










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.26 no.1 Buenos Aires abr. 2013
ARTÍCULOS ORIGINALES
Association between signs and symptoms of temporomandibular disorders and pregnancy (case control study)
Verónica A. Mayoral1, Irene A. Espinosa1, Álvaro J. Montiel2
1 School of Stomatology, Meritorious Autonomous University of Puebla, Mexico
2 General Regional Hospital 36 of Mexico's Social Security Institute (IMSS), Puebla, Mexico
CORRESPONDENCE Mayoral Garcia Veronica Anuette 26 poniente 3511 Fraccionamiento Valle Dorado C.P. 72070 Puebla, Pue. Mexico verona_2001@hotmail.com
ABSTRACT
Temporomandibular disorders (TMD) are a combination of multifactoral etiological muscular-skeletal symptoms. Prevalence is greater in women, where sexual hormones are important in pathogenisis, and its behavior at different stages of the reproductive life of women has never been fully documented. The general objective was to determine the association between signs and symptoms of temporomandibular disorders and pregnancy. A case-control study was conducted on 66 pregnant patients who met with a medical specialist and 66 non-pregnant women paired by age, who visited the General Regional Hospital 36 of Mexico's Social Security Institute (IMSS). These patients were examined for the Temporomandibular (TMD) research project to establish the prevalence of TMD in both groups. Descriptive variables were calculated through him SPSS 17 program and the association between groups with Xi Square and Ratio Possibilities (OR), The average age was 28.23 } 5.9 years in both groups, with median gestation 32.97 weeks. Most of the participants had a domestic partner. The prevalence of TDM in the non-pregnant group was 45.5% and only 15.2% in the pregnant group (X2=14.34, p<.000). We calculated the ratio of possibilities (RP) pregnant/non-pregnant with a value of 41 with confidence intervals from 23 to 72. In conclusion, pregnancy protects women from TDM signs and symptoms. Pregnant women have a considerably lower prevalence of these disorders.
Key words: Temporomandibular Joint Disorders; Pregnancy.
Asociación entre los signos y síntomas de los trastornos temporomandibulares y el embarazo(estudio de casos y controles)
RESUMEN
Los Trastornos Temporomandibulares (TTM) se refieren a una coleccion de condiciones medicas y dentales que afectan a la Articulacion Temporomandibular (ATM), y/o musculos masticatorios, asi como estructuras vecinas. Otros autores definen los TTM como un conjunto de sintomas musculo-esqueleticos de etiologia multifactorial. La prevalencia es mayor en mujeres, donde las hormonas sexuales son importantes en la patogenesis y su comportamiento en las diferentes etapas de la vida reproductiva de las mujeres no ha sido completamente documentado. El objetivo general fue determinar la asociacion entre los signos y sintomas de trastornos temporomandibulares y el embarazo. Se realizo un estudio de casos y controles con 66 pacientes embarazadas que acudieron con medico especialista y 66 no embarazadas pareadas por edad que acudieron a consulta al HGR 36 del IMSS. Fueron exploradas por medio de los Criterios de Diagnostico para la Investigacion de los Trastornos Temporomandibulares (CDI/TTM) para establecer la prevalencia de TTM en ambos grupos. Se calculo estadistica descriptiva de las variables a traves del programa SPSS v.17 y la asociacion entre grupos con Chi cuadrada y Razon de posibilidades (OR). La edad promedio fue de 28.23 } 5.9 anos en ambos grupos, con una media de semanas de gestacion de 32.97. La mayoria de las participantes contaron con una pareja. La prevalencia de TTM en el grupo de las no embarazadas fue del 45.5% y de solo el 15.2%, en las mujeres embarazadas (X2=14.34, p<.000). Se calculo la razon de posibilidades (OR) embarazadas/no embarazadas con valor de .41 con intervalos de confianza de .23 a .72. En conclusion, el embarazo es un factor protector para presentar signos y sintomas de TTM, las mujeres embarazadas presentan una prevalencia considerablemente mas baja de dicho padecimiento.
Palabras Clave: Trastornos Temporomandibulares; Embarazo.
