representative of the whole population living in that area.
In this study the mean age of the individuals with AC lesions was 37.4 (+ 8.40) years old. This is slightly lower than what is reported in the literature, which reports affected individuals to be in 5th decade of life5, 18, 20. In addition, the prevalence of AC lesions was significantly higher in males than in females, probably reflecting larger number of males in the sample. Another explanation is that the number of males among agricultural sugarcane workers is much larger than the number of females. Corso et al.18 reported higher prevalence of AC among Caucasians, which seems to be the most susceptible ethnic group. This was the case in our sample where 90.78% of the individuals with AC lesions were Caucasians. However, AC lesions were also detected in 12 individuals of mixed ethnic origin, and one case in an African-Brazilian, showing that they are also at risk if they suffer continuous exposure to the sun for several years. In this study, individuals who had been exposed to the sun for more than 10 years had significantly higher frequencies of mild, moderate and severe AC lesions than individuals with less than 10 years of exposure. The malignant effects of the sun are cumulative and therefore exposure time is associated with the severity of the AC lesions. Despite the fact that they came from the same geographical area, none of the individuals who did administrative work in the same mill, and were not exposed to the sun during working hours, showed signs of AC. These findings are in accordance with the studies of Corso et al.18 and Silva et al.11 who also observed an association between years of exposure to the sun and severity of the lesions. In our study, the prevalence of smokers among individuals with AC lesions was relatively small (24.83%) when compared to other studies, in which prevalence was nearly 60%5 of the affected sample. The relatively small number of smokers in our total sample (28.33%) may have influenced our results.
In this study, the population screened consisted of agricultural workers who were exposed to the sun 8 hours or more per day without using any kind of sun protection. The frequency of moderate and severe AC lesions was higher among individuals who had >10 years of exposure to the sun than in individuals who had been exposed to the sun for less time. Very often, affected individuals did not know that the lesions on their lips were associated with long-term sun exposure during working hours. Therefore, programs to increase awareness among those individuals and simple prevention methods, such as the use of adequate hats and creams to block the sun rays, should be implemented to protect this population at risk for AC. Companies involved in the sugarcane/ ethanol industry should screen and control the prevalence of AQ among their agricultural workers as part of their healthcare programs.
CONCLUSION
Prevalence of AC was found among Caucasian, male, agricultural sugarcane workers in the south of Brazil, who had undergone long-term exposure to the sun during working hours. The severity of the lesions was associated with the time of exposure to the sun. To improve future research, we suggest the inclusion of histopathology results and outcome longitudinal data, using biopsy results or long-term follow-up of subjects.
1. Pennini SN, Rebello PFB, Ramos e Silva M. Queilites. J Bras Med 2000;78:104-110. [ Links ]
2. Awde JD, Kogon SL, Morin RJ. Lip cancer: a review. J Can Dent Assoc 1996;62:634-636. [ Links ]
3. Dufresne RG Jr, Curlin Mu. Actinic Cheilitis. A treatment review. Dermatol Surg 1997;23:15-21. [ Links ]
4. Lundeen RC, Langlais RP, Terezhalmy GT. Sunscreen protection fot lip mucosa: a review and update. J Am Dent Assoc 1985;111:617-621. [ Links ]
5. Markopoulos A, Albanidou-Farmaki E, Kayavis I. Actinic cheilitis: clinical and pathologic characteristics in 65 cases. Oral Dis 2004;10:212-216. [ Links ]
6. Cataldo E, Doku HC. Solar cheilitis. J Dermatol Surg Oncol 1981;7:989-995. [ Links ]
7. Manganaro AM, Will MJ, Poulos E. Actinic cheilitis: a premalignant condiction. Gen Dent 1997;45:492-494. [ Links ]
8. Kaugars GE, Pillion T, Svirsky JA, Page DG, Burns JC, Abbey LM. Actinic cheilitis. A review of 152 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88: 181-186. [ Links ]
9. Domaneschi C, Santos SG, Navarro CM, Massucato EM, Sposto MR. Queilite Actinica: Associacao entre radiacao actinica e trauma. R G O 2003;51:101-104. [ Links ]
10. Picascia DD, Robinson JK. Actinic cheilitis: a review of the etiology, differencial diagnosis and tratment. J Am Acad Dermatol 1987;17:255-264. [ Links ]
11. Silva FD, Daniel FI, Grando LJ, Calvo MC, Rath IBS, Fabro SML. Estudo da prevalencia de alteracoes labiais em pescadores da ilha de Santa Catarina. Rev Odonto Ciencia 2006;21:37-42. [ Links ]
12. Ministerio Internacional da Restauracao. Brasil e o maior exportador de etanol e segundo maior produtor mundial. 2009. Available at http://www.mir12.com.br/br/index2.php?pg=ZGVzdGFxdWUyMDA4&id=229. [ Links ]
13. UOL (Universo online). Condicao de trabalho no Brasil. 2010 Available at: http://www1.folha.uol.com.br/fsp/brasil/fc2905200827.htm [ Links ]
14. Alves F. Por que morrem os cortadores de cana. Saude e Sociedade 2006;15:90-98. [ Links ]
15. Medeiros Jr M, Araujo MI, Bacellar O, Barreto ACS, Pereira CB, Guimaraes NS. Avaliacao clinica do edema labial. Rev Bras Alergia Imunopatol 2000;23:92-98. [ Links ]
16. Oliveira EF, Silva OMP, Blachman IT, Pio MRB. Perfil epidemiologico das neoplasias orais malignas no municipio de Sao Paulo, Brasil. Rev Odontol UNESP 2005; 34:141-147. [ Links ]
17. Campisi G, Margiotta V. Oral mucosa lesions and risk habitis among men in an Italian study population. J Oral Pathol Med 2001;30:22-28. [ Links ]
18. Corso FM, Wild C, Gouveia LO, Ribas MO. Queilite Actinica: Prevalencia na Clinica Estomatologica da PUCPR. Clin Pesq Odontol 2006;2:277-281. [ Links ]
19. Cavalcante ASR, Anbinder AL, Carvalho YR. Actinic cheilitis: clinical and histological features. J Oral Maxillofac Surg. 2008;66:498-503. [ Links ]
20. Pontes HAR, Aguiar MCF, Mesquita RA, Pontes FSC, Silveira Junior JB. Imunoexpressao da proteina de reparo hMSH2 em queilite actinica e mucosa labial normal. Rev Bras. Cancerol 2005;5:23-30. [ Links ]

