










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.28 no.2 Buenos Aires ago. 2015
ARTÍCULOS ORIGINALES
Ultrastructure of the surface of dental enamel with molar incisor hypomineralization (MIH) with and without acid etching
Carola B. Bozal1, Andrea Kaplan2, Andrea Ortolani3, Silvina G. Cortese3, Ana M. Biondi3
1 Deparment of Histology and Embriology. School of Dentistry, University of Buenos Aires, Argentina.
2 Deparment of Dental Materials. School of Dentistry, University of Buenos Aires, Argentina.
3 Deparment of Pediatric Dentistry. School of Dentistry, University of Buenos Aires, Argentina.
CORRESPONDENCE Dra. Ana M. Biondi Catedra de Odontologia Integral Ninos Facultad de Odontologia, UBA Marcelo T. de Alvear 2142 15oB - (1122) C.A.B.A., Argentina anamariabiondi@hotmail.com
ABSTRACT
The aim of the present work was to analyze the ultrastructure and mineral composition of the surface of the enamel on a molar with MIH, with and without acid etching. A permanent tooth without clinical MIH lesions (control) and a tooth with clinical diagnosis of mild and moderate MIH, with indication for extraction, were processed with and without acid etching (H3PO4 37%, 20") for observation with scanning electron microscope (SEM) ZEISS (Supra 40) and mineral composition analysis with an EDS detector (Oxford Instruments). The control enamel showed normal prismatic surface and etching pattern. The clinically healthy enamel on the tooth with MIH revealed partial loss of prismatic pattern. The mild lesion was porous with occasional cracks. The moderate lesion was more porous, with larger cracks and many scales. The mineral composition of the affected surfaces had lower Ca and P content and higher O and C. On the tooth with MIH, even on normal looking enamel, the demineralization does not correspond to an etching pattern, and exhibits exposure of crystals with rods with rounded ends and less demineralization in the inter-prismatic spaces. Acid etching increased the presence of cracks and deep pores in the adamantine structure of the enamel with lesion. In moderate lesions, the mineral composition had higher content of Ca, P and Cl. Enamel with MIH, even on clinically intact adamantine surfaces, shows severe alterations in the ultrastructure and changes in ionic composition, which affect the acid etching pattern and may interfere with adhesion.
Key words: Dental enamel; Hypomineralization; Acid etching.
RESUMEN
Ultraestructura de la superficie del esmalte dental con hipomineralización molar incisiva (MIH) con y sin grabado ácido
El objetivo del presente trabajo fue analizar la ultraestructura y composicion mineral de la superficie del esmalte de un molar con MIH, con y sin tratamiento de grabado acido. Se analizaron una pieza dentaria permanente sin lesiones clinicas de MIH (controles) y una pieza con diagnostico clinico de MIH leve y moderada, con indicacion de extraccion con y sin grabado acido (H3PO4 37%, 20"). Fueron procesadas para su observacion con microscopio electronico de barrido (SEM) ZEISS (Supra 40) y analisis de la composicion mineral con detector EDS (Oxford Instruments). El esmalte del control mostro superficie prismatica y patron de grabado normales. El esmalte clinicamente sano en la pieza con MIH revelo una perdida parcial del patron prismatico. La lesion leve se presento porosa con ocasionales grietas. La moderada presento mayor porosidad, con grietas de mayor tamano y presencia de gran cantidad de escamas. La composicion mineral de las superficies afectadas mostro menor contenido de Ca y P y aumento de O y C. En la muestra con MIH, inclusive con aspecto normal, las desmineralizaciones no responden a un patron de grabado, mostrando exposicion de cristales con redondeamiento en los extremos de las varillas y menor desmineralizacion en los espacios interprismaticos. El grabado acido incremento la aparicion de grietas y profundos poros en la estructura adamantina del esmalte con lesion. La composicion mineral mostro en las lesiones moderadas una mayor disminucion del contenido de Ca, P y Cl. El esmalte con MIH, inclusive en la superficie adamantina clinicamente intacta, presenta severas alteraciones ultraestruc - tu rales y cambios en la composicion ionica afectando el patron de grabado acido, que podria interferir con los mecanismos de adhesion.
Palabras clave: Esmalte dental; Hipomineralizacion; Grabado acido.
