










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.29 no.1 Buenos Aires Apr. 2016
ARTÍCULOS ORIGINALES
Dental bleaching with ozone: effects on color and enamel microhardness
Manuella S.C.A. Santana1, Enrico C. Bridi1, Ricardo S. Navarro2, Carlos J. de Lima2, Adriana B. Fernandes2, Flávia L.B. do Amaral1, Fabiana M. G. França1, Cecilia P. Turssi1, Roberta T. Basting1
1 São Leopoldo Mandic Institute and Dental Research Center. Campinas, São Paulo, Brazil.
2 Institute of Biomedical Engineering of Camilo Castelo Branco University, São José dos Campos, São Paulo,Brazil.
CORRESPONDENCE Profa. Dra. Roberta Tarkany Basting Faculdade de Odontologia e Instituto de Pesquisas Sao Leopoldo Mandic Departamento de Odontologia Restauradora - Dentistica Rua Jose Rocha Junqueira, 13. Bairro Swift, Campinas – SP CEP: 13045-755 BRAZIL rbasting@yahoo.com
ABSTRACT
The aim of this in vitro study was to evaluate the effects of dental bleaching with ozone (O3) on color change and enamel microhardness. Enamel blocks (3 x 3 x 3mm) were randomly distributed for treatments (n=10). Color change (ΔE) and Knoop microhardness of the enamel blocks were evaluated before and after the following treatments: C – deionized water (control); HP – 37.5% hydrogen peroxide (Pola Office+/ SDI); PLA – placebo gel; O3 – ozone; and O2 – oxygen. Four 8-minute applications were used for HP and PLA, and one 19-minute application for O3 and O2.One-way ANOVA revealed that ΔE was not significantly influenced by the treatment (p = 0.112). For the treatments with HP, PLA, O3 andO2, ΔE was greater than 3.3. The paired t test showed significant decrease in microhardness after treatments (p < 0.001) but no significant difference between treatments (ANOVA; p = 0.313). Dental bleaching treatments with O3, HP, O2 and PLA induced enamel color changes that may be clinically discernible, although enamel microhardeness decreased.
Key words: Hydrogen peroxide; Ozone; Tooth bleaching.
RESUMO
Clareamento dental com ozônio: efeitos na cor e na microdureza do esmalte
O objetivo deste estudo in vitro foi avaliar os efeitos do clareamento dental com ozônio (O3) quanto à alteração de cor e microdureza do esmalte. Blocos de esmalte (3 x 3 x 3mm) foram aleatoriamente distribuídos entre os tratamentos (n=10). Alteração de cor (ΔE) e microdureza Knoop foram avaliados antes e após cada um dos seguintes tratamentos: C – água deionizada (controle); PH – peróxido de hidrogênio a 37,5% (Pola Office+/ SDI); PLA – gel placebo; O3 – ozônio; O2 – oxigênio. Quatro aplicações de PH e PLA foram realizadas por 8 minutos cada e uma aplicação de O3 e O2 foram realizados por 19 minutos em cada bloco de esmalte. ANOVA a um critério mostrou que os valores de ΔE não foram significativamente influenciados pelo tratamento (p = 0,112). Para os tratamentos com PH, PLA, O3 e O2, o ΔE foi maior que 3,3. O teste t pareado mostrou diminução significativa dos valores de microdureza no final do tratamento quando comparado com o tempo baseline (p < 0,001), mas não houve diferença significativa entre os tratamentos (ANOVA; p = 0,313). O tratamento com O3, PH, O2 e PLA levou a alteração de cor do esmalte clinicamente perceptível, embora tenha sido observada diminuição da microdureza do esmalte com a realização dos tratamentos.
Palavras-chave: Peróxido de hidrogênio; Ozônio; Clareamento dental.
