










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.32 no.1 Buenos Aires abr. 2019
ORIGINAL ARTICLE
Evaluation of 3Mix-MP and pulpectomies in non-vital primary molars
Evaluación de 3Mix-MP y pulpectomías en molares primarios no vitales
Giselle A. Zacharczuk1, Marina A. Toscano1, Graciela E. López1, Andrea M. Ortolani1
1 Universidad de Buenos Aires. Facultad de Odontología. Cátedra de Odontología Integral Niños. Buenos Aires, Argentina.
Received: December 2018; Accepted: March 2019.
ABSTRACT
Pulpectomies in primary molars are often hindered by several factors, including anatomical and physiological characteristics of posterior primary teeth and young patients' lack of cooperation with laborious treatments. This study was undertaken in search of easier but equally effective therapies that could eliminate infection, preserve the teeth and avoid extractions. The aim of the study was to estimate and compare clinical and radiographic success between pulp treatment with 3Mix-MP and pulpectomy with Maisto-Capurro paste in primary necrotic molars. A longitudinal prospective study was conducted at the Department of Comprehensive Pediatric Dentistry of the Faculty of Dentistry of the University of Buenos Aires (20152017). The study included 46 primary molars with necrotic pulp of children without immune or metabolic compromise. Children and their legal guardians provided assent and informed consent. Selected molars were randomly divided into 2 groups: G1: Pulpectomy treatment with Maisto-Capurro paste; and G2: Treatment with 3Mix-MP paste. Treatments were evaluated at 1, 3, 6,12 and 18 months (intra and inter-rater agreement 0.92 and 0.84). Clinical success was considered to be the absence of any of the following: pain, sensitivity to percussion or palpation, swelling, fistula and non-physiological mobility, while radiographic success was considered to be: absence of internal or external non-physiological resorption, no progression or reduction of radiolucent periapical/interradicular lesion and evidence of bone regeneration. Percentages, 95% C.I., and CHI2 were calculated for the comparison between groups. Overall clinical success was 91.5% and 87.5% (p=0.48) and overall radiographic success was 88.3% and 82.3% (p=0.31) for G1 and G2 respectively. No significant clinical or radiographic difference was found between groups. Both treatments showed similar clinical and radiographic behavior during the study periods.
Keywords: 3Mix ointment, pulpectomy, primary dentition, dental pulp, endodontics.
RESUMEN
Las pulpectomías en molares primarios se ven dificultadas frecuentemente por las características anatómicas y fisiológicas de éstos y por la escasa colaboración que brindan los pacientes de corta edad ante tratamientos tan laboriosos. En búsqueda de terapéuticas más sencillas, pero igualmente eficaces, que consigan eliminar la infección para conservar las piezas y evitar las exodoncias, se ha planteado como objetivo de este estudio: estimar y comparar la proporción de éxito clínico y radiográfico entre el tratamiento pulpar con 3Mix-MP y la pulpectomía con pasta de Maisto-Capurro en molares primarios con necrosis. Se realizó un estudio longitudinal y prospectivo en la Cátedra de Odontología Integral Niños de la Facultad de Odontología de la Universidad de Buenos Aires (2015 - 2017). Formaron parte del estudio 46 molares primarios con diagnóstico de necrosis pulpar, de niños sin compromiso inmunológico ni metabólico y que junto con sus responsables legales brindaron el asentimiento y el consentimiento informado. Los molares seleccionados fueron divididos aleatoriamente en 2 grupos: G1: Tratamiento de pulpectomía con pasta de Maisto-Capurro y G2: Tratamiento con pasta 3Mix-MP. Los tratamientos fueron evaluados al mes, 3, 6, 12y 18 meses (concordancia intra-examinador 0,92 e interexaminador 0,84), considerando como éxito clínico la ausencia de dolor, sensibilidad a la percusión y palpación, edema, fístula y movilidad no fisiológica; y como éxito radiográfico, ausencia de reabsorción interna o externa no fisiológica, no progresión o reducción de la lesión radiolúcida interradicular/periapical y evidencia de regeneración ósea. Se calcularon porcentajes, I.C 95% y CHI2para la comparación. El éxito clínico global fue de 91,5%y 87,5% (p=0.48) y el éxito radiográfico global de 88,3% y 82,3% (p=0.31)para G1 y G2 respectivamente, sin diferencias significativas entre ambos grupos. En los periodos estudiados ambos tratamientos mostraron comportamientos clínico y radiográfico semejantes.