INTRODUCTION
Temporomandibular disorders (TMD) refer to a collection of medical and dental conditions affecting the Temporomandibular Joint (TMJ) and/or the muscles of mastication, as well as contiguous tissue components1. Other authors have described TMD as a constellation of related pathological changes that produce muscular-skeletal symptoms. These can be detected by pain associated with chewing, limited jaw movement and painful temporomandibular jaw action 2. Prevalence of TMD has been reported as almost 80% and a proportion of 3 females to each male 3.
Kuttitla establishes that women suffer more TMD that men at a rate of 3:1, without determining the age intervals 4. According to a study conducted by Slade in a Canadian population, women showed a greater prevalence of TMD signs and symptoms than men, mainly with 11.1% of women expressing muscular pain and only 4% of men expressing discomfort, with significant statistical differences (p<0.0001) 5. In relation to temporomandibular disorders in women, according to Janal, a prevalence of 10.5% in women in New York has been documented, almost all of whom (10.1%) were young women of low-income socioeconomic status 6.
The authors coincide in that Temporomandibular Disorders are of multifactorial origin, where risk factors can be genetic, physiological, traumatic or oral habits 7, among others 8-10, with a greater prevalence in females, in whom hormone variations could be a determining factor because hormones evidently play a role in etiology. 11-14. Hormonal changes include menarche, the menstrual cycle and menopause, among others; however the longestlasting hormonal change is pregnancy 15.
Pregnancy is defined as the "physiological state of women initiated with fertilization and ending in labor and birth" 16, gestation is a physiological state in which the woman undergoes important static organic, endocrinometabolic and cardiovascular changes.
The impact of hormones on pain perception has been documented by several authors. Francis Chacon talked about the difference in perception of pain between men and women and found that women have greater risk of neuropathic pain and greater prevalence of muscular-skeletal pain 2. Michelle P. Warren reported that the severity of pain is also related to the ages of the women. The onset of painful syndromes tends to occur after puberty and peaks during the reproductive years, predominating in women between the ages of 20 and 40 years 11. The tissues of the Temporomandibular Joint (TMJ) contain numerous cells with estrogen receptors, particularly the condyle, the disc, and the capsule joint and to a lesser extent, the muscles of mastication 16. These structures can be considered a target for sexual steriods, particularly estrogen, which acts on the bones with an antiresorption caused by the inhabition of osteoclastic activity, and there is great influence on the cartilage Furthermore, estrogen and progesterone can influence the content and characteristics of collagen fibers by increasing the amount of collagen type III but decreasing collagen type I; the expression of the estrogen receptors and the effect of said estrogen on ligament components is that the presence of collagen type III was related to the decrease in the perception of pain17.
Another possible hormonal factor is relaxin, which is a female hormone produced by the corpus luteum. It appears in the blood during the days prior to the menstrual cycle and sporadically during the full term of pregnancy, so that during delivery there is muscle relaxation. It also modulates muscle activity in female reproductive organs. The increase in combined systemic relaxation in pregnant women has been linked to high levels of relaxine 11. LeResche, upon studying the effects of oral contraceptives on TDM pain, found that is much higher in women at times of high estrogen concentration 18. Suarez showed that adolescents at the beginning of the menstrual cycle have a greater number of TMD signs and symptoms than those in whom where menarche is not present 14, Muscular-skeletal orofacial and symptoms related to TDM appear to improve during the period of pregnancy, mainly in the last days of the term, which was correlated with high levels of estrogen 15.
The association between pregnancy and TMD symptomology is still uncertain. Hormonal changes appear to influence the pain threshold in women and the discomfort of those suffering TMD is characterized at the muscular-skeletal level, and could be influenced by hormonal changes provoked during pregnancy, which is why the aim of this study was to identify the association between TDM and pregnancy in women who sought medical treatment at the IMSS in Puebla.