INTRODUCTION
With the aim of improving smile esthetics, in-office bleaching treatment or at-home techniques using individual trays have been developed to treat teeth with color changes.1-4 In addition to hydrogen peroxide and carbamide peroxide - the most commonly used bleaching agents - dentists have used ozone, which may or may not be used together with hydrogen peroxide.5-8 Ozone is a naturally occurring gas composed of three oxygen atoms (O3). It is a highly oxidizing agent, able to partake in diverse chemical reactions with organic and inorganic substances.9 Its clinical use is via a mixture of oxygen and pure ozone, at a rate of 0.05 - 5% ozone and 95 – 99.95% oxygen. Due to its instability, the ozone molecule must be prepared immediately prior to clinical use, as longterm storage is impossible10 . Ozone may be used safely in situations where diffusion is an important factor, such as in dental hard tissues, acting on organic substances of the tooth tissues.11
The effectiveness of short-term exposure to ozone has been shown in different studies. Tessier et al.8 used ozone for bleaching stains caused by tetracycline, finding it effective at three to five minutes at a concentration of 2100ppm + 5% and flow rate of 615cc/min1. Other studies have used ozone applica tion times of 406 or 60 seconds12 with the same concentration and flow rate. Elhamid and Mosallam7 reported the use of ozone at a concentration of 175μg/mL to 1mL3/s incorporated into a gel, for a period of 30 minutes. Zanjani et al.13 applied ozone for four minutes, although no information was provided regarding concentration and flow. Exposure to ozone has been found to reduce enamel stains by 28% after three minutes and by 56% after five minutes.8 Other studies have compared the bleaching efficacy of ozone to other techniques. Elhamid and Mosallam7 reported that an ozonized gel provided better dental bleaching than carbamide peroxide. In contrast, Manton et al.5 applied ozone for 40 seconds every four hours over a layer of carbamide peroxide solution for 52 hours of bleaching treatment, finding no significant increase in bleaching effectiveness, and less bleaching effect when it was used prior to bleaching with peroxide. Zanjani et al.13 demonstrated that hydrogen peroxide produced more color change than ozone applied for four minutes. Regarding the use of peroxides, due to the long period of close contact between the bleaching agent and the tooth and the generally inherent acidic characteristics of the product components, porosity and surface erosion may be observed,3,14-18 as well as a decrease in surface microhardness of the enamel and dentin.19-23 Using ozone for bleaching purposes may produce a lesser side-effect on microhardness, as no residual bleaching agent remains in contact with the tooth.
Thus, the aim of this in vitro study was to evaluate the effects of ozone bleaching treatment in terms of color change and microhardness of the enamel surface. The null hypotheses were: a) ozone does not promote color changes on teeth; b) ozone does not cause changes to enamel microhardness.
MATERIALS AND METHODS
Specimens were 100 blocks of human dental enamel, with 50 blocks assigned to color assessment and 50 to microhardness. For both experiments, the 50 blocks were randomly distributed and subject to five different procedures (n=10). The study factors were:
A) Five treatments: control (C) – deionized water; ozone (O3), oxygen (O2), 37.5% hydrogen peroxide (HP) and a placebo gel without 37.5% hydrogen peroxide (PLA).
B) Two evaluation times: before treatment (baseline) and after treatment.
The response variables were color change (ΔE) evaluated using the CIELab system, and microhardness measured quantitatively in Knoop hardness numbers (KHN) after staining and application of the treatment agents.
Obtaining and preparing the enamel blocks
Following approval from the Research Ethics Committee (number 838.553), twenty-five human third molars with clinically sound crowns and without cracks or stains were used. The remains of the periodontal ligament were removed and the teeth stored in 0.1% thymol solution for one to six months.24 The dental crowns were cut using a doubled-sided diamond disc (Microdont Micro Usinagem de Precisao Ltda, Sao Paulo, SP, Brazil) and low-speed handpiece (Kavo do Brasil, Joinville, SC, Brazil). Enamel blocks 3 x 3 x 3 mm were then cut starting from the palatal and buccal aspects of each crown, under deionized water cooling to prevent enamel cracks. An average four enamel blocks were obtained from each crown and stored in relative humidity at a temperature of 37o + 1o C throughout the experiment. They were randomly distributed among groups to evaluate color change and microhardness.
Preparation of the enamel blocks for staining and color analysis
In order to create stains prior to treatment,25-26 fifty enamel blocks were coated with wax (DentBras Ind. Com. Imp. Exp. de Prod. Odont. Ltda, Pirassununga, SP, Brazil) to limit the staining to surface enamel only and immersed individually in 2 ml Methyl Orange II solution (0.15 mM) for 15 days, with the solution being changed after 7 days.25-26 The 50 blocks were randomly assigned to the experimental groups (n=10) according to treatment: control (C) – deionized water; ozone (O3), oxygen (O2), 37.5% hydrogen peroxide (HP) and a placebo gel without the 37.5% hydrogen peroxide (PLA). Color was analyzed following Jaime et al.26 The blocks were photographed before and after bleaching procedures using a digital camera (Nikon D70, Nikon Factory, Ayuthaya, Thailand) and a macro lens with a built-in circular flash (Medical- NIKKOR, Tokyo, Japan). The digital camera was standardized to obtain photographs at a release speed of 1/125, diaphragm aperture F16, sensor sensitivity ISO 200, manual function with activated flash. The blocks were placed on a flat surface against a black background, with their outermost surface as parallel as possible to the horizontal plane. Images were assessed using image editing software (Photoshop CS6, Adobe Systems Ireland Ltd., San Jose, CA, USA) to generate numerical values, according to the CIELab system (Commission Internationale de l'Eclairage" - CIE). The CIELAB system was used with the parameters: L* indicating lightness, ranging from 0 (black) to 100 (white); a* representing the saturation of the red (+) and green axes (-); and yellow (+) and blue (-) represented by the b* axis.
