










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.32 no.2 Buenos Aires Aug. 2019
ORIGINAL ARTICLE
Arch parameters and dental discrepancy (crowding and spacing) in a sample of an Afro-Colombian population
Parámetros de arco y discrepancia dental (apiñamiento y espaciamiento) en una muestra de población Afrocolombiana
Martha P. Rojas-Sánchez1, Gretel González-Colmenares2, Manuel F. Cevallos1, Lisseth A. Ortiz1, Diana C. Parra1
1 Universidad Antonio Nariño, Facultad de Odontología, Postgrado de Ortodoncia, Bogotá, Colombia.
2 Universidad Antonio Nariño, Facultad de odontología, Departamento de Investigación, Bogotá, Colombia.
Received: February 2019; Accepted: July 2019
ABSTRACT
The aim of this study was to determine the differences in arch length, inter-canine distance, inter-premolar distance, intermolar distance and arch shape between dental discrepancies (crowding and spacing) in a sample of dental casts from the Afro-Colombian population of San Basilio de Palenque. An analytical, cross-sectional study was conducted on a convenience sample of 63 subjects aged 11 to 57years, of Afro-Colombian origin, with full dentition from first molar to first molar, without extensive caries or restorations, and excluding casts with defects due to loss. The differences between arch (upper and lower) variables were analyzed according to dental discrepancies. Plaster models digitalized with a TR1OS3 Mono scanner with exactitude (6.9 ± 0.9 pm) and precision (4.5 ± 0.9 pm) were analyzed with Orthonalyzer software. Statistical analyses were done on SPSS software (Version 20 for Windows) and Real Statistics. Spacing discrepancy of68.25% was found for upper arch and 66.66% for lower arch; crowding discrepancy of 19.04% for upper arch and 20.63% for lower arch, and an adequate ratio of 12.69% for both arches. No statistically significant difference (p>0.05) was found between arch parameters except for inter-premolar distance on the lower arch. The most frequent arch shape in the population was oval for both upper arch, with 76.19%, and lower arch, with 71.42%. Tooth size was larger in males than females but the difference was not statistically significant.
Keywords: Dental arch, malocclusion, diastema; Dental crown; Jaw maxilla.
RESUMEN
El objetivo de este estudio fue determinar las diferencias en longitud de arco, distancia intercanina, interpremolar, intermolar y la forma de arco entre discrepancias dentales (apiñamiento y espaciamiento), en una muestra de modelos dentales de la población afrocolombiana de San Basilio de Palenque. Se realizó un estudio analítico transversal, en una muestra por conveniencia de 63 sujetos con un rango de edad entre 11 y 57 años, de origen afrocolombiano, quienes tuvieron dentición completa de primer molar a primer molar, sin caries extensas, ni restauraciones; se excluyeron los modelos con defectos por el vaciado. Se analizaron las diferencias entre las variables de los maxilares (superior e inferior) con las discrepancias dentales. Se utilizaron modelos de yeso que fueron digitalizados con el escánerTR1OS3 Mono con una exactitud de (6.9 ± 0.9 pm) y una precisión de (4.5 ± 0.9 pm)y analizados con el software Orthonalyzer. Los análisis estadísticos se llevaron a cabo utilizando el software SPSS (Versión 20 para Windows) y Real Statistics. Se encontró una discrepancia de espaciamiento de un 68,25% para el arco superior y 66,66% en el arco inferior; y una discrepancia de apiñamiento en el arco superior de 19,04% e inferior de 20,63% y una relación adecuada de 12,69% para los dos arcos. No se encontraron diferencias estadísticamente significativas (p>0.05) en los parámetros de arco a excepción de la distancia interpremolar del arco inferior. La forma de arco más frecuente en la población fue ovalada tanto en el arco superior con un 76,19% como en el arco inferior con un 71,42%. En cuanto al tamaño dental, se presentó mayor tamaño en los hombres que en las mujeres, pero este no fue estadísticamente significativo.
Palabras clave: Arcada dental, maloclusión, distema; Corona dental; Maxilar superior.
INTRODUCTION
Jaws undergo a number of changes during growth and development, beginning with the embryo stage and continuing through the development of deciduous and permanent dentition1. In 2015, Mauad et al.2 reported that the greatest changes in size and shape of the jaws occur at two important times during growth and development: the first during the deciduous dentition period (approximately 3-6 years of age) and the second during the eruption of permanent dentition and until it is functional. These changes involve the size and shape of dental arches and continue to occur until the growth stage has been completed3. Jaws change in size and shape as a result of multiple factors, including bone remodeling, position of teeth, sutural expansion of the upper jaw, nutrition, environment and genetics, among others4-6.
Adequate growth should lead to proper occlusion between jaws, although in this regard, tooth size should also be taken into account7. Tooth size should correlate appropriately with the size of the bony bases, since any discrepancy between them could cause crowding or spacing8, with impacted, rotated, displaced or excessively spaced teeth9. The causes of discrepancy are not yet absolutely clear. They have been related to different etiologies, such as reduction in arch size, tooth size, and relationship between tooth size and number of teeth10.
