










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Odontológica Latinoamericana
versão On-line ISSN 1852-4834
Acta odontol. latinoam. vol.29 no.3 Buenos Aires dez. 2016
ARTÍCULOS ORIGINALES
Microbiological contamination in digital radiography: evaluation at the radiology clinic of an educational institution
Cristiana P. Malta1, Naiana N. L. Damasceno1, Rosangela A. Ribeiro1, Carolina S. F. Silva2, Karina L. Devito1
1 School of Dentistry, Federal University of Juiz de Fora, Brazil.
2 Biological Sciences Institute, Federal University of Juiz de Fora, Brazil.
CORRESPONDENCE Dr. Karina Lopes Devito Faculdade de Odontologia - Universidade Federal de Juiz de Fora Campus Universitario, s/n, CEP: 36036900, Juiz de Fora, Minas Gerais, Brazil karina.devito@ufjf.edu.br
ABSTRACT
The aim of this study was to evaluate the contamination rate of intraand extraoral digital Xray equipment in a dental radiology clinic at a public educational institution. Samples were collected on three different days, at two times in the day: in the morning, before attending patients, and at the end of the day, after appointment hours and before cleaning and disinfection procedures. Samples were collected from the periapical Xray machine (tube head, positioning device, control panel and activator button), the panoramic Xray machine (temporal support, bite block, control panel and activator button), the intraoral digital system (sensor), and the digital system computers (keyboard and mouse). The samples were seeded in different culture media, incubated, and colonyforming units (CFU/mL) counted. Biochemical tests were performed for suspected colonies of Staphylococcus, Streptococcus and Gramnegative bacilli (GNB). Fungi were visually differentiated into filamentous fungi and yeasts. The results indicated the growth of fungi and Staphylococcus from all sampling locations. GNB growth was observed from all sites sampled from the intraoral Xray equipment. On the panoramic unit, GNB growth was observed in samples from activator button, keyboard and mouse. In general, a higher number of CFU/mL was present before use. It can be concluded that more stringent protocols are needed to control infection and prevent Xray exams from acting as vehicle for cross contamination.
Key words: Radiology; Digital radiography; Infection control; Microorganisms; Bacteria; Fungi.
RESUMO
Contaminação microbiológica em radiografias digitais: avaliação da clínica de radiologia de uma instituição de ensino
O objetivo neste estudo foi avaliar o índice de contaminação dos equipamentos de radiografias digitais intra e extrabucais da clínica de radiologia odontológica de uma instituição pública de ensino. As amostras foram coletadas em três dias distintos, em dois momentos: pela manhã, antes dos atendimentos clínicos, e ao final do dia, após os atendimentos e antes dos procedimen tos de limpeza e desinfecção. As amostras foram coletadas do aparelho de raios X periapical (cabeçote, braço articular, painel de controle e botão disparador); do aparelho de raios X panorâmico (apoio temporal, bloco de mordida, painel de controle e botão disparador); do sistema digital intrabucal (sensor); dos computadores dos sistemas digitais (teclado emouse). As amostras foram semeadas em diferentes meios de cultura e, após incubação, foram contadas as unidades formadoras de colônia (UFC/mL). Testes bioquímicos foram realizados para colônias suspeitas de Staphylococcus, Streptococcus e bastonetes Gram negativos(BGN). Os fungos foram diferenciados visualmente em fungos filamentosos e leveduras. Os resultados indicaram crescimento de fungos e Staphylococcus em todos os locais amostrados. Em relação aos BGN, houve crescimento em todos os locais coletados do equipamento radiográfico intrabucal. No aparelho panorâmico, houve crescimento de BGN apenas no botão disparador, teclado e mouse. De maneira geral, houve maior número de UFC/mL antes do uso. Pode se concluir que é necessário implantar protocolos mais rigorosos de controle de infecção na prática radiológica, evitando que a obtenção de exames radiográficos seja um veículo para contaminação cruzada na FO/UFJF.
Palavras-chave: Radiologia; Radiografia Digital; Controle de Infecção; Microorganismos; Bactérias; Fungos.