MATERIAL AND METHODS
Under the observational analytical design, we previously calculated the size of our sample, which included 66 pregnant patients seeking care for their pregnancies from medical specialists and 66 nonpregnant patients seeking medical care, both groups at the IMSS General Regional Hospital No. 36 in the city of Puebla. The selection criteria for the cases were pregnant women of any age and nonpregnant women that were paired with the case groups. All the women participating signed consent forms. Exclusion criteria for both groups were women suffering any systemic illness involving the muscular-skeletal system and/or those with any type of disability.
To diagnose TMD we used the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/ TMD), previously standardized by researcher (Kappa .78). We began with the background questionnaire and later with the clinical evaluation conducted by the same researcher in accordance with the RDC/TDM. All patients were under the same environmental conditions, in the prenatal area as well as the hospital visitor area.
We collected the information and created a database with the SPSS version 17 statistics program in order to calculate mean, descriptive, median, percentages, standard deviation statistics and for the association between groups we calculated with the Xi squared statistics test and ratio possibility (OR). The difference was significant at the 5% level.
RESULTS
From 132 patients, we obtained a median age of 28 years in both groups. The average weeks of gestation in the Pregnant Women were 32.97. Regarding couple status, 77.3% in the case group (pregnant) and 60.6% in the control group (non-pregnant) had a stable partner. In general, the demographics in both groups were similar (Table 1).
Table 1: Socio-demographic characteristics by group.

Information related to TMD signs and symptoms according to the Health Patient Questionnaire show joint click predominately in the group of non-pregnant women, diurnal bruxism was the only sign reported in a majority of pregnant women, while ear buzzing was noted to exactly the same extent in both groups. Most variables did not show statistical differences between groups (Table 2).
Table 2: Signs and symptoms according to Health Patient Questionnaire (RDC/TMD) by group.

In the clinical examination, we observed that there were more painful extraoral muscles, intraoral muscles and joint areas in non-pregnant women, with statistical significance in almost all the variables registered. Only average mouth opening capacity was the same between the groups (Table 3).
Table 3: Signs and symptoms according to clinical examination (RDC/TMD) by group.

** T test
The prevalence of temporomandibular disorders in pregnant women was three times less than in nonpregnant women (Figs. 1-2).
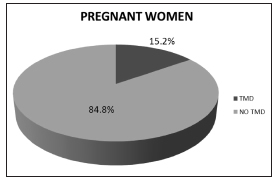
Fig. 1: Prevalence of Temporomandibular Disorders (RDC/TMD) in pregnant women.

Fig. 2: Prevalence of Temporomandibular Disorders (RDC/TMD) in non-pregnant women.
Finally we calculated the Odds ratio (OR) of the temporomandibular disorders and pregnancy, and found OR = 0.411 (CI 95% 0.234-0.720) with p<0.000. These results mean that pregnancy protects women from developing signs and symptoms of TMD.
DISCUSSION
The results of this study show that non-pregnant women have 30.3% more TMD that pregnant women, in agreement with a study conducted by Landi14, 17 where epidemiological data suggest that the symptomology begins after puberty and is lower in postmenopausal women than in fertile women. The lower prevalence of temporomandibular disorder signs and symptoms in pregnant women can be explained by virtue of pain modulation due to estrogen as well as migraines, due to the temporomandibular illness developing during the menstrual cycle, disappearing with pregnancy and reappearing after delivery, similarly to the abrupt withdrawal of exogenous estrogens2. During pregnancy the pain threshold becomes higher, explaining why pregnant women have fewer intraoral, extraoral muscular zones and joint pain than non-pregnant women. According to the study conducted by Perez13 on climacteric women, the prevalence of temporomandibular disorders is lower in the clinical examination, probably because the hormones diminish, while in the present study, during pregnancy the level of hormones is higher and the clinical examination is lower compared to non-pregnant women.
Pregnancy produces drastic changes in estrogen and progesterone and the most significant changes in both hormones occur during the second quarter, because their levels increase abruptly around the 12th week of pregnancy. Higher levels of other forms of estrogen (estradiol) are also found during the second and third quarter of pregnancy. All pain, including muscularskeletal pain in the temporomandibular region, diminishes at the beginning of the second quarter of pregnancy and remains low at nine months13. This was corroborated after an average gestation period of 33 weeks, or after the second quarter of pregnancy.