The association between dental crowding and tooth and arch size have been studied previously. Howe et al.11 reported that crowding was associated to smaller dental arches rather than to larger teeth. Mills12 reported a significant correlation between crowding and arch width. Radznic13 established that arch length is highly correlated to crowding. Tooth-size discrepancy can also cause crowding or spacing, and tooth mesiodistal width is considered a primary etiological factor in spacing anomalies causing malocclusion14. Barrett15 showed that tooth position in the dental arch can be determined considering tooth size and amount of space available for teeth in the dental arch. Fastlicht16 reported two factors responsible for dental crowding: larger tooth mesiodistal dimensions and smaller dental arch sizes. In 2018, Haidi et al.17 conducted a study on a Saudi population, finding that tapered dental arches were prevalent, with males having larger arches than females, and discrepancy in tooth size in the anterior segment. In 2000, Burris18 reported that American blacks had square dental arches, and that they were larger than in whites. There is little information available on the shape and size of dental arches in Colombian populations. Different facial features may influence dental arch shape and be related to the bony bases19. In 2016, Rodríguez et al.20 conducted a study on Colombians of three ethnic descents, including a sample of Afro-
Colombian population from Puerto Tejada, Cauca, on dental arch shape and size, finding that the oval is the most frequent in all ethnic groups for both jaws. Inter-canine distance varied among arch shapes, with significant difference in the upper arch, particularly in triangular arches. No significant difference was found between upper and lower arch shape.
Populational studies have shown that there is a wide range of tooth sizes17; e.g., American blacks have significantly larger dental crown size than American whites21, though they have been reported to have more spacing on the arches22. Other studies have shown variations in crowding and spacing in different ethnic groups. Spacing prevalence ranges from 6% to 50%, and crowding ranges from 5% to 80% in different populations23-25.
The population in Colombia is considered mestizo, as a result of a mixture of three large populations: indigenous, African and European, which began at the time of the conquest with the arrival of Europeans, mostly Spaniards, who brought with them African slaves26. Currently there are relatively isolated Afro-Colombian populations, such as the people of San Basilio de Palenque, who have kept alive many of their customs, as well as maintaining their genetics. Genetic studies on the population of San Basilio de Palenque show a high African component, with haplogroup E1b1a-M2 from eastern Africa, indicating that these people probably have unaltered African heritage26-28. The aim of the current study was to determine differences in arch length; inter-canine, inter-premolar and intermolar distances, and arch shape between dental discrepancies (crowding and spacing) in a sample of dental casts from the Afro-Colombian population ofSan Basilio de Palenque. Although Afro-descendant communities have been reported to have larger teeth than other populational groups, they also have a high frequency of diastemas, so it is assumed that this tooth size-arch length discrepancy may be due to greater arch length and inter-canine, interpremolar and inter-molar distances.
MATERIALS AND METHODS
An analytical, cross-sectional study was performed on a sample of 63 casts from 32 males and 30 females, aged 11 to 57 years, of Afro-Colombian origin, from the town of San Basilio de Palenque, Mahates Bolívar district, Colombia, who signed informed assent and consent. Casts were taken on subjects who had complete permanent dentition from first molar to first molar, upper and lower, without previous orthodontic treatment, without extensive caries, restorations or rehabilitations on the mesial and distal surfaces. Casts with impression defects, loss or fracturing, which prevented variables from being recorded, were excluded. This study was approved by the University ethics committee.
A TRIOS 3 Mono scanner was used to digitalize the plaster casts with exactness 6.9 ± 0.9 pm and precision 4.5 ± 0.9 pm. Orthonalyzer software was used to view the casts in 3D for analysis. First, the casts were formatted and canine tips, vestibular cusps for first and second molars, and mesiovesti-bular cusp of first upper and lower molars were located in order to measure the following distances: maxillary and mandibular inter-canine distance, distance between maxillary and mandibular first premolars, distance between maxillary and mandibular second premolars, maxillary and mandibular intermolar distance (Fig. 1). Maxillary and mandibular arch length was evaluated by measuring the distance between the vestibular surfaces of upper central incisors and another tangent line connecting the most distal points of the second premolars (Fig. 2). Arch shape was determined by superimposing square, oval and triangular arch shapes in occlusal view on the 3D cast, both upper and lower, and considering the shape most similar to the cast analyzed (Fig. 3).