For the microhardness experiments, 50 enamel blocks were embedded in polyester resin (Maxi Rubber, Diadema, SP, Brazil). The enamel surface was planed using a pneumatic polisher (Ecomet 250, Buehler Ltd., Lake Bluff, IL, USA) with an attached head (Buehler Automet 250, Buehler Ltd., Lake Bluff, IL, USA) containing 600 and 1200 grit aluminum oxide sandpaper (Arotec S/A Ind. e Com., Cotia, SP, Brazil). Final polishing was performed with a synthetic velvet polishing cloth (Supra, Arotec S/A Ind. e Com., Cotia, SP, Brazil) moistened with 3 μm diamond paste for metallogra - phy (Arotec S/A Ind. e Com., Cotia, SP, Brazil). Enamel microhardness analysis was performed using a digital durometer (Pantec HVS 1000, Panambra, Sao Paulo, SP, Brazil) and Knoop-type penetrator, with a static load of 25 g for five seconds. Three microhardness indentations were performed at randomly selected sites on each enamel surface at each time (before and after treatment), with each indentation separated by a distance of 200 μm. To avoid differences in the initial mean values (baseline) of enamel microhardness between groups, test specimens that presented similar microhardness values were selected. Fifty test specimens were randomly allocated to each experimental group (n=10): control (C) – deionized water; ozone (O3), oxygen (O2), 37.5% hydrogen peroxide (HP) and a placebo gel without 37.5% hydrogen peroxide (PLA).
Experimental treatments
Table 1 provides the specifications of the agents used. The pH of the agents (deionized water, HP and PLA) was measured with a pH-meter (W3B, Bel Equipamentos Analiticos Ltda, Piracicaba, SP, Brazil), using the mean of three values. The pH values were measured shortly after handling HP and PLA at baseline and eight minutes.
Table 1: Treatment agents, composition and manufacturer.
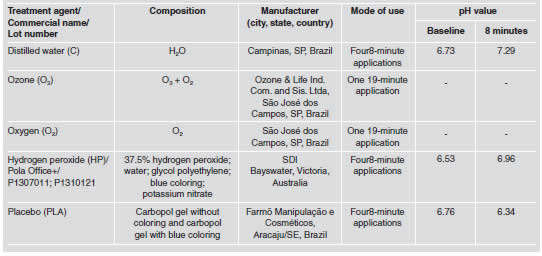
For the control group (C), 0.01 ml deionized water was applied for 8 minutes, after which it was removed from the surface with gauze, and the procedure repeated a further three times (four applications altogether). Then the enamel surface was washed with deionized water for 10 seconds and dried with gauze. For the O3 group, an ozone gas generator was used (Ozone & Life Ind. Com. and Sis. Ltda, O&L 1.5M, Sao Jose dos Campos, SP, Brazil) with an output of 80 W, connected to an oxygen cylinder via a flow control valve.27 In order to apply the gas directly to the enamel blocks, a 1L volume rectangular stainless steel box with a side opening for entrance and exit was created, so that the entire volume of the box could be filled with gas. The enamel blocks were lined up in the box, allowing simultaneous exposure of the enamel to the gas. The box was then sealed with adhesive tape and the ozonization performed in a fume cupboard. Dose was adjusted in terms of ozone concentration, in ppm, and application time in minutes. An ozone concentration of 4mg/L was used, at an oxygen flow of . l/min, as per the manufacturing guidelines. This concentration and flow-rate were based on the premise that 1mg/L corresponds to 667 ppm, and since an approximate value of 2100 ppm was desired,8,27 the closest value (4 mg/L), as per the table provided by the manufacturer was used. Total application time was 19 minutes, with the first four minutes corresponding to total filling time of the 1L box with ozone, plus 15 minutes of concentrated application. This protocol was adapted from Tessier et al.8 and Zarate et al.28 in order to maximize the effectiveness of the ozone treatment. For the O2 group, an oxygen cylinder with flow control valve was used. The gas was applied using the same stainless steel box. Dose was adjusted in terms of oxygen concentration applied, in ppm, and exposure time in minutes, with the oxygen flow rate used being . l/min (approximately 2100 ppm). Total application time was 19 minutes, with the first 4 minutes being the time taken to fill the box to a maximum capacity (1L) plus 15 minutes of oxygen application. For the HP group, a bleaching gel containing 37.5% hydrogen peroxide (Pola Office Plus, SDI Limited, Bayswater, Victoria, Australia) was used. A thin layer (0.01 ml) of gel was applied to each surface and left for eight minutes. The gel was then removed from the surface enamel and reapplied as described above for group C. For the PLA group, the gel was similar to the commercial product (HP) but lacking hydrogen peroxide. A thin layer (0.01 ml) of gel was applied to the enamel surface and left for eight minutes. The gel was removed from the surface with gauze and the procedure repeated as described above for the C and HP groups.
