










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.25 no.2 Buenos Aires oct. 2012
ARTÍCULOS ORIGINALES
Comparative study of preventive protocols in children at high cariogenic risk
María C. Martínez1, Betina Tolcachir1, Alfonsina Lescano de Ferrer1, María A. Bojanich2, Silvina R. Barembaum2, Silvia E. Calamari2, Ana I. Azcurra2
1 Social and Preventive Dentistry Department, School of Dentistry, National University of Córdoba, Argentina.
2 Oral Biology Department, School of Dentistry, National University of Córdoba, Argentina.
CORRESPONDENCE Dra. Ana I. Azcurra Oral Biology Department, Faculty of Dentistry, National University of Cordoba. Haya de la Torre SN, Pabellon Argentina Ciudad Universitaria- 5016, Cordoba, Argentina e-mail: anaazcurra@yahoo.com
ABSTRACT
The aim of this study was to compare the efficacy of two preventive protocols - fluoride gel (F) alone or combined with chlorhexidine varnishes (CHX) - on sialochemical, clinical and microbiological parameters in a group of children at high cariogenic risk. Two therapeutic-preventive protocols were applied in 73 children at high cariogenic risk (average age 6.2±1.4 years old) and clinical parameters (simplified oral hygiene index: OHIS; decayed, missing and filled teeth: dmf index; sugar intake and exposure to fluoride), as well as sialochemical parameters (salivary pH and flow, buffer capacity) and microbiological parameters (CFU/mg of dental biofilm of Streptococcus mutans group) were recorded and correlated before and after the protocols. Association was found between parameters that cause deficient control of dental biofilm: high values of OHIS index, CFU/mg dental biofilm, sugar intake and the d component of dmft index, and lower values of salivary flow rate and buffer capacity. After the protocols, a significant decrease was found in OHI-S and CFU/mg dental biofilm. No significant difference was found with children's gender and age. The association observed between OHI-S and cariogenic bacteria emphasizes the importance of prevention, especially regarding the oral health of the most vulnerable children. The early inclusion of F associated with CHX in the initial step of preventive and therapeutic protocols would provide benefits regarding oral microbe control while children acquire new habits of oral hygiene.
Key words: Dental caries susceptibility; Children; Saliva; Fluoride; Chlorhexidine.
RESUMEN
Estudio comparativo de protocolos preventivos en niños de alto riesgo cariogénico
El objetivo de este trabajo fue evaluar la eficacia de dos protocolos preventivos - fluoruro (F) solo o combinando con clorhexidina (CHX)- sobre indicadores clinicos, sialoquimicos y microbiologicos, en una poblacion de ninos de alto riesgo cariogenico. Se aplicaron dos protocolos terapeutico-preventivos en 73 ninos en edad escolar de alto riesgo cariogenico y se determinaron y correlacionaron parametros clinicos (indice de higiene oral simplificado IHO-S, ceo-d, consumo de azucar y exposicion a fluoruros), sialoquimicos (pH y flujo salival, capacidad amortiguadora) y microbiologicos (UFC/mg de biofilm dental de Streptococcus grupo mutans) antes y despues de la aplicacion de los tratamientos. Se observo una asociacion entre los parametros que producen una deficiente control de placa bacteriana: altos valores de IHO-S, de UFC/mg biofilm dental, de consumo de azucar, del componente c del indice ceo-d y los menores valores de flujo salival y de capacidad amortiguadora. Luego de la aplicacion de los tratamientos, se observo una disminucion significativa de IHO-S y UFC/mg biofilm dental. No se observaron diferencias significativas con el genero y la edad de los ninos. La asociacion observada entre los niveles de higiene oral y de bacterias cariogenicas enfatiza la importancia de la prevencion y atencion de la salud de los ninos mas vulnerables. La incorporacion del F asociada a la CHX en la etapa inicial de los protocolos terapeutico-preventivos ofreceria tempranamente beneficios en el control microbiano mientras se incorporan habitos de higiene oral.
Palabras clave: Niños; Susceptibilidad a caries dental; Saliva; Clorhexidina; Fluoruro.