INTRODUCTION
Molar incisor hypomineralization (MIH) presents a new challenge in Pediatric Dentistry and Restorative Dentistry. Typical MIH lesions are caused by disturbance during the early mineralization stage1, affecting teeth at that chronological stage by producing enamel which is deficient in minerals, with normal content of residual amelogenin and rich in albumin2. The etiology of MIH is as yet unknown1-3. It has been suggested that ameloblasts are vulnerable during their transition from the secretion stage to maturation. Differences in the susceptibility of ameloblasts at different stages of their development cycle might explain the random distribution of lesions, since not all teeth formed during the same period are affected to the same extent3. Clinically, the defects appear as alterations in translucency and color of the affected enamel, showing as demarcated brown-yellow and/or cream-white asymmetrical opacities, mainly on permanent incisors and molars. They can lead to loss of enamel, causing high impact on the need for treatment in children and adolescents. The creamwhite colored lesions are classified as mild, following the criteria of Mathu-Muju K and Wright JT, and the brown-yellow/brown lesions are classified as moderate4, 5. Moderate lesions have higher porosity, lower mineral density throughout the entire enamel thickness, and lower mechanical strength than mild lesions6. Histologically, the microstructure is preserved, indicating normal function of the ameloblasts during the secretion stage. However, in the affected areas, the crystals are disorganized and there are enlarged inter-prismatic spaces7, suggesting that the problem may occur during the early years of life2.
Clinical studies conducted in Buenos Aires City reveal that out of 1109 children born between 1993 and 2003, with and without demand for dental healthcare and different social risk levels, the prevalence of MIH was 21.73%, increasing significantly in younger children. Patients with MIH require significantly more frequent restorative interventions and more re-treatment than those without MIH8. The results of a study conducted in 2010 on therapeutic alternatives at the Department of Comprehensive Pediatric Dentistry at the School of Dentistry of Buenos Aires University (FOUBA) revealed that 17.8% of molars with MIH required restorations with steel crowns9. Moderate and severe lesions at early ages have become a focus of attention in Pediatric Dentistry over the past decade. Clinical complications deriving from MIH include problems related to aesthetics, increased susceptibility to caries, hypersensitivity, anesthetic failure and difficulty in adhesion in techniques employed for restoration of the lesions10,11. The latter calls for a study on the microstructural features of affected tissues, in particular the enamel surface, in order to find adequate restorative alternatives. Studies reported in the literature analyze the ultrastructural and biochemical characteristics of the interior of the enamel in permanent teeth diagnosed with MIH. They have found that the affected enamel has lower mineral concentration, less organized crystalline structure, greater porosity, greater carbonate content and lower Ca/P ratio3, 12,13. The mechanical properties, hardness and modulus of elasticity of hypomineralized enamel are lower than those of normal enamel14. The ultrastructural features and mineral composition of the surface of the enamel on MIH lesions and on the clinically normal enamel on teeth affected by MIH are unknown to date.
In 1955, Buonocore proposed a strategy for improving adhesion to enamel by acid etching to create micro-roughness in the adamantine structure15. Still in use today, acid etching produces morphological patterns in the enamel which are classified as types I, II and III. In type I etching, the cores of the adamantine prisms are dissolved; in type II, the periphery of the prisms is dissolved, affecting the inter-prismatic substance. Type III does not produce deep etching and only partially removes the enamel crystals around the prisms. Effective acid etching requires a specific prismatic ultrastructure, which is not available when there is hypomineralization. Research into adhesion to hypomineralized enamel is limited; it has been reported that the affected enamel has a porous interface with fissures and fails in cohesion16. The literature does not describe the ultrastructural characteristics of the acid-etched surface of enamel with MIH lesion or the properties of the etching pattern on clinically normal enamel present in teeth affected by MIH lesions. Thus, the aims of this study were to analyze the ultrastructure and mineral composition of the surface of enamel with and without clinical lesions on a molar with MIH, with and without acid etching.
