











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
In spite of the controversy regarding success rates of conventional endodontic therapy, it is a fact that with the continuous improvement of instruments and techniques, high indexes are obtained, approximately 88%1. In case of failure, clinicians may and must decide for endodontic retreatment, that has 80% success rates, an evidence of its effectiveness2.
When there is failure in retreatment or when this practice is contraindicated, surgical therapy may be a solution for teeth maintenance. Such procedure consists in exposing the apex of the root, in performing apical resection, apical retropreparation and then sealing with retrofilling material3, 4.
Apical sealing is the most important surgical success factor resulting from the use of retrofilling material, which can prevent bacterial activity and bacterial by-products inside the root canal and in periapical tissues5, 6. Periapical infections may be resistant to antimicrobial therapy and only paraendodontic surgery can produce disinfection and enhance tissue repair7. Success indexes of paraendodontic surgeries performed according to modern concepts account for 88,4%8 .
Materials have been developed through time and their properties have been improved. This has changed the materials of choice for retrofilling. Mineral Trioxide Aggregate (MTA) - developed at the University of Loma Linda in the early 1990's 9 -presents advantages vis a vis previously used materials, due to its sealing ability, marginal adaptation and biocompatibility10, 11, 12. MTA has been the most widely used retrofilling material, yet, it has some limitations, such as long setting time, difficulty in handling and maintaining the mixture consistency13,14.
Retrocavity preparation may be performed after resection at an angle of 45° or 90° with respect to the long axis of the tooth. For many years, the 45° -angled section was used as it enabled the visual and manual access to the apical region15. This angling enhances the exposure of dentinal tubules, enabling higher microleakage levels and resulting in keeping the lingual/palatal root portion without the adequade treatment16,17. In the case of the 90° resection, it enables a better crown/root proportion as it preserves more dental structure and promotes less leakage18,19. Retrocavities need to have at least a 3-mm depth for a more effective and a safer sealing action16. The use of spherical burs for making these retrocavities means that a root resection at 45° should be made for chamfering the root and having manual access, which tends to promote a higher periapical per-meability20,21. However, by using angled ultrasound tips for the apical retropreparation, it was possible to get a more even and conservative preparation, when compared with the spherical burs 22 making it unnecessary to chamfer the root portion and permitting that a 90°-angle resection be made20.
The purpose of this research was to evaluate apical microleakage in diaphonized and MTA-retrofilled teeth, by using 45° and 90° apical section angles, through the dyeing (India Ink) method analysed by stereo microscope.
MATERIALS AND METHODS
The research project was submitted to the Ethics Committee in Research with Humans of the University of Itauna. The project was approved and protocol N° 421.819 was then assigned.
Twenty-six central superior, uniradicular incisors, with a completely formed apex, were used in the research study. The teeth were cleaned, sterilized in autoclave and previously submerged in saline solution, at the beginning of the procedures. Periapical X-Rays were made for evaluating the absence of calcifications, reabsorptions or of any previous endodontic treatment.
After selecting the teeth, access to their crowns was performed using the high rotation carbide bur 1557 (KG Sorensen, Sâo Paulo, Brazil), and subsequently, the ceiling of the pulp chamber was removed, with the high rotation Endo-Z bur (Dentsply Maillefer, Ballaigues, Switzerland). The teeth were instrumented using the Oregon Technique, with manual K-type files. The patency was established by means of the K #10 file (Dentsply Maillefer, Ballaigues, Switzerland) and the length of the canal was determined through visualization of the K #15 file (Maillefer, Ballaigues, Switzerland) in the apical foramen. The length of the task was determined as being 1 mm beyond the apical foramen. Gates-Glidden #2 and #4 Burs (Maillefer, Ballaigues, Switzerland) were used for preparing the two coronal thirds of the dental roots; the apical third was standardized in all the teeth with a K-type #45 file (Maillefer, Ballaigues, Switzerland). During instrumentation, 2 ml of a NaOCL solution were used for canal irrigation. The final irrigation was done with 3 ml of Ethylenediaminetetraacetic acid (EDTA) 17% (Formula & Action, Sâo Paulo, Brazil) for 60 s, followed by 2 ml of NaOCl 2,5%. Before the filling procedure, the canals were completely dried with absorbent paper cones (Dentisply Maillefer, Ballaigues, Switzerland). The filling procedure was done through the lateral condensation technique by using a digital spacer digital #25 (Odous de Deus, Belo Horizonte, Brazil), Endofill cement filling (Dentisply Maillefer,
Ballaigues, Switzerland) and gutta-percha cones #45 and accessory cones R1 (Dentisply Maillefer, Ballaigues, Switzerland). Three millimeters of the root crown portion were removed and, then, sealing was done by using IRM (Dentsply/Caulk, Milford, USA).
Subsequently, the samples were divided into two groups: A (n=10) and B (n=10). By using a millimetered ruler, in the apical third of the teeth a 3 mm standard marking was made at the points where the samples were resected. In Group A, the root-end was resected at an angle of 90° with the long axis of the tooth, by means of a high rotation multilaminated Zekrya bur (Dentsply-Maillefer, Ballaigues, Switzerland), with constant irrigation. The section was done from the mesial surface up to the end of the root distal surface. In Group B, the same procedures were applied, however, the apical resection was performed at a 45° cutting angle with the axis of the tooth.