INTRODUCTION
Knowledge which has come to light in recent years regarding dental caries has led to a new paradigm and comprehensive approach to its treatment. The multifactorial etiology and complex pathogenesis of dental caries involve microbiological, histological, immune and biochemical aspects, which lead to a diagnostic criterion and therapeutic reformulation for a preventive approach. In odontopediatric clinical practices, it is essential to unify the criteria for a certain diagnosis, identifying individual children or groups of more vulnerable children. With this purpose, clinical indexes have been associated to sialochemical and microbiological tests1. The former arise from dental medical history, both personal and family histories, cultural and socio-economic context, and clinical dental-stomatological examination. Among sialochemical tests, salivary buffer capacity, pH and flow rate are considered as risk factors; while microbiological tests refer to colony-forming units and species identification2,3. Considering these indicators, a patient can be categorized as being at high or low cariogenic risk, based on which it is possible to devise preventive and therapeutic strategies tending towards the control each of the factors involved. It is therefore essential to plan preventive actions according to the needs of each group of children, thus reducing costs and improving efficacy1,4.
In general, preventive actions in children at high cariogenic risk tend to improve host resistance, control cariogenic food intake and, above all, control the pathogenic microbes5. The two latter can be managed by changing eating habits and oral hygiene. Depending on their lifestyle and family environment, children may take some time to assimilate these behavioral changes, which require intensive interaction among the child, his/her family and health care professional. While these changes are being implemented, one therapeutic action to control dental biofilm is the use of a chemical that could affect adhesion, colonization and/or bacterial metabolism, such as fluorides (F)6 and chlorhexidine (CHX)7. F has an important inhibitory action on microbial biofilm, conditioning the necessary bacterial metabolic processes for the development and maturation of dental biofilm through enzymatic inhibition4. CHX controls the microbiological load in patients, in particular reducing salivary counts for Streptococcus mutans, which is highly sensitive to it8,9. The aim of this study was to assess and compare the efficacy of two preventive protocols, one applying only F and the other combining F with CHX, on sialochemical, microbiological and clinical parameters and indexes, in a population of children at high cariogenic risk.
MATERIAL AND METHODS
The study was a randomized clinical trial on children with clinical diagnosis of high cariogenic risk (n=73, both sexes, average age 6.2±1.4 years old), who received care at the Department of Pediatric Dentistry, School of Dentistry, National University of Cordoba, Argentina. The study was approved by the Ethics Committee, School of Medical Sciences, National University of Cordoba, Argentina, and parents/guardians of all subjects signed informed consent after a detailed explanation of the protocol. No patient had any history of systemic illness, and all underwent standardized detailed examination of the oral cavity. High cariogenic risk criteria were established by means of the following clinical indicators: dental caries lesions over the past year including white spot lesions, presence of dental pits and fissures, Greene and Vermillion's oral hygiene index simplified10 (OHI-S) ≥ 0.8, sugar intake > 4 per day and low frequency of visits to the dentist11. The following parameters were determined in this high caries risk group: Microbiological parameters: counts of S. mutans group in dental biofilm collected from the lingual face of mandibular molars with a periodontal probe, which was immediately placed in sterile physiological solution in pre-weighed tubes. Samples were immediately cultivated (mg of dental biofilm collected) in duplicate, in mitis salivarius agar with bacitracin (DIFCOR, Becton Dickinson, France), incubated for 48 hr at 37oC in microaerophilic environment; colonies were counted (CFU/mg of dental biofilm). Biochemical identification was performed by means of morphological characteristics and conventional biochemical tests (DiatabsR, Doughnut Diagnoses, Denmark) 12. Sialochemical parameters: Saliva samples (stimulated by chewing a piece of 3x3 cm2 paraffin film) were collected by direct salivation between 9 and 11 a.m. for 5 min in iced graduated tubes. Patients had been advised not to eat anything for at least 2 hours before the sample collection. Salivary flow rate, buffer capacity and pH were determined immediately (OrionR pH meter, USA)2,3,13.
All children received initial preventive therapy consisting of oral hygiene techniques, dietary advice and caries inactivation. After that, they were randomly divided into two groups for the application of preventive protocols under evaluation: Group I: (n=36) received a weekly topical application of fluoride gel for four weeks (F: acidulated gel 1.23% NaF, Gelato, Deepak, USA), and Group II: (n=37) received combined therapy, alternating topical acidulated fluoride application with 1% chlorhexidine varnish, for the same period and frequency (F + CHX: Periobacter Prof, NAF, Argentina). Clinical, sialochemical and microbiological parameters were assessed again one week after the final application of the different treatments. The analysis of correspondence association required operationalization of variables and determination of levels, considering the median for the quantitative variables: level 1: lower or equal to the median; level 2: above the statistical median. For OHI-S, ≥ 0.8 values were included in level 2, while level 1 corresponded to < 0.8 values.