INTRODUCTION
Radiographic exams area complementary tool for diagnosing major diseases of the oral cavity. Their increasing popularity has encouraged private colleges and clinics to adopt them1. The advantages of digital radiography include reduced radiation exposure, rapid image acquisition, easy digital storage, and electronic image transmission, as well as elimination of darkroom requirements and the possibility of image quality enhancement, such as changes in contrast and density2-4. In digital radiography, image receptors can be of two types: 1) solid electronic sensors such as chargecoupled devices (CCD) and complementary metal oxide semiconductor (CMOS) sensors, which produce images directly; and 2) photostimulable storage phosphor (PSP) plates that must be scanned to convert latent images into visible images3,5-8.
Digital radiography has many advantages over conventional techniques that use radiographic film as the image receiver. However, since the receptor is reused a number of times, as opposed to the single use of radiographic film, digital systems clearly increase problems associated with infection control1. The sensors or phosphor plates cannot be sterilized; thus, it is important to use effective physical barriers to protect them7,9-11. At dental schools, the sensors are handled by a large number of operators and used ona great many patients, further challenging the effectiveness of infection control3. In addition to the sensors, care should be taken with the other equipment involved with digital systems, such as the computer, particularly the keyboard and the mouse, and the actual Xray machine, whether intraoral or extraoral.
Given the need to evaluate the infection control protocol followed at the Radiology Clinic (School of Dentistry), the aim of this study was to evaluate microbial contamination on the surfaces of the intraoral and extraoral digital radiology equipment used at the Radiology Clinic to identify the different groups of microorganisms present on them, and to compare contamination rates before and after clinic office hours.
MATERIALS AND METHODS
Samples were collected at the Radiology Clinic over three nonconsecutive random days at two different times: in the morning, before attending patients, and at the end of the day, after appointment hours and before cleaning and disinfection procedures. Samples were collected from the following surfaces of the radiological equipment and accessories: 1) digital intraoral system: periapical Xray machine (tube head, positioning device, control panel and activator button), digital system (sensor), and computer (mouse and keyboard); 2) digital extraoral system: panoramic Xray machine (temporal support, bite block, control panel and activator button) and computer (mouse and keyboard). Material was collected using a sterile swab soaked in a test tube containing 10 mL sterile saline solution (0.85% NaCl). After using the swab, it was stored in the same tube until samples were processed. Sterilized 5x5 cm2 templates were used to standardize the sampling area. The total area sampled per device was 125 cm2. For the activator button, sensor and bite block, where the surface is extremely small, the entire area was used for collection. Throughout the collection process, personal protective equipment was used to avoid cross contamination.
The collected samples were subjected to serial dilution in which 1 mL aliquots were transferred to tubes containing 9 mL sterile saline solution (0.85% NaCl), and so on, until 102 dilution. After homogenization, 100 μL aliquots were dispensed using a pipette and seeded with a Drigalski loop on the surfaces of plates, in duplicate. The following culture media were used: mannitol agar (HiMedia, Mumbai, India), which is selective for the isolation of staphylococci; MacConkey agar (HiMedia, Mumbai, India), which is selective for the isolation of enterobacteria and other Gramnegative nonfermenting bacilli; Sabouraud dextrose agar (HiMedia, Mumbai, India), which is used for the isolation of molds and yeasts; and sheep blood agar (HiMedia, Mumbai, India), which is used for the recovery of streptococci/enterococci, staphylococci and Gramnegative bacilli. The seeded plates with mannitol agar and MacConkey agar culture media were incubated at 35 ± 2°C in a bacteriological incubator for 24 to 48 hours. The plates containing the blood agar medium were subjected to microaerophilic conditions with a candle in an augmented atmosphere of 5% CO2 at 35 ± 2°C for 24 to 72 hours. The Sabouraud agar plates were incubated at 27 ± 2°C for up to seven days. After the incubation period, the colonies were counted. The dilution formula was applied to calculate colonyforming units per milliliter (CFU/mL) of each sampling site and averaged, considering the duplication.