MATERIALS AND METHODS
Teeth
This study used 2 permanent human teeth: a tooth with a clinical diagnosis of MIH and a healthy tooth (control). The tooth with clinical diagnosis of MIH was a first molar with both mild and moderate hypomineralization lesions, without loss of substance. The control sample was a healthy premolar without lesions on the enamel (hypoplasia, amelogenesis imperfecta, fluorosis, caries). Both teeth were extracted by orthodontic indication, for reasons unrelated to this study. The experimental design was approved by the Ethics Committee of the School of Dentistry, University of Buenos Aires (UBACYT 208-2110/2 and UBACYT 2011-2014/3).
Sample processing
The teeth were cut in half across their free surfaces (vestibular to lingual). Each half of the tooth with clinical diagnosis of MIH had 3 clear clinically distinguishable zones: mild lesion (cream-white), moderate lesion (brown-yellow) and clinically healthy enamel, which were demarcated on the surface of the enamel as shown in Fig. 1. One half of each tooth was processed with acid etching (H3PO4 37%, time: 20") and the other half without. The halves were thoroughly rinsed with distilled water for 60 s and gently air dried, after which they were mounted and sputter-coated for observation under scanning electron microscope (SEM) ZEISS (Supra 40), and mineral composition was analyzed with an EDS detector (Oxford Instruments). The SEM has a field emission electron gun and a 3rd generation Gemini column. Magnifications of 1.0 KX, 20.0 KX and 70.0 KX were used. The mineral composition of the surface was analyzed using energy-dispersive spectroscopy with an EDS detector Oxford Instrument-INCA, which detects elements as from Boron. Both pieces of equipment belong to the Advanced Microscopy Center at the School of Exact and Natural Sciences, Buenos Aires University.

Fig. 1: Molar with MIH on which the zones of enamel with lesions have been marked: A) Moderate lesion, ochre stain; B) Mild lesion, white stain and C) Clinically intact/healthy enamel.
RESULTS
SEM examination of the adamantine surface without acid etching (Fig. 2)
The enamel on the control tooth (without hypomine - r alization) had a normal prismatic surface without structural alterations. The clinically healthy enamel on the tooth with MIH showed partial loss of the prismatic pattern, with no structural alteration. Higher magnification shows that the crystals forming the prism have more rounded ends than in the healthy control. The enamel with hypomineralization lesions did not have the typical features of prismatic enamel. The surface of the enamel from the cream-white colored (mild) hypomineralized lesion was porous, with occasional cracks and presence of different planes, giving the surface a staggered/ layered appearance. In the zone of the brown-yellow (moderate) hypominer - alization lesion, there was more porosity, larger cracks and a large quantity of scale-like lesions.
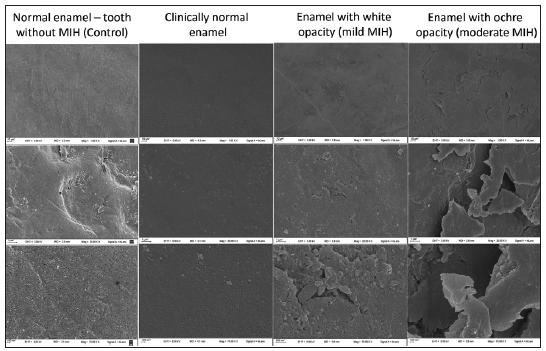
Fig. 2: SEM microphotographs of the adamantine surface without acid etching:a) Normal enamel on tooth without MIH (control): 1. Prismatic enamel surface without structural alterations. Magnification 1.0 KV; 2. Head of an enamel prism. Magnification 20.0 KV; 3. Surface of crystals forming the prism. Magnification 70.0 KV. b) Clinically normal enamel on tooth with MIH: 1. Prismatic enamel surface without structural alterations. Magnification 1.0 KV; 2. Loss of prismatic pattern image, without structural alterations. Magnification 20.0 KV. 3. Crystals forming the prism have a more rounded end than the control. Magnification 70.0 KV. c) Enamel with cream-white opacity (mild MIH): 1. Surface with slight structural alterations compared to the control. Magnification 1.0 KV; 2. Presence of different planes on the surface ("staggering") and cracks. Magnification 20.0 KV; 3. Globulous surface with small cracks. Magnification 70.0 KV. d) Enamel with ochre-brown opacity (moderate MIH): 1. Irregular surface with erosions, circularedged hollows with visible bottom and scale-shaped enamel plaques. Magnification 1.0 KV; 2. Scaling adamantine surface. Magnification 20.0 KV; 3. Very large, deep "Y"-shaped crack, without visible bottom. Magnification 70.0 KV.