Statistical Analysis
Categorical variables were summarized as proportions, and comparisons of groups were made by Student's t test for paired samples, ANOVA and correspondence analysis, considering a significance level of p<0.05 (Infostat Professional, version 2007).
RESULTS
The sample was made up of 61.8% female and 39.2% male participants. Clinical, sialochemical and microbiological variables at baseline (pretreatment) are shown in Table 1.
Table 1: Clinical, sialochemical and microbiological parameters of children before treatments.
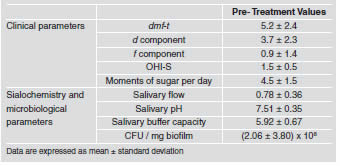
Association between the parameters studied and clinical indexes before the application of the treatment was carried out by multivariate correspondence analysis. Association was found between deficient levels of parameters that control cariogenic dental biofilm: high values for OHI-S, CFU/mg of dental biofilm, and sugar intake, and poor buffer capacity; as well as high levels of active caries with the d component of the dmf-t index and lower values of salivary flow rate. Association was also found between lower levels of OHI-S and CFU/mg of dental biofilm and better buffer capacity. Lower levels of variable active caries, the d component of the dmf-t index and higher sugar intake values were associated with higher values of salivary flow rate (inertia 37.85%). No association was observed between salivary pH and children's gender; nevertheless, lower buffer capacity was found in female patients. Regarding children's age, a tendency towards lower salivary flow rate was observed in younger children (≤ 5 years old, p=0.08), probably related to the difficulty in salivating and collecting saliva.
After both treatments, the levels of CFU/mg dental biofilm decreased significantly in relation to pretreatment values (F: p=0.004; F + CHX: p=0.001). Comparing both treatments, the decrease in CFU/mg dental biofilm was greater in Group II (F + CHX treatment) (p <0.0001) (Fig. 1). Moreover, OHIS decreased significantly with treatment (treatment F: p=0.0002, treatment F + CHX: p<0.0001) (Fig. 2). No significant difference was found between treatments. Higher values of CFU and OHI-S were observed in children over 6 years old, with more significant differences. No significant difference was found between girls and boys.

Fig. 1: Effect of therapeutic preventive protocol treatment on S. mutans levels (CFU/mg biofilm).

Fig. 2: Effect of therapeutic preventive protocol treatment on the oral hygiene index (OHI-S).
DISCUSSION
Although there is much research on cariogenic risk employing clinical, sialochemical and microbiological parameters as risk indicators at baseline and after treatment, there is very little information about young school-age population in our region. The high prevalence of caries among children warrants further research on the subject, which encouraged us to contribute this study. Clinical, microbiological and sialochemical variables were selected from bibliographic reviews2,8,11,13 and our clinical experience allows us to establish points of reference. Although there are many indexes for quantifying the presence of oral biofilm, in odontopediatric practices, the Green and Vermillion Simplified allows biofilm in primary teeth to be measured quickly and easily, and to be associated to oral hygiene status 10.
Like other researchers, we have established assessment protocols and treatments for children at high cariogenic risk adapted to our context. Such protocols are based on oral hygiene, history of dental caries, dietary habits, state of oral health, oral microbial load, salivary flow rate and pH13. In this regard, Zero et al.14 found that the model for the assessment of risk factors depends on the population studied; Peterson et al.15 reinforces this idea, suggesting that geographical area can be considered as a predictor, as well as social factors, lifestyles, and cultural and economical aspects. Many protocolized clinical trials associate the promotion and education of oral health with the application of chemical substances, combining mainly fluoride and chlorhexidine7,16,17, as well as studying the relationship between S. mutans levels and different stages of early childhood caries18. Nevertheless, and in agreement with Rijkmo et al.19, it is difficult to compare results because of the diversity of methodological conditions and heterogeneity of populations. This is the case for S. mutans counts, reported in our study as CFU/mg dental biofilm, which are not comparable with some published values, usually reported as CFU/mL saliva5,8,12. In this study we have considered the fact that CFU associated to dental biofilm are much more closely related to cariogenic risk than are planktonic bacteria in saliva.