Fig. 1: Measurement of transversal distance between homologous teeth on digital maxillary cast.

Fig. 2: Measurement of arch length on digital mandibular cast.

Fig. 3: Determination of arch shape on maxillary digital cast.
Dental arch discrepancy (crowding and spacing) was considered as the difference between arch perimeter and the sum of mesiodistal diameters from distal face of the second premolar to the distal face of the contralateral tooth, on both upper and lower arches. Arch perimeter (basal region available in the arch) was determined by adding the length segments of maxillary and mandibular arch (A1 B1 C1 D1) where A1 is the distance between the distal surface of the second right premolar to the mesial surface of the canine on the same side, B1 is the distance between the mesial surface of the right canine to the midline, C1 is the distance from the midline to the mesial surface of the left canine, D1 is the distance from the mesial surface of the left canine to the distal surface of the second premolar on the same side. The sample was classified into 3 groups: crowding (values less than -1 mm), spacing (values higher than 1 mm) and normal (values from -0.9 mm to 0.9 mm).
Statistical analysis was performed using SPSS software (Version 20 for Windows) and RealStatistics. All measurements were taken by a single observer, trained in taking measurements. To determine intrarater error, measurements were taken 15 days apart for 19% of the sample, and Bland Altmand graphs29 and Dahlberg and Houston statistics30 were applied.
RESULTS
The results of the paired T-test for each variable show that there was no difference in the average of the measurements taken by a single rater (p>0.05), accepting H0 for equal means. The Dalhberg values for each variable (0.30 mm, 0.40 mm, 0.28 mm, 0.40 mm, 0.39 mm, 0.30 mm, 0.30 mm) show control of the systematic random error for one rater. In the upper arch, mean distances between canines, between premolars (first and second), between molars and arch length were greater in males than females; nevertheless, there was no significant difference (p<0.05) between any of the variables in upper and lower arches (Tables 1 and 2).
Table 1: Comparison of upper arch variables for both sexes.
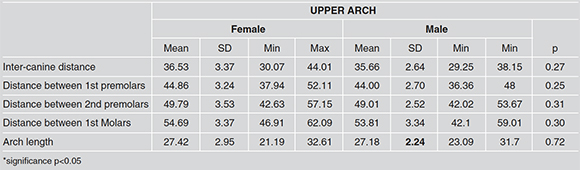
Table 2: Comparison of lower arch variables for both sexes.

No significant difference was found between sexes for upper and lower tooth size (p>0.05) although measurements were greater for males than females (p<0.05) (Tables 3 and 4).
Table 3: Comparison of upper tooth sizes per sex.

Table 4: Comparison of lower tooth sizes per sex.