Colonies suggestive of staphylococci that were identified in mannitol agar and blood agar were subcultured in tryptone soya agar (TSA; HiMedia, Mumbai, India) to remove selective agent interfe rence for Gram stain test confirmation and for biochemical analyses. In the Gram stain test, the observation of grouped Grampositive cocci is confirmatory of the group. The catalase test was used to differentiate staphylococci from streptococci/ enterococci because staphylococci behave as catalasepositive bacteria. The coagulase and DNase tests served to differentiate Staphylococcus aureus from other species. At all stages, reference cultures were used as positive controls (Staphylococcus aureusATCC 33591 and Staphylococcus epidermidis ATCC 12228). Novobiocin antimicrobial suscepti bility testing was used to differentiate between Staphylococcus epidermidis and Staphylococcus saprophyticus; the positive control for sensitivity in this test was the presence of a halo equal to or greater than 15 mm. To avoid overestimating the results, the count of staphylococcal colonies on blood agar was disregarded for the locations that presented growth in both mannitol agar and blood agar in the same collection.
Colonies suggestive of streptococci/enterococci in the blood agar medium were subcultured in TSA for confirmation by the Gram stain test, in which Grampositive cocci are observed in long chains, while for colonies suggestive of enterococci, Grampositive cocci are observed in short chains or in pairs. To differentiate staphylococci from streptococci/ enterococci, the colonies subcultured in TSA were subjected to the catalase test, where catalasenegative colonies were selected. These colonies were further subcultured in blood agar and incubated under microaerophilic conditions for 24 hours to observe the hemolysis pattern. Colonies suggestive of Gramnegative bacilli (GNB) in MacConkey agar and blood agar were subcultured in TSA and submitted to the Gram stain test. To differentiate between glucosefermenting and nonfermenting bacilli, the fermentation test was conducted in a glucose broth. Oxidase test strips were used to differentiate between oxidasepositive and oxidasenegative colonies. Tests were also run using the Bactray system (Laborclin, Pinhais, Parana, Brazil) for the biochemical identification of GNB via pH changes, substrate hydrolysis, and metabolic production. To avoid overestimating the results, the count of GNB colonies in blood agar was disregarded for the locations that presented growth in both MacConkey agar and blood agar in the same collection. Fungi growing in Sabouraud agar were visually differentiated into filamentous fungi and yeasts. No biochemical test was performed.
The KolmogorovSmirnov test was used to verify that the values were normally distributed. The Wilcoxon test allowed a comparison of the CFU counts before and after the clinic's activities. We used SPSS version 13.0 (SPSS Inc, Chicago, USA). The significance level was 5% (p≤0.05).
RESULTS
Altogether, 78 samples were collected from the Radiology Clinic, with half the samples (three per site) collected before the clinical procedures and the other half (three per site) collected after clinic office hours and before cleaning and disinfection procedures.
Tables 1 and 2 present the data describing the quantitative distribution of the different microorga nisms from the collection sites for intraoral and extraoral digital systems, respectively. Fungi were present at all collection sites, both before and after clinic office hours. Staphylococci were also highly prevalent, being absent only in a few specific collection periods. In contrast, GNB were found less frequently, although they were present at all the collection sites before the use of the intraoral equipment.
Table 1: Descriptive data (mean, median, minimum, and maximum) of the quantitative distribution of the various microorganisms in the respective collection locations in the intraoral digital system.
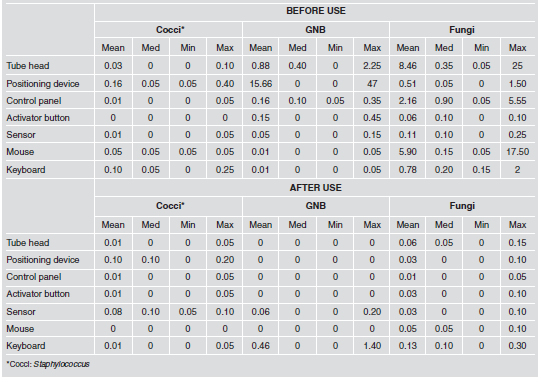
Table 2: Descriptive data (mean, median, minimum, and maximum) of the quantitative distribution of the various microorganisms in the respective collection locations in the extraoral digital system.