Our study found an improvement in the level of OHIS and CFU/mg dental biofilm after treatments with more statistically significant levels when the sample was stratified according to age, which could be related to a greater efficacy of educational protocols and greater motor ability in the older group of children. Regarding the observed dmf-t index values, the high prevalence of the d component observed with a low level of the f component indicates the lack of attention to oral health among these children; moreover, high values of the d component determine, together with other parameters, a future prognosis of high caries risk20,21. These authors noted how powerful the d component is as a predictor of caries on permanent dentition and therefore, how important educational programs to recover oral health are. In our study, salivary flow rate values corresponded to high and medium risk values according to Bordoni et al.22, medium risk values observed by Sanchez- Perez et al.23 and were lower than those reported by Tukia-Humala et al.24. These findings reinforce the need for local studies describing the special characteristics of vulnerable children in our region. The salivary buffer capacity values observed in our study did not correlate with those reported in other papers according to caries risk and age25. These papers found that salivary buffer capacity and flow rate improved after tooth brushing techniques were taught, emphasizing the importance of implementing preventive and educational programs. Our results showed higher values of salivary flow rate than those reported in the literature according to the cariogenic risk observed22,26.
The decrease in S. mutans counts and improvement in oral hygiene index after fluoride application combined with CHX varnishes, added to the educational motivation and preventive and educational actions, were similar to those reported by Petersson et al.15. Many authors26,27 confirmed the benefits of applying chemical compounds in order to reduce the bacterial load and control caries, emphasizing the benefits of the application of fluoride combined with CHX varnishes in patients at high cariogenic risk. Twetman28 showed the antimicrobial properties of CHX, although its effectiveness on long-term prevention was not proved. Experimental studies with both antimicrobial agents also showed a greater effectiveness in the prevention of biofilm development, and thus of enamel demineralization29. The association observed between oral hygiene index and cariogenic bacteria counts in this study supports the need to emphasize preventive actions for maintaining oral health in the most vulnerable children; this could also demonstrate that OHI-S reflects pathogenic Streptococcus levels, although it must be remembered that dental caries is a multifactorial disease, and other factors such as oral hygiene and access to fluoridated products are also determinants of the carious process. In this sense, prevention should be based on diet control, teaching oral hygiene techniques and reinforcing host resistance. Nevertheless, including CHX during the initial phase of clinical odontopediatric actions in children at high cariogenic risk offers benefits in microbial control while dietary and oral hygiene habits are being promoted. This study shows that the application of CHX together with fluoride varnishes is an important complement to initial therapy in children at high cariogenic risk and provides better control of some indicators than does using only fluoride. Nevertheless, and considering that our work cannot be interpreted as an epidemiological study, further studies are needed to assess the efficacy on long-term prevention.
ACKNOWLEDGMENTS
This work was supported by the Secretary of Science and Technology (SeCyT) of the National University of Cordoba, No 159/07.
1. Pitts NB. How the detection, assessment, diagnosis and monitoring of caries integrate with personalized caries management. Monogr Oral Sci 2009;21:1-14. [ Links ]
2. Battellino LJ, Cornejo LS, Dorronsoro de Cattoni ST, Luna Maldonado de Yankilevich ER, Calamari SE, Azcura AI, Virga C. Oral health status evaluation of pre-school children: longitudinal epidemiologic study (1993-1994), Cordoba, Argentina. Rev Saude Publica 1997;31:272-81.
3. Cornejo LS, Brunotto M, Hilas E. Salivary factors associated to the prevalence and increase of dental caries in rural schoolchildren. Rev Saude Publica 2008;42:19-25.
4. Ekstrand J. Oliveby A. Fluoride in the oral environment. Acta Odontol Scand 1999;57:330-3.
5. Okada M, Soda Y, Hayashi F, Doi T, Suzuki J, Miura K, Kozai K. Longitudinal study of dental caries incidence associated with Streptococcus mutans and Streptococcus sobrinus in pre-school children. J Med Microbiol 2005;54:661-5.
6. Duckworth R. Fluoride in saliva and plaque following use of fluoride-containig mouthrinses. J Dent Res 1987;66:1730-4.
7. Forgie A, Paterson M, Pine C. A randomized controlled trial of caries-preventive efficacy of a chlorhexidine-containing varnish in high-caries-risk adolescents. Caries Res 2000;34:432-39.