In the upper arch, spacing discrepancy was present in 68.25% of the sample, crowding in 19.04%, and normal ratio in 12.69%. For lower arch, there was spacing in 66.66%, crowding in 20.63% and normal ratio in 12.69%.
For upper arches, in subjects with spacing, 74.41% of the arches were oval, 18.59% were square and 6.97% were triangular. In subjects with crowding, 75.0% of the arches were oval, 25.0% were triangular and none square. In subjects with normal arch ratio, 87.54% of the arches were oval and 12.45% triangular (Table 5).
Table 5: Discrepancy ratio and arch shape in upper arch.

For lower arches, in subjects with spacing, 73.80% of the arches were oval, 14.28% square and 11.89% triangular. In subjects with crowding, 61.51% of the arches were oval, 30.73% triangular and 7.65% square. In subjects with normal ratio, 75.01% of the arches were oval and 24.98% were triangular (Table 6).
Table 6: Discrepancy ratio and arch shape in lower arch.

Tables 7 and 8 show means and SD for the different variables in the three groups (spacing, crowding and normal ratio) in upper and lower arches. The means for all variables were higher in the spacing group, except upper arch length, although there was no significant difference in the variables between groups (p>0.05).
Table 7: Descriptive analysis of Spacing, Crowding and Normal in upper arch.

Table 8: Descriptive analysis of Spacing, Crowding and Normal in lower arch.

To explore the groups internally, the categories spacing and crowding were divided. Crowding was considered moderate-to-severe in subjects with a difference greater than -4 mm in available space / required space ratio; and spacing was considered moderate-to-severe in subjects with a positive difference of +4 mm for this ratio. Comparison of the moderate-to-severe crowding and moderate-to-severe spacing groups showed significant differences (p<0.05) in the distances between first and second premolar for both arches (Tables 9 and 10).
Table 9: Difference between severe crowding and severe spacing in upper arch.

Table 10: Difference between severe crowding and severe spacing in lower arch.