Following treatment application, the enamel blocks were stored in a humid environment for 12 hours before color and microhardness evaluation. Prior to statistical analysis, the data for color and microhardness were evaluated for the assumptions of normality (Shapiro-Wilk test) and homogeneity of variance (Levene test), both of which were confirmed. The initial color (parameters L*, a* and b*) and microhardness values were compared to the final values using the paired t test. Color changes (ΔE) were obtained via the CIELab system using the formulas: ΔE*= [(ΔL*)2 + (Δa*)2 + (Δb*)2 ]1/2, where ΔE is color change; ΔL = Lfinal – Linicial; Δa = afinal – ainicial; and Δb = bfinal – binicial. An ΔE value of 3 3.3 is considered discernible clinically.29
To ascertain the presence of a significant difference between the treatments applied to the enamel blocks in terms of ΔL, Δa, Δb, ΔE and ΔKHN, oneway analysis of variance (ANOVA) was used. The Tukey test was applied for multiple comparisons. Confirmation of correlation between the enamel color and microhardness values following different treatments was performed using the Pearson test. All statistical tests adopted a significance level of 5%, using SPSS 20 (SPSS Inc., Chicago, IL, USA).
RESULTS
One-way analysis of variance revealed no signi - ficant difference for ΔE values for the treatments applied to the enamel blocks (p = 0.112) (Table 2). However, with the exception of the control group (immersed in deionized water), all the other groups had ΔE values higher than 3.3. The paired t test was applied to compare initial and final Knoop microhardness values, independently of treatment. Knoop microhardness decreased significantly compared to baseline (p < 0.001) for all groups, but there was significant difference in Δ KHN values among groups (p = 0.313) (Table 2).
Table 2: Means and standard deviations for the parameters shade (ΔE) and Knoop microhardness (ΔKHN) of the enamel, according to treatment.

Pearson's test did not reveal significant correlation between ΔE values and Knoop microhardness changes (ΔKHN) (p = 0.415; r2 = -0.118) (Fig. 1).
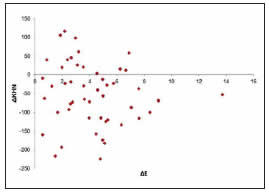
Fig. 1: Dispersion diagram of ΔE in terms of ΔKHN values.