Mineral composition by EDS of the enamel surface without acid etching (Fig. 3)
The mineral composition of the adamantine surfaces of the tooth with mild MIH lesion had similar Ca and P content as the control, and higher Ca content in the enamel zone that was clinically intact on the tooth with MIH diagnosis. The enamel zone with moderate lesion had lower Ca and P content than the control. All the enamel zones of the tooth with MIH diagnosis had much higher C content with lower O content than the control tooth, even in the clinically healthy enamel zone. The enamel with moderate lesion contained Mg, Zn and Rb, which were absent from the mild lesion and from clinically healthy enamel.

Fig. 3: Graphs and tables for EDS of the adamantine surface without acid etching (a%).
SEM examination of the adamantine surface with acid etching (Fig. 4)
After acid etching, the tooth with MIH diagnosis did not show the typical patterns of demineraliza - tion (type I and type II) found in normal enamel. The enamel on the tooth with MIH lost surface matter, partially exposing an underlying prismatic adamantine structure, matching a type III etching pattern. None of these demineralization match deep etching patterns (types I and II), showing exposed crystals with rounded rod ends and less deminera - liza tion of inter-prismatic spaces. Acid etching increased the amount of cracks and deep pores in the adamantine structure of the enamel with lesion.
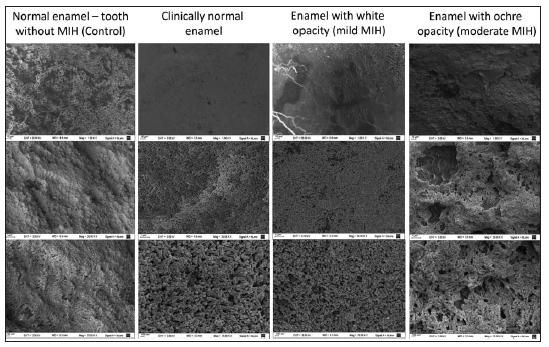
Fig. 4: SEM microphotographs of the adamantine surface with acid etching: a) Normal enamel on tooth without MIH (control): 1. Loss of surface substance with typical type I and II acid etching patterns. Magnification 1.0 KV; 2. The demineralization pattern maintains prismatic structure. Magnification 20.0 KV; 3. Prismatic pattern is maintained. Magnification 70.0 KV. b) Clinically normal enamel on tooth with MIH: 1. No demineralization pattern observed. Magnification 1.0 KV; 2. Irregular loss of substance without pattern. Magnification 20.0 KV; 3. Loss of substance with exposure of crystals. Magnification 70.0 KV. c) Enamel with cream-white opacity (mild MIH): 1. No demineralization pattern observed. Magnification 1.0 KV; 2. Irregular loss of substance without pattern. Magnification 20.0 KV; 3. Loss of substance with exposure of crystals. Magnification 70.0 KV. d) Enamel with ochre-brown opacity (moderate MIH): 1. No demineralization pattern observed. Magnification 1.0 KV; 2. Loss of deep substance with no pattern. Magnification 20.0 KV; 3. Exposure of crystals and deeper surface cracks. Magnification 70.0 KV.
Mineral composition of the acid etched enamel surface, determined by EDS (Fig. 5)
The analysis of mineral composition by EDS showed that after acid etching, the percentages of Ca and P increase while the percentage of C decreases on the surface of the enamel with mild lesion and the zone of clinically intact enamel. The ionic composition of the enamel from the moderate lesion zone was similar to that of normal enamel. It is worth noting Na and Mg were only present in the enamel of the tooth with MIH diagnosis.
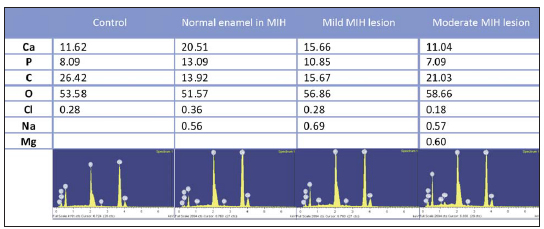
Fig. 5: Graphs and tables for EDS of adamantine surface with acid etching (a%).