In assessing the growth of Staphylococcus/ Streptococcus in the intraoral digital Xray system, all the colonies tested positive for catalase, i.e., no growth of Streptococcus/ enterobacteria was observed. After coagulase and DNase testing, Staphylococcus aureus was not isolated. Regarding the novobiocin susceptibility profile, 23.81% were resistant and were identified as Staphylococcus saprophyticus, whereas 76.19% were sensitive and characterized as Staphylococcus epidermidis. In the extraoral digital Xray system, only one sample, which was collected after the use of the control panel, had a negative result for catalase and was visible as Grampositive cocci in long chains, which are representative of Streptococcus. This colony was subcultured in blood agar and incubated under microaerophilic conditions for 24 hours, at which point a partial hemolysis pattern was observed that was alphahemolytic. The rest of the colonies, which were catalasepositive bacteria, were subjected to coagulase and DNase testing. Only one colony, which was obtained from the activator button before use, showed positive results for both tests and was identified as S. aureus. Regarding the novobiocin susceptibility profile, 31.34% were resistant and identified as S. saprophyticus, whereas 64.93% were sensitive and characterized as S. epidermidis (Fig. 1).

Fig. 1: Isolation percentage of the different microorganisms detected.
In the evaluation of GNB growth on the intraoral digital Xray system, all samples were negative for the glucose fermentation test. Approximately 30% of the samples were oxidasepositive GNB, and 70% were oxidasenegative GNB. Tests were conducted using the Bactray system, which identified Proteus mirabilis on the positioning device, control panel, tube head and keyboard before use and on the sensor and keyboard after use in 52.94% of the samples, with a 100% probability. Pseudomonas pseudoalcaligenes was identified on the tube head, positioning device, control panel, button and mouse before use in 29.41% of the samples, with a probability of 83.18%. Acinetobacterbaumannii/ calcoaceticus was identified on the sensor, positioning device and tube head before use in 17.65% of the samples, with a probability of 65.5%. Regarding the glucose fermentation test for the colonies identified on the extraoral digital Xray system, 23.08% of the samples were fermentationpositive bacteria, and 76.92% were fermentationnegative bacteria. Only one oxidasepositive sample was identified. The Bactray system identified Acinetobacter baumannii/ calcoaceticus on the keyboard before use and on the keyboard and activator button after use in 53.85% of the samples, with a probability of 65.5%. Serratiaplymuthica was identified on the keyboard and mouse before use in 23.08% of the samples, with a probability of 62.84%. Klebsiellarhinoscleromatis was identified on the keyboard after use in 15.38% of the samples, with a probability of 30%. Burkholderiapseudomallei was identified on the keyboard after use in 7.69% of the samples, with a probability of 48.78% (Fig. 1). In the evaluation of fungal growth fromthe intraoral digital Xray system, 3.64% filamentous fungi and 96.36% yeasts were distinguished visually. For the extraoral system, 68.74% filamentous fungi and 31.26% yeasts were distinguished (Fig. 1).
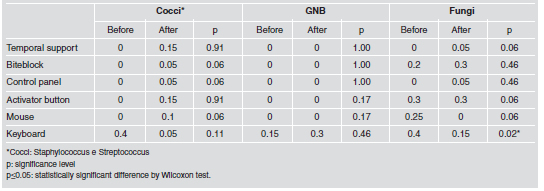
The results of the comparisons between CFU/mL counts before and after the clinical procedures are shown in Tables 3 and 4. For the intraoral digital system, the Wilcoxon test indicated significant differences only for the fungi collected from the tube head, control panel, mouse and keyboard. For the extraoral digital system, the CFU/mL counts before and after clinical procedures showed a significant difference only for the fungi collected from the keyboard. Notably, the number of colonies was always higher before clinical procedures.
Table 3: Comparison of CFU/mL counts (median) before and after the clinical procedures, for the intraoral digital X-ray system.

Table 4: Comparison of CFU/mL counts (median) before and after the clinical procedures, for the extraoral digital X-ray system.
DISCUSSION
Digital Xray is a major advance in radiogra phic imaging and is increasingly being adopted by dental professionals. It is already used even in undergraduate courses in dentistry and has great potential to aid diagnosis and treatment procedures and to facilitate image storage, transfer and retrieval4,6,8,12. However, the substitution of films by sensors or phosphor plates does not free the digital equipment from crosscontamination; on the contrary, the reuse of the image receptors increases the importance of infection control. Bacterial, viral, and fungal infections pose a significant hazard in dental practice, and biosafety principles must be followed to prevent contamination of equipment, operators and patients. Dental radiography, which is normally overlooked because it is not routinely associated with needles, sharp instruments and waste blood, has recently become a concern because infectious diseases may be transmitted by contamination of the materials and equipment used to obtain intraoral and extraoral radiographs. The protocols suggested as universal precautions for infection control emphasize the use of barriers or the chemical disinfection of surfaces. However, the barriers used for radiographic equipment should allow visual access to the control panel and should not interfere with the configuration of the machine. Moreover, disinfecting surfaces with chemicals is not common practice with electronic equipment13. Digital Xray sensors, which cannot be sterilized by heat, should be covered with protective barriers2,14 However, some studies have shown that receptors for digital images are potential sources of contamination even when surrounded by a plastic barrier10,11,15,16.