DISCUSSION
Treatment effectiveness and safety are among the primary factors to consider when selecting a technique or bleaching agent.1 The effectiveness of a bleaching agent is evaluated by objective methods based on the L*, a*, e b* (CIELab) system, which is appropriate for scientific research and provides definitions of parameters that can be evaluated quantitatively.30-31 ΔE describes color change by including these three dimensions of color, and values above 3.3 are considered clinically discernible color changes proving the effectiveness of bleaching procedures.32-33 With the exception of the control group, all treatments in this study produced ΔE values above 3.3, confirming that they were effective in promoting color change. The teeth used to explore color change were stained prior to treatment in order to enhance the results of the treatment agents, following methods validated in previous studies.25-26 The greatest mean ΔE value was observed for ozone, although there was no significant difference with the other treatments. Other studies have also demonstrated the effecti - veness of bleaching following application of ozone.7-8 Ozone is an unstable gas that rapidly releases nascent oxygen molecules to form oxygen.11 It is a highly oxidizing agent, capable of participating in diverse chemical reactions with both organic and inorganic substances.9
The ozone molecule and, in particular, the radical hydroxyl (OH-), a non-selective oxidant formed by ozone decomposition, play an important role in the oxidation process.7,34 Ozone decomposes in aqueous solution, which is the starting point in the formation of the peroxide radical (HO2 -) and, subsequently, hydroxyl radicals (OH-). These reactions occur simultaneously, however, chromophore groups may be broken by ozone, forming smaller molecules, resulting in a tooth bleaching effect by one of three of the following fundamental mechanisms: a) bonding mechanism, which occurs via the addition of ozone by a double bond to form ozonide in the presence of non-aqueous solvents yet, once water is present, ozone is hydrolyzed to other products via cleavage of the double bond that would have occurred; b) substitution mechanism, where one atom or functional group is replaced by another one; c) cleavage mechanism, in which a carbon-carbon bond is separated to produce composite organic fragments.9 Nevertheless, ozone might be incapable of such intense penetration when compared to other peroxide-based bleaching agents, since a greater number of applications are required to achieve satisfactory results.28,35 However, in our study, the color change produced by ozone was similar to that of hydrogen peroxide, probably due to the ozone protocol used. Zarate et al.28 used a low concentration (0.5 ppm) for 20 minutes daily, which is different from our study, which used 2100 ppm. Manton et al.5 analyzed the use of ozone prior to and simultaneously with bleaching with carbamide peroxide and were unable to verify an increase in bleaching effectiveness with the combined treatment. However, they used an application time of only 40 seconds, confirming that there is variability among ozone application methods and therefore divergent results would be expected. Tessier et al.8 demonstrated the possibility of effective bleaching with ozone on even more severely stained teeth, such as in situations of staining secondary to tetracycline, using a short exposure time (3 to 5 min). Longer bleaching sessions may increase bleaching efficacy, since chromophore saturation of the dental tissues occurs gradually.36
In our study, ΔE values greater than 3.3 were also observed for the placebo and oxygen groups. Although we did not expect this color change for the oxygen group, it may be explained by oxygen being a potential oxidant, which is the basis of bleaching treatments. In accordance with Abdelaziz et al.34 although the oxidation potential of oxygen is five times lower than that of ozone, it may explain the bleaching capacity of the two gases used in this study. Additionally, ozone is 10 times more soluble than oxygen13,37 and since the samples were submitted to ozone and oxygen treatments in a dry environment, ozone may not have had the diffusion expected on the substrate and, consequently, may not have produced a difference in enamel color change. Other studies have also shown that hydrogen peroxide bleaching leads to noticeable color change.1,2,4,15,32-33,36 Its mechanism of action is based in its ability to generate active oxygen and free radicals such as perhydroxyl, which are highly reactive, extremely electrophilic and unstable, degrading organic molecules to acquire stability and creating other radicals. The radicals may easily react with most unsaturated bonds, resulting in mono- or di-hydroxylation of the bonds. These agents react with highly coupled organic molecules, which can break the coupled electrons and change the energy absorption of the molecule. Hydrogen ions (H+) are produced in the process of breaking down hydrogen peroxide, which may produce a relatively acidic environment and may affect tooth surface and subsurface integrity.38 Some bleaching products are made with low pH values in order to guarantee the stability of hydrogen peroxide, an important factor in the bleaching reaction process.16 However, consecutive bleaching sessions at high concentrations of hydrogen peroxide may lead to micromorphological and chemical changes to the enamel structure.14,33,36 Therefore, evaluation of surface microhardness is frequently used to assess the effects of bleaching agents in terms of changes to the mineral content that may occur to the tooth.18,20,23 This study found that regardless of treatment, microhardness decreased significantly, with no difference between treatments. This decrease in surface microhardness resulting from bleaching is a concern, with other studies corroborating these results when using hydrogen peroxide at high concentrations.3,18-21,23,32,39