DISCUSSION
The aim of this study was to determine differences in arch length; inter-canine, inter-premolar and intermolar distances, and arch shape among subjects with crowding and spacing dental discrepancies, in an Afro-descendant population, in which there is usually larger tooth-size and frequent presence of diastemas.
In the Afro-Colombian population study sample, we found a greater frequency of spacing discrepancy (68.25% for upper arch and 66.66% for lower arch). These results are similar to those reported by Burris18 for a black American population, in whom greater presence of spacing was found.
In this population, the frequency of spacing was high, but no significant difference was found in arch parameters between groups (crowding and spacing). However, because orthodontics traditionally classifies discrepancies as severe, moderate and mild, the sample was divided accordingly. Significant differences between inter-premolar distances were found between the extremes - severe crowding compared to severe spacing. This is in agreement with a study on a Pakistani population by Faruqui31. However, our results differ from other studies in which the difference was greater for inter-canine and inter-molar distances17,20. These results should be considered with caution, due to the small sample size. The most frequent arch shape in the study population was “oval”, both for upper arch (78.98%) and lower arch (70.10%). These results are in agreement with Bedoya-Rodriguez et al.20, who found a frequency of 78.6% oval for upper arch and 74.3% for lower arch in an Afro-descendant population in the Cauca Department, Colombia. However, our results differ from those reported by Burris18 in American blacks, in whom the most frequent arch shape was square. These results may be a consequence of allometries in the growth and development processes in North American and Latin American populations.
Comparison between sexes showed no significant difference in study variables. Therefore, no distinction is made according to sex, and the sample is taken as a single group, in contrast to other studies that found significantly larger measurements in males than in females for all variables6,18.
Dental crowding and spacing are known to be the outcome of several etiological factors in permanent dentition. However, discrepancy in the mesiodistal size of upper and lower teeth is considered to be a determining factor12,14. Although there is no statistically significant difference in tooth size between sexes, teeth were slightly larger in males than in females, whereas transverse arch measurements were greater in females. For orthodontic diagnosis, the amount of space deficiency or excess in the arch is usually established according to the mesiodistal size of teeth and the perimeter of the arches 32-34. Some studies suggest that other factors, such as tooth shape, bony base shape, arch length and arch transversal width play an important part in special discrepancies and have implications in the diagnosis and treatment plan5,6,17,18.
Crowding is also caused by dental compensation to problems of arch-length discrepancy. The current study did not consider this variable because profile radiographs were not available. It is therefore recommended to use craniofacial radiographs in future studies in order to relate malocclusions to dental discrepancies, considering that this population tends to have biprotrusion35.
Inclination of tooth long axes may be one of the reasons for spacing. Maxillary teeth, particularly incisors, tend to be more inclined over the basal arch, as mentioned by Moorrees8 in a study finding that the teeth in the mandibular arch had considerable inclination with respect to the occlusal plane and therefore the maxillary dental arch presented a larger circumference than the bony base arch.
A possible cause of dental discrepancy (spacing and crowding) in the study sample may be alterations in tooth size, considering that diagnostic exploration found low Bolton’s index in 34.9% of this population14.
One of the limitations in this study is the lack of standardization in transverse arch measurements. Some authors use palatine and lingual cusps as reference points8, others measure from the distal fossae in premolars to the central fossa in molars29,36 and still others consider vestibular cusps, as we did in the current study17,18. Nevertheless, the study sample is not consistent with the representation of the Afro-Colombian population, in addition to which oral status made it difficult to meet the exclusion criteria because the population is highly susceptible to dental caries and edentulism37.