DISCUSSION
Enamel with MIH, including clinically intact adamantine surfaces, has ultrastructural alterations and changes in ionic composition which affect the acid etching pattern and may interfere with adhesion. The reduction in mineral concentration in the enamel of the tooth affected by MIH observed in this study matches the results published by Fearne et al. in 20043, reporting that the reduction occurs from the dentin-enamel junction towards the subsurface zone of the enamel, which is the opposite of what happens in an incipient caries lesion in normal enamel. The surface of hypomineralized enamel contains increased proportions of C and O, as other authors have reported for the interior of hypomineralized enamel 12. This increase in C content may indicate persistence of remains of organic matter, probably due to faults in the enamel maturation period, during which proteins in the organic matrix are reabsorbed and the mineral content of the crystal increases. The substitution or loss of carbonate in HA crystals is known to increase their solubility in acid media. The persistence of carbonate could be expected to have the opposite effect16. Another possibility is that the greater porosity of this enamel enables the adsorption of foods and drinks, with the carbonate in the lesion thus coming from the breakdown of organic compounds. It should be noted that the clinically healthy enamel on the tooth with MIH diagnosis had higher Ca and P content than normal enamel. However, considered together with surface morphology, this shows that these ions would not form prismatic structures and would be more closely associated to an amorphous deposit of crystals covering the heads of the prisms, reminiscent of the aprismatic enamel which is more often found in primary teeth.
The analysis of the adamantine microstructure after acid etching of the tooth with MIH does not show type I and II demineralization patterns, which are the ones that really provide retention and clinical certainty of adhesion and marginal sealing. Nevertheless, the pattern found (type III) produces a slight superficial decalcification clinically described as "undesirable" for achieving adhesion of restorative materials to the enamel. In a systematic review, Zhu et al. (2014)17 propose that there is selective dissolution of enamel prisms or their periphery to enable the penetration of resins to facilitate micromechanical grip which will provide better adhesion. They also report that laboratory studies show a reduction in the quantity of typical patterns in the aprismatic enamel. The same concept could be applied to the findings herein, since the adamantine structure observed differs substantially from the normal, and thus a more deficient adhesion of reinforced resins could be expected. It would be interesting to test this inference with the relevant adhesive strength tests, since there is no information in the literature. The lack of available teeth may make it difficult to carry out a reliable study, since a significant sample size is necessary for obtaining data with the lowest dispersion possible. However, in the same review, Zhu et al. report that maximizing the ideal etching pattern as proposed by laboratory studies might not be clinically relevant.
The analysis of the acid etching results with relation to the mineral composition of the enamel shows that the higher C content on the hypomineralized enamel surface may interfere with the demineralization sought through the acid etching technique, which would thus be unable to create characteristic demineralization patterns. It is very likely that these atypical features of etched enamel are one of the causes of poor adhesion of restorative materials to enamel on teeth diagnosed with MIH, even in enamel zones which are clinically intact. After acid etching, the percentages of Ca and P increase, while the proportion of C decreases on the surface of enamel with mild lesions and zones of clinically intact enamel. This may indicate a deficiency in demineralization caused by phosphoric acid on the adamantine surface. The higher C content observed on the surface of hypomineralized enamel before acid etching may interfere with the demineraliza - tion sought at the expense of Ca and P. Phosphoric acid would thus be acting differently on this enamel, creating random demineralization without a defined pattern.
It would be interesting to complement this study with an evaluation of enamel microhardness in each of the zones described and for each treatment, in order to test whether there is correspondence between their chemical and physical properties. This would be very helpful for establishing appropriate treatment protocols. In the understanding that to date, the ultrastructure features and mineral composition of the surface of the enamel affected by MIH were unknown, and in particular, that it was unknown whether there was any alteration in the ultrastructure of clinically normal enamel on teeth with MIH, we believe that the preliminary results presented herein are clinically important to pediatric dentistry, which more and more often faces the challenge of restoring teeth with MIH.
CONCLUSIONS
The variations in mineral composition observed on surfaces to which restoration materials should adhere suggest that acid etching with phosphoric acid acts differently on enamel on molars with MIH, and may interfere with adhesion mechanisms. The results hereof reveal that the enamel on molars with MIH, including any clinically intact adamantine surfaces, produce an acid etching pattern which is incompatible with the requirements for an effective adhesive restoration technique.