In dental schools, problems with infection control are more critical because of the large number of patients and radiographic equipment operators involved. In addition, the inexperience of most operators (undergraduate students) can further complicate the installation of strict infection control protocols. Some authors have suggested gas sterilization with ethylene oxide for digital sensors at dental schools3. Additionally, for installations that do not have access to gas sterilization systems, a disinfectant with adequate cleaning effectiveness and short contact time, such as propanolethanol or a chlorinebased disinfectant3 can be considered. Although the literature describes the actions that should be taken to control infection before, during and after radiographic film exposure and emphasizes that aseptic practices applied in dental radiography are relatively simple and inexpensive, a great amount of negligence by operators still occurs17,18. Qudeimat et al reported that changing gloves between patients was rare among dentists and dental assistants in a teaching center in Jordan19. McCarthy and MacDonald, who compared infection control practices among general dentists and specialist groups, indicated that better compliance with infection control practices is needed in both groups20. These situations indicate that crossinfection control issues do not arouse interest among dental surgeons or that there is a deficiency in continuing education regarding how to avoid crossinfection in dental practice. Biosafety in radiology should be more clearly required by the authoritative bodies, not only for students in dental programs but also for professionals in public and private practices21. Many microorganisms are related to dental practice. Even though some of them belong the normal microbiota, they should be considered opportunistic pathogens which can cause human infections constituting a disease when introduced into unprotected sites or in situations of immune system deficiency, depending on their virulence factors. The upper respiratory tract and oral cavity are colonized by numerous microorganisms such as Staphylococcus, Streptococcus, Porphyromonas, Prevotella, Haemophilus, Eubacterium, Enterobacteriaceae, Actinomyces, Acinetobacter and Candida22,23.
The genus Staphylococcus is composed of diverse species that can be found in human clinical samples. These microorganisms are important pathogens and, in general, involved in various diseases mediated by toxins, such as skin diseases, bacte remia, endocarditis, pneumonia, osteomyelitis, septic arthritis, urinary tract infections and opportunistic infections. The species most commonly associated with human diseases are Staphylococcus aureus - the most virulent and bestknown member of the genus- and Staphylococcus epidermidis, Staphylococcus haemolyticus, Staphylococcus lugdunensis and Staphylococcus saprophyticus22. The results of the present study indicated growth of Staphylococcus from all sampling sites, and Staphylococcus aureus, Staphylococcus saprophyticus and Staphylococcus epidermidis were also identified. The rate of contamination with Staphylococcus is of concern because, although these bacteria are members of the normal microbiota of the skin and mucous membranes of humans, they also cause suppuration, abscess formation, various pyogenic infections, and even fatal septicemia22.
Streptococci and enterococci are Grampositive, catalasenegative, and oxidasenegative bacteria that usually grow into pairs and in chains. Among the important streptococci is Streptococcus pyogenes, which is responsible for suppurative afflictions such as pharyngitis, soft tissue infections, and streptococcal toxic shock syndrome and for nonsuppurative disorders such as rheumatic fever and glomerulonephritis. Streptococcus agalactiae is responsible for diseases in newborns and infections in pregnant women. Several βhemolytic streptococci are important. Streptococcus viridans is responsible for abscess formation in deep tissue; Streptococcus anginus, for septicemia in neutropenic patients; Streptococcus mitis and Streptococcus salivarius, for subacute endocarditis; Streptococcus mutans, for tooth decay; Streptococcus bovis, for cancer of the gastrointestinal tract; Streptococcus pneumoniae, for pneumonia, meningitis, and bacteremia22.