Palabras clave: Pasta 3Mix, pulpectomías, dentición primaria, pulpa dental, endodoncia.
INTRODUCTION
Premature loss of primary molars can cause a series of consequences such as reduction of the space required for eruption of replacement teeth, mesialization of permanent first molars, problems with mastication and lingual interposition, among others. The use of space maintainers is not always effective, especially when primary second molars are lost prior to the eruption of permanent first molars.
In pediatric dentistry, non-vital primary teeth often receive endodontic treatment with the aim of preserving those teeth in adequate anatomical-functional condition until the time of their normal exfoliation.
Pulpectomy is the endodontic therapy of choice. During this treatment, necrotic pulp tissue is removed, root canals are shaped and disinfected and an intracanal resorbable medication is placed1. In Argentina, Maisto-Capurro paste is the most frequently used endodontic material for filling root canals in primary teeth. It is an alkaline paste composed of calcium hydroxide and iodoform and is characterized by having the following properties: antimicrobial potential, biocompatibility, radiopacity and rapid resorption2. Several factors make pulpectomy treatment difficult to perform: the complex internal anatomy of root canals in primary molars,3 which prevents their adequate mechanical/ chemical preparation, physiological root resorption processes that modify the shape, position and size of the endodontic apex and factors related to cooperation and behavior in young children.
Less complex techniques are therefore needed, which would simplify operative steps, require less cooperation from the patient, and at the same time ensure proper disinfection of the root canal system. LSTR (Lesion Sterilization and Tissue Repair) therapy, developed at the University of Niigata, Japan, is proposed as a treatment option for primary molars with pulp necrosis. LSTR is based on the concept that repair is possible if lesions are adequately disinfected4. It uses the NIET (NonInstrumental Endodontic Treatment) technique and a paste with proven antimicrobial efficacy: 3Mix-MP, which is a triple antibiotic paste (3Mix) containing metronidazole, ciprofloxacin and minocycline powder in macrogol and propylene glycol (MP) antibiotic carriers5.
The ability of 3Mix-MP to disinfect carious lesions and infected root dentin lesions has been demonstrated in vitro, 5-7 including its efficacy against E. Coli 6 and Enterococcus faecalis and faecium8. Studies have also been performed on animals9 and it has been proven that propylene glycol as a triple antibiotic paste carrier enables adequate penetration through dentin10 and that its biocompatibility is similar to that of calcium hydroxide11.
The aim of the current study was to estimate and compare clinical and radiographic success between pulp treatment with 3Mix-MP and pulpectomy with Maisto-Capurro paste in non-vital primary molars.
MATERIALS AND METHODS
This experimental, prospective, longitudinal study was conducted at the Department of Comprehensive Pediatric Dentistry at the Buenos Aires University School of Dentistry during 2015 - 2017, with approval from its Ethics in Research Committee (N° 0018/2015).
Sample selection and group formation
Teeth were selected through anamnesis and clinical-radiographic examination according to the inclusion and exclusion criteria specified below.
Inclusion criteria: primary molars diagnosed with pulp necrosis in patients of both sexes who visited for comprehensive dental care, and who signed assent and informed consent together with their legal guardians.
Exclusion criteria:
• Molars with more than 1/3 root resorption.
• Presence of periapical or interradicular radiolucent areas which could compromise the permanent tooth bud.
• Internal resorption.
• Perforation of the pulp chamber floor.
• Teeth with extensive crown destruction which would not allow subsequent restoration.
• Immunologically and/or metabolically compromised patients.
Selected molars were randomly assigned to 2 groups: G1 (control), treated with pulpectomy and Maisto-Capurro paste; G2 (experimental) treated with LSTR 3Mix-MP
Tooth of patients who attended on even days were assigned to G1, and those who attended on odd days to G2. If the same patient had more than one molar appropriate for the study, such molars were assigned to different groups.