One of the problems in odontometric studies is the low reproducibility of measurements. In this study, error was controlled by ensuring that the rater was sufficiently trained to achieve consistent results. Analyses for orthodontic diagnosis should take into account that if standards from other populations are used, tooth size may vary as a result of sexual dimorphism, greater ethnic influence or specific kinds of malocclusion33. It is therefore essential to evaluate the patient individually rather than according to measurements or analyses performed on other populations.
The current study found no significant differences for arch parameters (arch length, arch shape, inter-canine distance, inter-premolar distance, intermolar distance, arch perimeter, tooth size) of dental discrepancies (crowding and spacing). Greater spacing discrepancy was found for both arches. Moreover, no significant differences were found for the variables (arch length, arch shape, inter-canine distance, inter-premolar distance, inter-molar distance, arch perimeter, tooth size) between males and females. The most frequent arch shape was oval. For subjects with spacing, the upper arch was oval in 74.41% and the lower arch was oval in 73.80%. For subjects with crowding, the upper arch was oval in 75.0% and the lower arch was oval in 61.51%. There were significant differences for inter-premolar distance in the lower arch when severe crowding and severe spacing were compared. Diagnosis of dental discrepancies should consider not only arch size and tooth size, but also tooth inclination and the individual skeletal component.
ACKNOWLEDGMENTS
We thank the people of San Basilio de Palenque for cooperation with sampling, and the municipal authorities of the town for their cooperation. We also thank Dr. Tomas Castellanos for loaning the scanner, software and facilities for conducting this study.
FUNDING
None
CORRESPONDENCE
Dra. Gretel González-Colmenares
Carrera 3 E, No. 47A-15, Bloque 5, Bogotá, Colombia
gretgonzalez@uan.edu.co
1. Sillman JH. Dimensional changes of the dental arches: Longitudinal study from birth to 25 years. Am J Orthod 1964; 50:824-842. [ Links ]
2. Mauad BA, Silva RC, Aragón MLS de C, Pontes LF, Silva Júnior NG da, Normando D. Changes in lower dental arch dimensions and tooth alignment in young adults without orthodontic treatment. Dental Press J Orthod 2015;20:64-8. [ Links ]
3. Lazenby RA. Continuing periosteal apposition II: The significance of peak bone mass, strain equilibrium, and age-related activity differentials for mechanical compensation in human tubular bones. Am J Phys Anthropol 1990; 82:473-84. [ Links ]
4. Harris EF. A longitudinal study of arch size and form in untreated adults. Am J Orthod Dentofacial Orthop 1997; 111:419-27. [ Links ]
5. Correia GDC, Habib FAL, Vogel CJ. Tooth-size discrepancy: A comparison between manual and digital methods. Dental Press J Orthod 2014; 19:107-113. [ Links ]
6. Cassidy KM, Harris EF, Tolley EA, Keim RG. Genetic influence on dental arch form in orthodontic patients. Angle Orthod 1998; 68:445-454. [ Links ]
7. Arbeláez CJ. Discrepancias de tamaño dental (índice de Bolton) en una muestra de modelos digitales tridimensionales de pacientes con oclusión ideal; validación del método y descripción de hallazgos métricos (tesis Posgrado de Ortodoncia. Universidad Nacional de Colombia, Bogotá, Colombia. 2015. URL: http://bdigital.unal.edu.co/50061/1/Discrepancias%20de%20tama%C3%B1o%20dental%20%28%C3%ADndice%20de%20bolton%29%20en%20una%20muestra%20de%20modelos%20digitales%20tridimensionales%20de%20pacientes%20con%20oclusi%C3%B3n%20ideal%3B%20validaci%C3%B3n%20del%20m%C3%A9todo%20y%20descripci%C3%B3n%20de%20hallazgos%20m%C3%A9tricos-Catalina%20Jaramillo%20Arbel%C3%A1ez-2015.pdf [ Links ]
8. Moorrees CFA, Reed RB. Biometrics of crowding and spacing of the teeth in the mandible. Am J Phys Anthropol 1954; 12:77-88. [ Links ]
9. Merz ML, Isaacson RJ, Germane N, Rubenstein LK. Tooth diameters and arch perimeters in a black and a white population. Am J Orthod Dentofac Orthop 1991; 100:53-58. [ Links ]
10. Bolton W. Disharmony in tooth size and it relation to the analysis and treatment of malocclusion. The Angle orthodontist 1958; 28:113-130. [ Links ]
11. Howe RP, McNamara JA, O’Connor KA. An examination of dental crowding and its relationship to tooth size and arch dimension. Am J Orthod 1983; 83:363-73.
12. Mills LF, Hamilton PM. Epidemilogical studies of malalignment of Malalignent, A Methodfor computing Dentalarch Circumference. Angle Orthod 1965; 35:244-248. [ Links ]
13. Radnzic D. Dental crowding and its relationship to mesiodistal crown diameters and arch dimensions. Am J Orthod Dentofac Orthop 1988; 94:50-6. [ Links ]