ACKNOWLEDGEMENTS
This research was supported by University of Buenos Aires UBACyT Grants O068 and O200007BA. The authors wish to express their gratitude to Dra. Angela M. Ubios for her devoted assistance in microscopic photograph description.
1. Alaluusua S. Aetiology of Molar-Incisor Hypomineralization: A systematic review. Eur Arch Paediatr Dent 2010; 11:53-58. [ Links ]
2. Mangum JE, Crombie FA, Kilpatrick N, Manton DJ, Hubbard MJ. Surface integrity governs the proteome of hypomineralized enamel. J Dent Res 2010; 89:1160-1165. [ Links ]
3. Fearne J, Anderson P, Davis GR. 3D X-ray microscopic study of the extent of variations in enamel density in first permanent molars with idiopathic enamel hypomineralization Br Dent J 2004; 196:634-638. [ Links ]
4. Mathu-Muju K, Wright JT. Diagnosis and treatment of molar incisor hypomineralization. Compend Contin Educ Dent 2006; 27: 604-610. [ Links ]
5. Costa-Silva CM, Ambrosano GMB, Jeremias F, Souza JF, Mialhe FL. Increase in severity of molar-incisor hypomineralization and its relationship with the colour of enamel opacity: a prospective cohort study. Int J Paediatr Dent 2011; 21:333-234. [ Links ]
6. Crombie F, Manton D, Palamara J, Zalizniak I, Cochrane N, Reynolds E. Characterisation of developmentally hypomin eralised human enamel. Journal of Dentistry 2013; 41: 611-618. [ Links ]
7. Ortolani A, Cortese S, Argentieri A, Biondi A. Prevalence of Molar Incisor Hypomineralization in the City of Buenos Aires (Abstract) International Association for Dental Research. 90th IADR General Session. URL: http://iadr.confex.com/iadr/2012rio/webprogram/Paper162193.html [ Links ]
8. Kotsanos N, Kaklamanos EG, Arapostathis K. Treatment management of first permanent molars in children with Molar-Incisor Hypomineralisation Eur J Paediatr Dent 2005; 6: 179-184. [ Links ]
9. Biondi, AM; Cortese SG; Ortolani AM. Therapeutic alternatives in children with Molar Incisor Hypomineralisation (Abstract) International Association for Dental Research. 88th IADR/AADR/CADR General Session. URL: http://iadr.confex.com/iadr/2010barce/preliminaryprogram/abstract_139639.htm [ Links ]
10. Fagrell T, Lingstrom P, Olsson S, Steiniger F, Noren J. Bacterial invasion of dentinal tubules beneath apparently intact but hypomineralized enamel in molar teeth with molar incisor hypomineralization. Int J Paediatr Dent 2008; 18: 333-340. [ Links ]
11. William V, Burrow MF, Palamara JE, Messer LB. Microshear bond strength of resin composite to teeth affected by molar hypomineralization using 2 adhesive systems. Pediatr Dent 2006; 28: 233-241. [ Links ]
12. Jalevik B. Enamel hypomineralization in permanent first molars. A clinical, histo-morphological and biochemical study. Swed Dent J 2001; 1-86. [ Links ]
13. Jalevik B, Odelius H, Dietz W, Noren J. Secondary ion mass spectrometry and X-ray microanalysis of hypomineralized enamel in human permanent first molars. Arch Oral Biol 2001; 46: 239-247. [ Links ]
14. Suckling GW, Nelson DG, Patel MJ. Macroscopic and scanning electron microscopic appearance and hardness values of developmental defects in human permanent tooth enamel. Adv Dent Res 1989; 3: 219-233. [ Links ]
15. Buonocuore M. A Simple Method of Increasing the Adhesion of Acrylic Filling Materials to Enamel Surfaces JDR 1955; 34:849-853. [ Links ]
16. Waetherell JA., Deutsch D, Robinson C and Halls Worth AS. Fluoride concentrations in developing enamel. Nature 1975; 256:230-232. [ Links ]
17. Zhu JJ, Tang ATH, Matinlinna JP, Hagg U. Acid etching of human enamel in clinical applications: A systematic review. J Prosthet Dent 2014; 112:122-135. [ Links ]