Professional team and evaluation criteria
Four professionals were trained and calibrated in the examination methods, materials and sequence of technical procedures (intra-rater agreement 0.92 and inter-rater agreement 0.84). They selected the teeth for the study, performed the procedures according to the protocol described in Table 1 and evaluated evolution clinically and radiographically at 1, 3, 6, 12 and 18 months.
Table 1: Procedural protocol.

Clinical success was considered to be the absence of any of the following: pain or sensitivity to percussion and palpation, swelling, fistula and nonphysiological mobility, while radiographic success was considered to be: absence of internal or external non-physiological resorption, no progression or reduction of radiolucent periapical/interradicular lesion and evidence of bone regeneration.
Endodontic pastes preparation
1. Maisto-Capurro paste: equal parts by volume of calcium hydroxide and iodoform, with propylene glycol as carrier.
2. 3Mix-MP paste: the three antibiotics in this paste were purchased in their pure powdered form. For the preparation of the mixture they were proportioned in equal parts by volume (metronidazole: ciprofloxacin: minocycline=1:1:1). Carriers (macrogol and propylene glycol) were also used in a ratio 1:1 by volume. The antibiotic powder mixture was added to the carriers until a consistent, non-friable paste was obtained12.
Both pastes were prepared at the time of use.
Statistical analysis
The records for the different variables were entered into a Microsoft Excel database and analyzed statistically with SPSS software (Statistical Packages for the Social Sciences 20.0; IBM, Armonk, NY, USA). Percentages were calculated with their respective 95% confidence intervals and Chi-square test with a significance level of 0.05 was used to compare evolution between groups.
RESULTS
Each group consisted of 23 primary molars in children whose mean age was 6.15 ± 1.38 and 6.3 ± 1.49 for G1 and G2, respectively.
Comparison between groups of clinical and radiographic characteristics of molars in baseline conditions showed no significant difference (p= 0.66) (Fig.1).

Fig. 1: Analysis of baseline clinical and radiographic characteristics for both groups. Preoperative characteristic percentages for each group (G1 and G2). No statistically significant difference was found between groups (p=0.66).
Table 2 shows the clinical and radiographic outcomes for the times evaluated. The success rates of both G1 and G2 declined over time.
Table 2: Clinical and radiographic results for the evaluated periods.
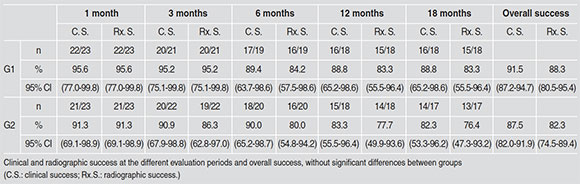
At 18 months (as the result of patients noncompliance with follow-up appointments) 18 molars (78.2%) were checked in G1 and 17 molars (73.9%) in G2. Clinical success at 18 months was 16/18 (88.8%) in G1 and 14/17 (82.3%) in G2, and radiographic success at 18 months was 15/ 18 (83.3%) and 13/17 (76.4%) in G1 and G2 respectively.
Overall clinical success was 91.5% and 87.5% (p= 0.48) and overall radiographic success was 88.3% and 82.3% (p= 0.31) for G1 and G2 respectively, with no significant difference between groups.
DISCUSSION
The management of primary molars diagnosed with necrosis is a controversial issue in pediatric dentistry. Endodontic therapy is a reasonable conservative option to ensure normal tooth exfoliation or longterm survival of the primary tooth in cases of agenesis. It also reduces the need for extraction, which, in addition to being a traumatic experience for a young child, requires the use of prosthetic resources to maintain spaces, involving higher costs and commitment to periodical follow-up.
The AAPD1 (American Academy of Pediatric Dentistry) considers pulpectomy to be the endodontic treatment of choice for necrotic primary molars. The review of the literature on this treatment showed variable success rates, depending on the materials employed for filling the canals. The most frequently used are zinc oxide eugenol (ZOE), iodoform pastes (KRI®) and pastes with calcium hydroxide and iodoform (Vitapex®, Metapex®), among others. Vitapex® has been widely studied and the literature reports clinical success rates of 100%13-16 and radiographic success rates at 12 months of 90 to 100%13,15-17. We used Maisto-Capurro paste in this study because it is very similar to Vitapex® in composition and characteristics. However, our overall clinical and radiographic results (91.5% and 88.3%, respectively) were slightly lower than those mentioned above for treatments with Vitapex®. We assume that this difference may be owed to the fact that Vitapex® is an industrial paste, ready to be used and presented in a syringe application system which facilitates manipulation, whereas in the present study Maisto-Capurro paste was prepared at the time of use, the ingredients were dispensed by the operators, and it was applied within the canals using endodontic files (Fig. 2).