In contrast, other studies have not observed significant changes in enamel microhardness,4,15 a difference which may be explained by the methods used, exposure time, composition, pH and concen tration of bleaching agent, as well as by differences in the evaluation time intervals of the treatment. It should be noted that although in our study the action time for the bleaching gel was similar (four 8-minute applications) to the study by Borges et al.4 (three 10- minute applications), there was a difference in the composition of the bleaching agent. We used a bleaching gel and placebo agent containing the thickening agent cabopol, which has acidic properties,40 whereas Borges et al.4 used a bleaching agent containing an acrylic thickener. In addition, in the studies by Borges et al.4 and Lia Mondelli et al.23 the specimens were stored in artificial saliva, providing the potential for remineralization from the solution to the substrate, whereas we used deionized water, which is subsaturated in terms of the mineral content of the enamel and may have led to decreased hardness.41 Tahmassebi et al.24 found no decrease in enamel microhardness using ozone, suggesting that it does not alter the mineral content of the enamel, and Duggal et al.42 observed no reduction in microhardness when using ozone with or without a fluoride product. However, our study revealed a decrease in microhardness for the group treated with ozone, probably due to the different methods used, with longer application time (19 minutes compared to a 60 seconds),24,42 and storage of the test specimens in a humid environment with deionized water, which may have reduced enamel surface hardness,41 whereas in other studies, the enamel was immersed in artificial24 or natural saliva,in which the demineralization process may be interrupted or reversed by dislocation of ionic changes on the tooth surface in favor of remineralization.42
It is well known that dental enamel becomes demineralized at a critical pH value (lower that 5.5). Bleaching agents with low pH levels may lead to significant enamel erosion,16 which, interestingly, is also seen when pH is above the critical level.43 Our study used a bleaching agent with mean pH 6.81. Bleaching agents with high concentrations of hydrogen peroxide, even at neutral pH values, are capable of demineralizing dental enamel3 while producing effective bleaching.18
Our study also found a decrease in microhardness in relation to baseline values for the control, placebo and oxygen groups. This was to be expected for the control group, where the tooth surface remained in contact with deionized water, since this solution is subsaturated with minerals in comparison to the enamel.41 For the placebo group, the results are in agreement with the findings of Basting et al.,40 in which the thickening agent in the bleaching gel and placebo was carbopol, showing a continuing demi nera li zation of the enamel and dentin with application time, even at neutral pH, causing significant changes to dental microhardness. For the oxygen group, this decrease in microhardness may be explained by the similar mechanism of action as ozone, and although oxygen is five times less oxidant than ozone, it still has high oxidation potential.34 Bocci et al.37 described how ozone can promptly react with the substrate, while oxygen generally requires a catalyzer to start its reaction. The remineralization produced by saliva and/or its substitutes containing calcium and phosphate allow maintenance of the baseline microhardness values23,41,44, which might have led to increased enamel microhardness for all groups, had artificial saliva been used to store the test specimens in this study. Moreover, although the post-bleaching period was not studied, an increase in microhardness might be expected as a result of the constant contact with saliva and/or re-mineralizing agents used in the treatments with high concentration hydrogen peroxide.21
Pearson's test did not reveal a significant correlation between color change (ΔE) and Knoop microhardness (ΔKHN). Therefore, the bleaching agent might act on the chromophores in the tooth structure to promote bleaching effectiveness, as well as altering the mineral content in an isolated manner. The limitations of this study include short exposure time and evaluation to confirm stability of the bleaching treatments and lack of an artificial saliva immersion step, which may have the potential to remineralize the enamel. Further studies are needed to evaluate the possible structural changes to the enamel following the application of ozone for dental bleaching. In conclusion, the data obtained indicate that treatment with ozone, hydrogen peroxide, oxygen and placebo cause color change to the dental enamel that may be discernible clinically and decrease in dental enamel microhardness, regardless of bleaching treatment type.