According to Jorge23, only four groups are considered oral streptococci, i.e., the mutans, anginosus, mitis, and salivarius groups. In this study, streptococcal contamination of the extraoral Xray device control panel proved the existence of oral cavity microorganisms on the radiographic equipment; these microorganisms are often present in oral mucosa and in saliva22. The bacilli or Gramnegative rods belonging to the Enterobacteriaceae family are widely distributed in nature; found in soil, water, vegetables, and the intestinal tracts of humans and animals24. They cause a variety of diseases in humans, including 30% to 35% of all bacteremia, over 70% of urinary tract infections, and a large number of intestinal infections. The Salmonella serotype Typhi, and Shigella and Yersinia pestis species are always associated with human disease, while other species such as Escherichia coli, Klebsiellapneumoniae, and Proteus mirabilis are commensal members of the normal microbiota that can cause opportunistic infections22. Escherichia coli, Klebsiellasppand Yersinia have been detected in the human oral cavity and subgingival samples23. Gramnegative nonfermenting bacilli are a nonsporeforming aerobic group that do not use carbohydrates as an energy source or degrade them by fermentative pathways, and have special requirements for growth24. They constitute a group of opportunistic pathogens of plants, animals and human beings, and their taxonomic classification has undergone changes in recent years. However, most of the clinically significant isolates are members of five genera: Pseudomonas, Burkholderia, Stenotrophomonas, Actinobacter and Moraxella22. In the present study, GNB growth was observed from all locations sampled from the intraoral radiographic equipment. On the panoramic unit, GNB growth was observed only from the activator button, keyboard and mouse. The following species were identified: Proteus mirabilis, Pseudomonas pseudoalcaligenes, Acinetobacterbaumannii/ calcoaceticus, Serratiaplymuthica, Klebsiellarhinoscleromatis and Burkholderiapseudomallei. Approximately 80,000 identified species of fungi exist; however, less than 400 are medically important, and fewer than 50 species cause approximately 90% of fungal infections. Most pathogenic fungi are exogenous, and their natural habitats are water, soil and organic waste. Candidiasis and dermatophytosis are the fungal infections (mycoses) of highest incidence, caused by fungi of the resident microbiota which are highly adapted to survival in the human host25. In the present study, although fungi were the most prevalent microorganisms, with growth in all samples and from all sampling sites, they were only identified visually as filamentous fungi or yeasts.
Although no study in the literature has determined the maximum amount of microorganisms allowed in a clinical dental setting, the goal is to reduce this amount as much as possible to promote health and prevent disease. Importantly, we can never be certain whether we are dealing with an immunocompromised patient during a radiographic examination. For these patients, a low number of microorganisms can cause disease, or normal microbiota can cause opportunistic infections. The results of this study also showed a higher CFU/mL count before the use of the radiographic equipment, possibly due to the timing of the sampling, because the swabbing actions during collection before the use of the equipment may have cleaned the collection sites. A second hypothesis is that the equipment and surfaces are poorly sanitized. Because potentially infectious individuals are not always identified through information from their medical history or through physical, clinical, and laboratory exams, protective measures should be adopted to prevent or reduce the transmission of pathogenic microorganisms that can cause various types of infectious or contagious diseases. Thus, the dentist is primarily responsible for crossinfection control in the clinical workplace, and must maintain asepsis while conducting Xray exams and verify that the necessary measures for safe and effective infection control are being followed by all team members. Methods for sterilization, disinfection, mechanical barriers and personal protective equipment should be used in all dental specialty work, including radiology, to ensure a favorable environment for maintaining the health of staff and patients26.
Based on the results of this study, acquisition of intraoral and extraoral digital radiographs increases the possibility of crossinfection, creating the need for more stringent protocols for infection control in radiological practice, in order to prevent Xray exams from being vehicles for cross contamination, particularly at educational institutions.