Fig. 2: Successful pulpectomy in a lower left first molar. A: Initial image: carious lesion involving pulp and interradicular radiolucency. B: Determination of working length. C: Immediately postoperative image. D: Xray. 12 months postoperative.
As mentioned, due to the complexity of the technique and the topographic characteristics of primary molars, pulpectomy is not always suitable to all children or all professionals. LSTR 3Mix-MP therapy is proposed as an alternative, especially for uncooperative children and low-resource areas. The procedure is simple, not time-consuming, and demands only one visit. It requires no mechanical instrumentation because the antimicrobial capacity of 3Mix-MP paste sterilizes the area, promoting lesion repair and preserving the primary tooth until normal exfoliation time4 (Figs. 3 and 4).

Fig. 3: Successful LSTR 3MixMP in a lower right second molar with carious lesion involving pulp and interradicular radiolucency. A: Initial image. B: Xray. 6 months postoperative: shows nonprogression of furcation lesion. C: Xray. 12 months postoperative: reduction in interradicular radiolucency area and presence of new bone formation. D: Xray. 18 months postoperative: complete resolution of bone lesion.

Fig. 4: Successful LSTR 3MixMP in a lower left second molar with carious lesion involving pulp and interradicular radiolucency. A: Initial image. B: Xray. 6 months postoperative: reduction in interradicular radiolucency area and presence of new bone formation. CD: Xray. 12 18 months postoperative: complete resolution of bone lesion.
In 2016, we published a preliminary study on treatment with 3Mix-MP paste on 44 non-vital primary molars, using the same diagnostic and evaluation criteria as in the current study. Follow up at one month post-operatively showed only one clinically unsatisfactory treatment with persistence of fistula, and three radiographically unsatisfactory treatments with increase in the interradicular radiolucent area; with no further failure up to the final follow-up evaluation at 12 months18. Regarding to overall clinical success, in the current study we achieve a rate of 87.5% for LSTR 3Mix-MP, which is lower than the percentages reported by Prabhakar et al.19, Nakornchai et al.20 and Nanda et al.,21 who obtained 93% to 100% for 12-month follow-up periods. This difference may be due to the fact that follow-up in our study was 18 months. Other authors such as Trairatvorakul & Detsomboonrat22 and Duanduan et al.23 achieved lower clinical success rates (75% and 84.62%, respectively) in longer follow-up periods. This suggests that the clinical success rate for LSTR 3Mix-MP therapy decreases as post-treatment time increases.
Radiographic success results are more heterogenous; Nanda et al.21, Nakornchai et al.20 and our study had success rates higher than 75%, while Trairatvorakul et al.22 and Prabhakar et al.19 had success rates lower than 40%. The disparity in success rates may be due to the different selection and evaluation criteria employed. Trairatvorakul classified teeth with no evidence of bone regeneration at 6 months as failures, in contrast to the rest of the clinical studies in which non-progression of the radiographic lesion was considered as success for all evaluation times.
In a prospective study on 50 teeth, Nakornchai et al.20 compared 3Mix-MP and Vitapex® with 12-month follow-up, finding a clinical success rate similar to ours and a slightly lower radiographic success rate for Vitapex®. This may be because the study by Nakornchai et al.20 included molars with unfavorable baseline conditions for pulpectomy treatments.
In a retrospective study, Duanduan et al.23 compared pulpectomy treatments with Vitapex® and LSTR 3Mix-MP in 73 non-vital teeth for 6 to 72 months, finding no significant difference, either clinical or radiographic, between treatments (Vitapex 89% and 64.6%; 3Mix-MP 84.6% and 65.2%.). They also report that type of restoration and time between temporary and permanent restorations are significant factors in prognosis, concluding that LSTR therapy is simple, time-saving, places less psychological load on patients and should be especially considered for primary molars with poor prognosis for pulpectomy treatments.