1. Basting RT, Amaral FLB, Franca FMG, Florio FM. Clinical comparative study of the effectiveness of and tooth sensitivity to 10% and 20% carbamide peroxide home-use and 35% and 38% hydrogen peroxide in-office bleaching materials containing desensitizing agents. Oper Dent 2012; 37:464-473. [ Links ]
2. de Almeida LC, Soares DG, Gallinari MO, de Souza Costa CA, Dos Santos PH, Briso AL. Color alteration, hydrogen peroxide diffusion, and cytotoxicity caused by in-office bleaching protocols. Clin Oral Investig 2015; 19:673-680. [ Links ]
3. Salomao DLF, Santos DM, Nogueira RD, Palma-Dibb RG, Geraldo-Martins VR. Acid demineralization susceptibility of dental enamel submitted to different bleaching techniques and fluoridation regimens. Oper Dent 2014; 39:178-185. [ Links ]
4. Borges AB, Zanatta RF, Barros AC, Silva LC, Pucci CR, Torres CR. Effect of hydrogen peroxide concentration on enamel color and microhardness. Oper Dent 2015; 40:96-101. [ Links ]
5. Manton DJ, Bhide R, Hopcraft MS, Reynolds EC. Effect of ozone and Tooth Mousseon the efficacy of peroxide bleaching. Aust Dent J 2008; 53: 128-132. [ Links ]
6. Can-Karabulut DC, Karabulut B. Shear bond strength to enamel after Power bleaching activated by different sources. Eur J Esthet Dent 2010; 5:382-396. [ Links ]
7. Abd Elhamid M, Mossallam R. Effect of bleaching versus repolishing on colour and surface topography of stained resin composite. Aust Dent J 2010; 55:390-398. [ Links ]
8. Tessier J, Rodriguez PN, Lifshitz F, Friedman SM, Lanata EJ. The use of ozone to lighten teeth. An experimental study. Acta Odontol Latinoam 2010; 23:84-89. [ Links ]
9. Perincek SD, Duran K, Korlu AE, Bhatiyari IM. An investigation in the use of ozone gas in the bleaching of cotton fabrics. Ozone-Sci Eng 2007; 29:325-333. [ Links ]
10. Gopalakrishnan S, Parthiban S. Ozone - a new revolution in dentistry. J Bio Innov 2012; 1:58-69. [ Links ]
11. Gupta G, Mansi B. Ozone therapy in periodontics. J Med Life 2012; 5:59-67. [ Links ]
12. Schmidlin PR, Zimmermann J, Bindl A. Effect of ozone on enamel and dentin bond strength. J Adhes Dent 2005; 7: 29-32. [ Links ]
13. Zanjani VA, Ghasemi A, Torabzadeh H, Jamali M, Razmavar S, Baghban AA. Bleaching effect of ozone on pigmented teeth. Dent Res J (Isfahan) 2015; 12: 20-24. [ Links ]
14. Souza RO, Lombardo GH, Pereira SM, Zamboni SC, Valera MC, Araujo MA, Ozcan M. Analysis of tooth enamel after excessive bleaching: a study using scanning electron microscopy and energy dispersive X-ray spectroscopy. Int J Prosthodont 2010; 23:29-32. [ Links ]
15. Ito Y, Momoi Y. Bleaching using 30% hydrogen and sodium hydrogen carbonate. Dent Mater J 2011; 30:193-198. [ Links ]
16. Xu B, Li Q, Wang Y. Effects of pH values of hydrogen peroxide bleaching agents on enamel surface properties. Oper Dent 2011; 36:554-562. [ Links ]
17. Horning D, Gomes GM, Bittencourt BF, Ruiz LM, Reis A, Gomes OM. Evaluation of human enamel permeality exposed to bleaching agents. Braz J Oral Sci 2013; 12: 114-118. URL: http://dx.doi.org/10.1590/S1677-32252013000200009 [ Links ]
18. Sa Y, Sun L, Wang Z, Ma X, Liang S, Xing W, Jiang T, Wang Y. Effects of two in-office bleaching agents with different pH on the structure of human enamel: an in situ and in vitro study. Oper Dent 2013; 38:100-110. [ Links ]
19. Borges AB, Yui KC D'Avila TC, Takahashi CL, Torres CR, Borges AL. Influence of remineralizing gels on bleached enamel microhardness in different time intervals. Oper Dent 2010; 35:180-186. [ Links ]
20. Arruda AM, Santos PH, Sundfeld RH, Berger SB, Briso AL. Effect of hydrogen peroxide at 35% on the morphology of enamel and interference in the de-remineralization process: an in situ study. Oper Dent 2012; 37:518-525. [ Links ]
21. Parreiras SO, Vianna P, Kossatz S, Loguercio AD, Reis A. Effects of light actived in-office bleaching on permeability, microhardness, and mineral content of enamel. Oper Dent 2014; 39: E225-30. doi: 10.2341/13-031. [ Links ]
22. Klaric E, Rakic M, Sever I, Milat O, Par M, Tarle Z. Enamel and dentin microhardness and chemical composition after experimental light-activated bleaching. Oper Dent 2015; 40: E132-141. doi: 10.2341/14-148. [ Links ]