8. Edelstein B, Tinanoff N. Screening preschool children for dental caries using a microbial test. Pediatr Dent 1989;11:129-32.
9. Matthijs S, Adriens P. Chlorhexidine varnishes: a review. J Clin Periodontol 2002;29:1-8.
10. Greene J, Vermillion J. The simplified oral hygiene in dex. J Am Dent Assoc 1964;68:7-13.
11. Maltz M, Jardim JJ, Alves LS Health promotion and dental caries. Braz Oral Res 2010;24:18-25.
12. de Carvalho FG, Silva DS, Hebling J, Spolidorio LC, Spolidorio DM. Presence of mutans streptococci and Candida spp. in dental plaque/dentine of carious teeth and early childhood caries. Arch Oral Biol 2006;51:1024-8.
13. Larmas M. Saliva and dental caries: diagnostic tests for normal dental practice. Int Dent J 1992;42:199-208.
14. Zero D, Fontana M, Lennon A. Clinical applications and outcomes of using indicators in caries management. J Dent Educ 2001;65:1126-32.
15. Peterson L, Twetman S. Efficacy of a chlorhexidine and a chlorhexidine –fluoride varnish mixture to decrease interdental levels of mutans streptococci. Caries Res 1997;31:361-5.
16. Peterson LG, Magnusson K, AnderssonH, Almquist B, Tweatman S. Effect of quarterly treatments with a chlorhexidine and fluoride varnish on proximal caries in caries-susceptible teenagers: a 3 years clinical study. Caries Res 2000;34:140-3.
17. Twetman S, Peterson L. Effect of different chlorhexidine varnish regimens on mutans streptococci levels in interdental plaque and saliva. Caries Res 1997;31:189-93.
18. Parisotto TM, Steiner-Oliveira C, Duque C, Peres RC, Rodrigues LK, Nobre-dos-Santos M. Relationship among microbiological composition and presence of dental plaque, sugar exposure, social factors and different stages of early childhood caries. Arch Oral Biol 2010;55:365-73.
19. van Rijkmo H, Truin G, van't Hof A. A meta analysis of clinical studies on the caries inhibiting effect of chlorhexidine treatment. J Dent Res 1996;75:790-5.
20. Habibian M, Roberts G Lawson M, Stevenson R, Harris S Dietary habits and dental health over the first 18 months of life. Community Dent Oral Epidemiolog 2001;29:239-46.
21. Tinanoff N, Palmer C. Dietary determinants of dental caries and dietary recommendations for preschool children. J Public Health Dent 2000;60:197-206.
22. Bordoni N. Programas preventivos. Propuesta para la organizacion de la atencion clinica. Rev Asoc Odontol Argent 1993;71: 212-22.
23. Sanchez-Perez L, Saenz-Martinez L, Irigoyen-Camacho E, Zepeda-Zepeda M, Acosta-Gio AE, Mendez-Ramirez I. Stimulated saliva flow rate patterns in children: A six-year longitudinal study. Arch Oral Biol 2009;54:970-5.
24. Tukia-Kulmala H, Tenovuo J. Intra- and inter-individual variation in salivary flow rate, buffer effect, lactobacilli, and mutans streptococci among 11- to 12-year-old schoolchildren. Acta Odontol Scand 1993;51:31-7.
25. Ligtenberg AJ, Brand HS, Bots CP, Nieuw Amerongen AV. The effect of toothbrushing on secretion rate, pH and buffer ing capacity of saliva. Int J Dent Hyg 2006;4:104-5.
26. Scheutz F, Matee MI, Poulsen S, Frydenberg M. Caries risk factors in the permanent dentition of Tanzanian children: a cohort study (1997-2003). Community Dent Oral Epidemiol 2007;35:500-6.
27. Splieth C, Steffen H, Rosin M, Welk A. Caries prevention with chlorhexidine-thymol varnish in high risk schoolchildren. Community Dent Oral Epidemiol 2000; 28:419-23.
28. Twetman S. Antimicrobials in future caries control? A review with special reference to chlorhexidine treatment. Caries Res 2004 38: 223-9.
29. Ccahuana-Vasquez RA, Cury JA. S. mutans biofilm model to evaluate antimicrobial substances and enamel demineralization. Braz Oral Res 2010;24:135-41.