1. Kalathingal S, Youngpeter A, Minton J, Shrout M, Dickinson D, Plummer K, Looney S. An evaluation of microbiologic contamination on a phosphor plate system: is weekly gas sterilization enough? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 109: 457-462. [ Links ]
2. American Dental Association Council on Scientific Affairs: The use of dental radiographs: update and recommendations. J Am Dent Assoc 2006; 137: 1304-1312. [ Links ]
3. Kalathingal SM, Moore S, Kwon S, Schuster GS, Shrout MK, Plummer K.An evaluation of microbiologic contamination on phosphor plates in a dental school. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 107: 279-282. [ Links ]
4. Christensen GJ.Is the current generation of technology facilitating better dentistry? J Am Dent Assoc 2011; 142: 959-963. [ Links ]
5. ADA Council on Scientific Affairs. An update on radiographic practices: information and recommendations. ADA Councilon Scientific Affairs. J Am Dent Assoc 2001; 132: 234-238. [ Links ]
6. MacDonald R. Digital imaging for dentists. Aust Dent J 2001; 46: 301-305. [ Links ]
7. Parks ET, Williamson GF. Digital radiography: an overview. J Contemp Dent Pract 2002; 3: 23-39. [ Links ]
8. Van Der Stelt PF. Filmless imaging: the uses of digital radiography in dental practice. J Am Dent Assoc 2005; 136: 1379-1387. [ Links ]
9. Wenzel A, Frandsen E, Hintze H.Patient discomfort and cross infection control in bitewing examination with a storage phosphor plate and a CCDbased sensor. J Dent 1999; 27: 243-246. [ Links ]
10. Hokett SD, Honey JR, Ruiz F, Baisden MK, Hoen MM. Assessing the effectiveness of direct digital: radiography barrier sheaths and finger cots. J Am Dent Assoc 2000; 131: 463-467. [ Links ]
11. MacDonald DS, Waterfield JD. Infection control in digital intraoral radiography: evaluation of microbiological contamination of photostimulable phosphor plates in barrier envelopes. J Can Dent Assoc 2011; 77: b93. [ Links ]
12. Farman AG, Levato CM, Gane D, Scarfe WC. In practice: how going digital will affect the dental office. J Am Dent Assoc 2008; 139: 14S-19S. [ Links ]
13. Wyche CJ. Infection control protocols for exposing and processing radiographs. J Dent Hyg 1996; 70: 122-126. [ Links ]
14. Negron W, Mauriello SM, Peterson CA, Arnold R. Crosscontamination of the PSP sensor on a preclinical setting. J Dent Hyg 2005; 79: 8. [ Links ]
15. Hubar JS, Oeschger MP. Optimizing efficiency of radiograph disinfection. Gen Dent 1995; 43: 360-362. [ Links ]
16. Kuperstein AS.Defective plastic infectioncontrol barriers and faulty technique may cause PSP plate contamination used in digital intraoral radiography. J Evid Base Dent Pract 2012; 12: 46-47. [ Links ]
17. Bartoloni JA, Charlton DG, Flint DJ. Infections control practices in dental radiology. Gen Dent 2003; 51: 264-271. [ Links ]
18. Palenik CJ. Infection control practices for dental radiography. Dent Today 2004; 23: 52-55. [ Links ]
19. Qudeimat MA, Farrah RY, Owais AI. Infection control knowledge and practices among dentists and dental nurses at a Jordanian university teaching center. Am J Infect Control 2006; 34: 218-222. [ Links ]
20. McCarthy GM, MacDonald JK.A comparison of infection control practices of different groups of oral specialists and general dental practitioners. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 47-54. [ Links ]
21. Yuzbasioglu E, Sarac D, Canbaz S, Sarac S, Gengiz S.A survey of crossinfection control procedures: knowledge and attitudes of Turkish dentists. J Appl Oral Sci 2009; 17: 565-569. [ Links ]
22. Murray PR, Rosenthal KS, Pfaller MA: Microbiologia Medica. Rio de Janeiro, RJ, Brasil: Elsevier, 2009. [ Links ]
23. Jorge AOC:Microbiologia e Imunologia Oral. Rio de Janeiro, RJ, Brasil: Elsevier, 2012. [ Links ]
24. Win-Koneman EW, Winn Jr W, Allen S, Janda W, Procop G, Schreckenberger P, Woods G:Diagnostico Microbiologico: Texto e Atlas Colorido. Rio de Janeiro, RJ, Brasil: Guanabara Koogan, 2008. [ Links ]
25. Brooks GF, Carroll KC, Butel JS, Morse AS, Mietzner TA:Microbiologia Medica de Jawetz, Melnick e Adelberg. Porto Alegre, RS, Brasil: AMGH, 2012. [ Links ]
26. Silva MAS, Martins MV, Medici Filho E, Moraes LC, Castilho JCM, Jorge AOC. Evaluation of the efficiency of an infection control protocol in dental radiology by means of microbiological analysis. Cienc Odontol Bras 2004; 7:15-21. [ Links ]