CONCLUSION
Pregnancy is a protective factor against signs and symptoms of temporomandibular disorders, pregnant women have a considerably lower prevalence of these disorders.
ACKNOWLEDGMENTS
The authors wish to acknowledge the support from Irene Espinosa de Santillana and directors of the General Regional Hospital.
1. McNeill C. Management of temporomandibular disorders: Concepts and controversies. J Prosthet Dent 1997;77:510-522. [ Links ]
2. Chacon F. Diferencias en la percepcion del dolor entre hombres y mujeres. Papel de los estrogenos. Informe Medico 2009;11:355-356. [ Links ]
3. Grau LI, Fernandez LK, Gonzalez G, Osorio NM. Algunas consideraciones sobre los trastornos temporomandibulares. Rev Cubana Estomatol 2005;42. [ Links ]
4. Kuttila M, Niemi MP, Kuttila S, Alanen P, Le Bell Y. TMD treatment need in relation to age, gender, stress and diagnostic subgroup. J Orofac Pain 1998;12:67-74. [ Links ]
5. Locker D, Slade G. Prevalence of symptoms associated with temporomandibular disorders in a Canadian population. Community Dent Oral Epidemiol 1988;16:310-313. [ Links ]
6. Janal MN, Raphael KG, Nayak S, Klausner J. Prevalence of myofascial temporomandibular disorder in US community women. J Oral Rehabil 2008;35:801-809. [ Links ]
7. Espinosa SI, Popoca HE, Estrada EB: Asociacion entre los Trastornos Temporomandibulares y tipo de Bruxismo: Estudio de casos y controles. Espana: Editorial Academica Espanola 2012;21-64.
8. Okeson JP: Tratamiento de Oclusion y afecciones Temporomandibulares. Espana. Elsevier Mosby, 2008:48-57.
9. Sosa EG. Deteccion precoz de los desordenes temporomandibulares. Colombia: Amolca 2006;28-94.
10. Suarez PA, Pellitero RB, Diaz MJ, Bidopia RD. Disfuncion temporomandibular en relacion con las maloclusiones dentarias. Correo Cientifico Medico de Holguin 2000;4(4). URL: http://www.cocmed.sld.cu/no44/n44ori2.htm [ Links ]
11. Warren PM, Fried LJ. Temporomandibular disorders and hormones in women. Cells Tissues Organs 2001;169:187- 192. [ Links ]
12. Jafek WB, Murrow WB. Otorrino-Laringologia. Espana. Elsevier Mosby, 2005;155-161.
13. Perez GE, Aldana CE, Ruelas FM, Diaz RR. Frecuencia de trastornos temporomandibulares en mujeres climatericas en el Instituto Nacional de Perinatologia. Revista ADM 2005;62:85-90. [ Links ]
14. Isselee H, De Laat A, De Mot B, Lysens R. Pressure-pain threshold variation in temporomandibular disorder myalgia over the course of the menstrual cycle. J Orofac Pain 2002;16:105-117. [ Links ]
15. LeResche L, Sherman JJ, Huggins K, Saunders K, Mancl LA, Lentz G, Dworkin SF. Musculoskeletal orofacial pain and other signs and symptoms of temporomandibular disorders during pregnancy: a prospective study. J Orofac Pain 2005;19:193-201. [ Links ]
16. Bonilla FM, Pellicer A. Obstetricia, reproduccion y ginecologia basicas. Madrid, Espana:Medica Panamericana, 2007;80-113.
17. Landi N, Lombardi I, Manfredini D, Casarosa E, Biondi K, Gabbanini M, Bosco M. Sexual hormone serum levels and temporomandibular disorders. A preliminary study. Gynecol Endocrinol 2005;20:99-103. [ Links ]
18. Rammelsberg P, LeResche L, Dworkin S, Mancl L. Longitudinal outcome of temporomandibular disorders: A 5-year epidemiologic study of muscle disorders defined by research diagnostic criteria for temporomandibular disorders. J Orofac Pain 2003;17:9-20. [ Links ]