Other researchers report slightly higher success rates with modifications to the antibiotic paste. Pinky et al.24, Nanda et al.21 and Doneira et al.25 replaced metronidazole with ornidazole, which has longer-lasting action, better efficacy and lower metabolism than metronidazole.
According to Kayalvizhi et al.,26 another factor impacting disparity in results may be the lack of standardization of the technique, the proportion of drugs and paste preparation.
Our study used equal parts of antibiotics, following Hoshino et al.5, and 2.5% NaOCl as irrigant, following Nakornchai et al.,20 due to its powerful antimicrobial activity and ability to dissolve organic tissue. Other authors employed saline solution or pulp chamber cleaners such as phosphoric acid or EDTA4,19,21,22,24
We consider it unnecessary to make small receptacles for the medication by enlarging the entrance to the canals (2 mm deep and 1 mm diameter) to contain more paste; given the porosity and permeability of the pulp chamber floor 27 which would facilitate rapid diffusion of 3Mix, in addition to the fact that it has been proven that propylene glycol, used as carrier in the paste, penetrates through dentinal tubules 10.
For the definitive restoration of treated molars, we used steel crowns, as did most authors. Steel crowns ensure a proper seal, preventing microfiltration, which is essential to repair28.
CONCLUSION
For the times studied, both treatments had similar clinical and radiographic behavior.
Pulpectomy with 3Mix-MP could be a valid option for treatment of non-vital molars in young or uncooperative patients.
FUNDING
This study was partly supported by a grant from the "Profesor Rodolfo Erausquin" Clinical Research Support Program of Buenos Aires University School of Dentistry, Argentina.
CORRESPONDENCE
Od. Giselle Anahí Zacharczuk
Cátedra de Odontología Integral Niños, Facultad de Odontología. Universidad de Buenos Aires. Marcelo T. de Alvear 2142 15° A. C1122AAH. Ciudad Autónoma de Buenos Aires, Argentina.
gisellezachar@yahoo.com.ar
1. American Academy of Pediatric Dentistry (AAPD). Guideline on pulp therapy for primary and immature permanent teeth. Revised 2014. [ Links ]
2. Maisto OA, Capurro MA. Obturación de conductos radiculares con hidróxido de calcio - yodoformo. Rev Asoc Odont Arg 1964; 52:167-173. [ Links ]
3. Fumes et al. Root canal morphology of primary molars: a micro computed tomography study. Eur Arch Paediatr Dent 2014. DOI 10.1007/s40368-014-0117-0 [ Links ]
4. Takushige T, Cruz EV, Asgor Moral MA, Hoshino E. Endodontic treatment of primary teeth using a combination of antibacterial drugs. Int Endod J 2004; 37:132-138. [ Links ]
5. Hoshino E, Kurihara-Ando N, Sato I, Uematsu H, Sato M, Kota K, Iwaku M. In vitro antimicrobial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int Endod J 1996; 29:125-130. [ Links ]
6. Sato I, Ando-Kurihara N, Kota K, Iwaku M, Hoshino E. Sterilization of infected root-canal dentine by topical application of a mixture of ciprofloxacin, metronidazol and minocycline in situ. Int Endod J 1996; 29:118-124. [ Links ]
7. Sato T, Hoshino E, Uematsu H, Noda T. In vitro antimicrobial susceptibility to combinations of drugs on bacteria from carious and endodontic lesions of human deciduous teeth. Oral Microbiol Immunol 1993; 8:172-176. [ Links ]
8. Alam T, Nakazawa F, Nakajo K, Uematsu H, Hoshino E. Susceptibility of Enterococcus faecalis to a combination of antibacterial drugs (3Mix) in vitro. J Oral Biosci 2005; 47: 315-320. [ Links ]
9. Windley W, Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod 2005; 31:439-443. [ Links ]
10. Cruz EV, Kota K, Huque J, Iwaku M, Hoshino E. Penetration of propylene glycol through dentine. Int Endod J 2002; 35:330-336. [ Links ]