23. Lia Mondelli RF, Garrido Gabriel TR, Piola Rizzante FA, Magalhaes AC, Soares Bombonatti JF, Ishikiriama SK. Do different bleaching protocols affect the enamel microhardness? Eur J Dent 2015; 9: 25-30. [ Links ]
24. Tahmassebi JF, Chrysafi N, Duggal MS. The effect of ozone on progression or regression of artificial caries-like enamel lesions in vitro. J Dent 2014; 42:167-174. [ Links ]
25. Lee BS, Huang SH, Chiang YC, Chien YS, Mou CY, Lin CP. Development of in vitro tooth staining model and usage of catalysts to elevate the effectiveness of tooth bleaching. Dent Mater 2008; 24:57-66. [ Links ]
26. Jaime IM, Franca FM, Basting RT, Turssi CP, Amaral FL. Efficacy of hydrogen-peroxide-based mouthwash in altering enamel color. Am J Dent 2014; 27:47-50. [ Links ]
27. Garcia EJ, Serrano AP, Urruchi WI, Deboni MC, Reis A, Grande RH, Loguercio AD. Influence of ozone gas and ozonated water application to dentin and bonded interfaces on resin-dentin bond strength. J Adhes Dent 2012; 14: 363-370. [ Links ]
28. Miranda Zarate AM, Bermejo GN, Bazan Ponce de Leon JE, Saravia Rojas MA. Efectos de un blanqueamiento dental con ozono y otro con peroxido de carbamida al 22% sobre La fuerza de adhesion al esmalte en diferentes intervalos de tempo. Acta Odontol Venez 2009; 47: 1-9. [ Links ]
29. Ruyter IE, Nilner K, Moller B. Color stability of dental composite resin materials for crown and bridge veneers. Dent Mater 1987; 3: 246-251. [ Links ]
30. Johnston WM. Color measurement in dentistry. J Dent 2009; 37: e2-6. [ Links ]
31. Knosel M, Reus M, Rosenberger A, Ziebolz D. A novel method for testing the veridicality of dental colour assessments. Eur J Orthod 2012; 34:19-24. [ Links ]
32. Gomes MN, Francci C, Medeiros IS, De Godoy Froes Salgado NR, Riehl H, Marasca JM, Muench A. Effect of light irradiation on tooth whitening: enamel microhardness and color change. J Esthet Restor Dent 2009; 21:387-394. [ Links ]
33. Soares DG, Basso FG, Pontes EC, Garcia Lda F, Hebling J, de Souza Costa CA. Effective tooth-bleaching protocols capable of reducing H2O2 diffusion through enamel and dentine. J Dent 2014; 42:351-358. [ Links ]
34. Abdelaziz R, Mosallam RS, Yousry MM. Tubular occlusion of simulated hypersensitive dentin by the combined use of ozone and desensitizing agents. Acta Odontol Scand 2011; 69:395-400. [ Links ]
35. Bahteja S. The miraculous healing therapy – "Ozone therapy" in dentistry. Indian J Dent. 2012; 3: 150-155. [ Links ]
36. Soares DG, Ribeiro APD, Vargas FS, Hebling J, Costa CAS. Efficacy and cytotoxicity of a bleaching gel after short application times on dental enamel. Clin Oral Investig 2013; 17:1901-1909. [ Links ]
37. Bocci V, Bianchi L, Larini A. The ozone enigma in medicine the biochemical relationship between ozone and body fluids may account for its biological, therapeutic and toxic effects. Riv Ital Ossigeno-Ozon 2003; 2:113-120. [ Links ]
38. Frysh H, Bowles WH, Baker F, Rivera-Hidalgo F, Guillen G. Effect of pH on hydrogen peroxide bleaching agents. J Esthet Dent 1995; 7:130-133. [ Links ]
39. Araujo F de O, Baratieri LN, Araujo E. In situ study of inoffice bleaching procedures using light sources on human enamel microhardness. Oper Dent 2010; 35:139-146. [ Links ]
40. Basting RT, Rodrigues AL Jr, Serra MC. The effect of 10% carbamide peroxide, carbopol and/or glycerin on enamel and dentin microhardness. Oper Dent 2005; 30: 608-616. [ Links ]
41. Anjum A, Otsuki M, Matin K, Tagami J. Preservation in the liquid media produces alterations in enamel surface properties. J Dent 2009; 37: 884-890. [ Links ]
42. Duggal MS, Nikolopoulou A, Tahmassebi JF. The additional effect of ozone in combination with adjunct remineralisation products on inhibition of demineralization of the dental hard tissues in situ. J Dent 2012; 40: 934-940. [ Links ]
43. Batista GR, Pagani C, Borges AB, Pucci CR, Torres CRG. Evaluation of dental bleaching gels´ pH in enamel contact. Int J Contemp Dent 2010; 1:1-5. http://edentj.com/ index.php/ijcd/article/view/32/12 [ Links ]
44. Abouassi T, Wolkewitz M, Hahn P. Effect of carbamide peroxide and hydrogen peroxide on enamel surface: an in vitro study. Clin Oral Investig 2011; 15:673-680. [ Links ]