14. Bolton WA. The clinical application of a tooth-size analysis. Am J Orthod 1962; 48:504-529 . [ Links ]
15. Barrett MJ, Brown T, Macdonald MR. Dental observations on Australian aborigines: mesiodistal crown diameters of permanent teeth. Aust Dent J 1963; 8:150-6. [ Links ]
16. Fastlicht J. Crowding of mandibular incisors. Am J Orthod Dentofacial Orthop 1970; 58:156-63 [ Links ]
17. Haidi, O. Alhajrasi M, Felemban N, Hassan A. Dental arch dimensions, form and tooth size ratio among a Saudi sample. Saudi Med J 2018; 39:86-91. [ Links ]
18. Burris BG, Harris EF. Maxillary Arch Size and Shape in American Blacks and Whites. Angle Orthod 2000; 70:297302. [ Links ]
19. Bravo YL, Burbano PE, Bedoya A,Osorio JC, Tamayo J, Martinez CH. Variabilidad de las medidas de los arcos dentales y su relacion con la diferenciacion poblacional -Revision sistematica.Rev. Colomb Investig en Odontol 2015; 5:157-175. URL: https://pdfs.semanticscholar.org/b3cd/64ac6d2953e9660cb801cf9ca5c6af31f418.pdf [ Links ]
20. Bedoya-Rodrígez A, Montoya-Gómez J, González-Benavidez V, Tamayo-Cardona J, Martínez-Cajas H. Forma y tamaño del arco dental en poblaciones de tres ascendencias étnicas colomianas. Ces Odontol 2016; 29:20-32. [ Links ]
21. Richardson ER, Malhotra SK. Mesiodistal crown dimension of the permanent dentition of American Negroes. Am J Orthod 1975; 68:157-64. [ Links ]
22. Kelly JE, Harvey CR. An assessment of the occlusion of the teeth of youths 12-17 years. Vital and health statistics.
Series 11, Data from the national health survey. 1977; 162:1-65. URL: https://www.cdc.gov/nchs/data/series/sr_11/sr11_162.pdf
23. Gábris K, Márton S, Madléna M. Prevalence of malocclusions in Hungarian adolescents. Eur J Orthod 2006; 28:467-70. [ Links ]
24. Mugonzibwa EA, Eskeli R, Laine-Alava MT, Kuijpers-Jagtman AM, Katsaros C. Spacing and crowding among African and Caucasian children. Orthod Craniofacial Res 2008; 11:82-89. [ Links ]
25. Hack GD, Patzelt SBM. Evaluation of the Accuracy of Six Intraoral Scanning evices: An in-vitro Investigation. ADA Prof Prod Rev 2015; 10:1-5. URL: https://www.beldental.cz/upload/useruploads/files/ke_stazeni/evaluation_of_the_accuracy_of_six_intraoral_scanning_devices.pdf [ Links ]
26. Noguera MC. Estudio molecular de estructura Genética en poblaciones indígenas y afrocolombianas mediante marcadores nucleares y mitocondriales. 2011; 1-271. URL: https://repository.javeriana.edu.co/handle/10554/16657. [ Links ]
27. Padilla M, Tello L, Moreno F, Osorio JC, Bedoya A. Analysis of Dental Arch Dimensions in Three Colombian Ethnic Groups. Int J Morphol 2013; 31:100-106. [ Links ]
28. Mesa NR, Mondragon MC, Soto ID, Parra MV, Duque C, Ortiz-Barrientos D, et al. Autosomal, mtDNA, and Y-chromosome diversity in Amerinds: Pre- and PostColumbian patterns of gene flow in South America. Am J Hum Genet 2000; 67:1277-1286. [ Links ]
29. Houston, WJ. The analysis of errors in orthodontic measurements. Am J Orthod 1983; 83: 382-390. [ Links ]
30. Dahlberg G. Statistical methods for medical and biological students. Br Med J 1940; 2(4158): 358-359. URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2179091/pdf/brmedj04110-0016c.pdf No se encontró en PubMed. [ Links ]
31. Faruqui S, Fida M, Shaikh A. Comparison of tooth and arch dimensions in dental crowding and spacing. POJ 2012; 4:48-55. URL: http://applications.emro.who.int/imemrf/Pak_Orthod_J/Pak_Orthod_J_2012_4_2_48_55.pdf [ Links ]
32. Kundi IU, Bashir U, Zahid S, Shaheed S, Usman K. Bolton tooth size analysis of pakistanis of 13 to 20 years in islamabad city. Pakistan Oral Dent J 2012;32:421-6. URL: http://podj.com.pk/archive/Dec_2012/p-14.pdf [ Links ]
33. Lacerda dos Santos R, Melo M. Discrepancia Dentaria de Bolton y Finalización de Ortodoncia: Consideraciones Clínicas. Int. J. Odontostomat 2010;4:93-100. URL: http://dx.doi.org/10.4067/S0718-381X2010000100014 [ Links ]
34. Cuanalo LO, González de la Fuente MV, Nácar MS, Santillán NP, Sánchez CL, Moreno W. Forma de los arcos dentales en pacientes atendidos en la clínica multidisci-plinaria Zaragoza. Vertientes 2011;14:82-87. URL: https://www.medigraphic.com/pdfs/vertientes/vre-2011/vre112d.pdf [ Links ]
35. McKoy-White J, Evans CA, Viana G, Anderson NK, Giddon DB. Facial profile preferences of black women before and after orthodontic treatment. Am J Orthod Dentofac Orthop 2006;1:17-23. [ Links ]
36. Alvaran N, Roldan SI, Buschang PH. Maxillary and mandibular arch widths of Colombians. Am J Orthod Dentofac Orthop 2009; 135:649-656. [ Links ]
37. IV Estudio Nacional De Salud Bucal ENSAB IV. MINSALUD. 2014. URL: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/ENSAB-IV-Situacion-Bucal-Actual.pdf [ Links ]