11. Gomez Filho JE, Duarte PC, de Oliveira CB, Watanave S, et al. Tissue reaction to a triantibiotic paste used for endodontic tissue self-regeneration of nonvital immature permanent teeth. J Endod 2012; 380:91-94. [ Links ]
12. Niigata University Graduate School of Medical and Dental Sciences. Preparation of 3Mix-MP . 2003. URL: http://www.dent.niigatau.ac.jp/microbio/LSTR/background.html. [ Links ]
13. Nurko C, Garcia-Godoy F. Evaluation of a calcium hydroxide/ io- doform paste (Vitapex) in root canal therapy for primary teeth. J Clin Pediatr Dent 1999; 23:289-294 [ Links ]
14. Mortazavi M, Mesbahi M. Comparison of zinc oxide and eugenol, and Vitapex for root canal treatment of necrotic primary teeth. Int J Paediatr Dent 2004; 14:417-424. [ Links ]
15. Ozalp N, Sarolu I, Sonmez H. Evaluation of various root canal filling materials in primary molar pulpectomies: an in vivo study. Am J Dent 2005 ; 18:347-350. [ Links ]
16. Pramila R, Muthu MS, Deepa G, Farzan JM, Rodrigues SJ. Pulpectomies in primary mandibular molars: a comparison of outcomes using three root filling materials. Int Endod J 2016; 49:413-421. doi: 10.1111/iej.12478. [ Links ]
17. Trairatvorakul C, Chunlasikaiwan S. Success of pulpectomy with zinc oxide-eugenol vs calcium hydroxide/iodoform paste in primary molars: a clinical study. Pediatr Dent 2008; 30:303-308. [ Links ]
18. Toscano MA, Zacharczuk GA. Tratamiento con pasta 3Mix-MP en molares primarios no vitales: estudio preliminar. Bol Asoc Argent Odontol Niños 2016; 44:12-17. [ Links ]
19. Prabhakar AR, Sridevi E, Raju OS, Satish V. Endodontic treatment of primary teeth using combination of antibacterial drugs: An in vivo study. J Indian Soc Pedod Prev Dent 2008; 26:5-10 [ Links ]
20. Nakornchai S, Banditsing P, Visetratana N. Clinical evaluation of 3Mix and Vitapex as treatment options for pulpally involved primary molars. Int J Paediatr Dent 2010; 20: 214-21. [ Links ]
21. Nanda R, Koul M, Srivastava S, Upadhyay V, Dwivedi R. Clinical evaluation of 3 Mix and Other Mix in noninstrumental endodontic treatment of necrosed primary teeth. Journal of Oral Biology and Cranio facial research. 2014; 4:114-119. [ Links ]
22. Trairatvorakul C, Detsomboonrat P. Success rates of a mixture of ciprofloxacin, metronidazole, and minocycline antibiotics used in the non-instrumentation endodontic treatment of mandibular primary molars with carious pulpal involvement. Int J Paediatr Dent. 2012; 22:217-227. [ Links ]
23. Duanduan A, Sirimaharaj V, Chompu-inwai P. Retrospective Study of Pulpectomy with Vitapex® and LSTR with Three Antibiotics Combination (3Mix) for Non-Vital Pulp Treatment in Primary Teeth. Chiang Mai University Journal of Natural Sciences. 2013 12. 10.12982/CMUJNS.2013.0012.
24. Pinky C, Shashibhushan KK, Subbareddy VV. Endodontic treatment of necrosed primary teeth using two different combinations of antibacterial drugs: An in vivo study. J Indian Soc Pedod Prev Den. 2011, 29 : 121-127. [ Links ]
25. Doneria D, Thakur S, Singhal P, Chauhan D. Comparative evaluation of clinical and radiological success of zinc oxide-ozonated oil, modified 3mix-mp antibiotic paste, and vitapex as treatment options in primary molars requiring pulpectomy: An in vivo study. J Indian Soc Pedod Prev Dent 2017; 35:346-352 [ Links ]
26. Kayalvizhi G, Subramaniyan B, Suganya G. Topical application of antibiotics in primary teeth: an overview. J Dent Child 2013; 80:71-79. [ Links ]
27. Moss SJ, Addelston H, Goldsmith ED. Histologic study of pulpal floor of deciduous molars. J Am Dent Assoc 1965; 70: 372-379. [ Links ]
28. Seale NS, Randall R. The use of stainless steel crowns: a systematic literature review. Pediatr Dent 2015; 37: 145-160. [ Links ]