After apicoectomy, the cavities were shaped with the Retro-D700 ultrasonic tip adapted to the ENAC ultrasonic device (Osada, Tokyo, Japan), by applying medium-power and under constant irrigation, with standardized 3 mm cavity depth and diameters. The samples were covered with two layers of enamel, except for the apical 3 mm portion. Six teeth were used as a negative control and all the surfaces of the dental structure were covered with two layers of enamel, showing the effectiveness of the enamel as a barrier to dye penetration. Retrofillings were irrigated with EDTA, 24%, during 3 minutes and then carefully rinsed with water for removal of excess of EDTA. The chosen retrofilling material was white MTA (Angelus, Londrina, Brazil), handled according to the manufacturer's label and inserted into the cavities by using an MTA applicator (Angelus, Londrina, Brazil). After the handling procedure, and according to the manufacturer's label, an initial 15-minute lapse was considered for letting the MTA set.
After these procedures, the teeth were submerged in Indian ink and placed in a microbiological oven at 37°C, and 100% Relative Humidity, during 48 hours. Subsequently, the samples were withdrawn from the oven and placed on surgical bandage to remove the excess of dye. Then, they were left at room temperature during 24 hours for dye fixation. Subsequently, the teeth were decalcified in hydrochloric acid, 5%, during 3 days, rinsed during 24 hours, and dehydrated in incremental alcohol solutions (70%, 80%, 90% and 100%, respectively) during 4 hours, a diaphonization technique previously described by Vertucci 23. Then, the teeth were clarified using methyl salicylate, and remained like this until the analyses24. An examiner, trained and calibrated for identifying lineal dye penetration, performed the analyses of the samples.
Then, the teeth were photographed and evaluated in a stereosmicroscope (Leica Microsystems, Heerbrugg, Switzerland) with a 20X magnification, for observing the dye penetration process along the root-end surfaces. The lineal distance of the dye penetration was measured using the Image J software. This was transferred to a Microsoft Office Excel sheet and, then, to SigmaPlot program (Systat Software Inc. version 8.0, San Jose, CA, USA). The measurements of the lineal dye microleakage in both groups were analysed using a Student's-t test, with a p<0.05 significance level.
RESULTS
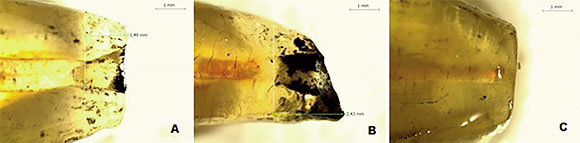
The measurements of the lineal dye microleakage of both groups are exhibited in Fig. 1 and illustrated in Fig. 2. The statistical Analysis showed a significant difference between Groups A and B (p=0.004). Both sections showed apical microleakage, yet, the group resected at 90° showed less leakage than the group with a 45° section in relation to the long axis of the tooth.
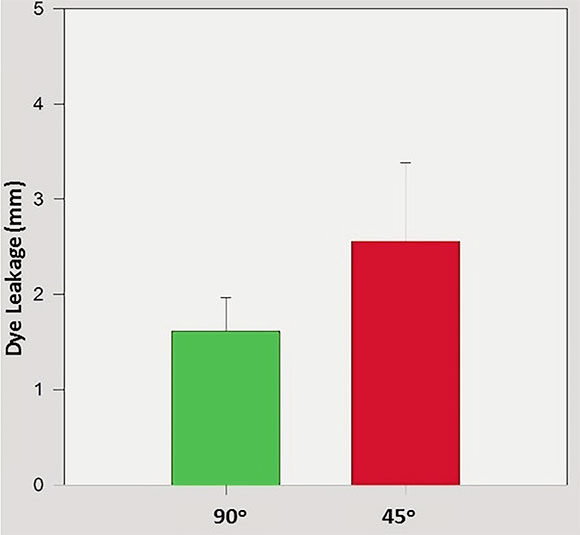
Fig. 1 Measures (arithmetical means) of microleakage in Group A (green column) and Group B (red column) in millimeters (mm). The vertical lines stand for standard deviations.
DISCUSSION
In spite of the limitations of in vitro research studies, such studies are very valuable for developing endodontic techniques and materials, leading to relevant information for clinical practice25.
Analysis using diaphonization permits the direct visualization of the internal anatomy of the root canal system and enables measuring lineal dye leakage in the interface dentin/retrofilling material. Diaphonization, which was used in previous Endodontia research studies, is a user-friendly method, with good sensitivity levels and no need for sophisticated methods and equipment. The dye used has a penetration capability similar to that of endodontic bacteria. This permits associating the outcomes of this in vitro study with those of the clinical study24-26.
The relation between apical section angling and microleakage has been approached in several research studies, through different methodologies3-79. In this research, diaphonization was the analytical method chosen as it enables the internal visualization of retrofilled teeth and of the apical third dyed by penetration of Indian ink. By means of diaphonization, it was possible to have a 3D view of all the surfaces of the tooth and, consequently, to have a good access for determining the penetration of the dye27,28. In literature, there are studies in which the chosen methodology was vertical dental resection for analysis of microleakage, yet, this technique restricts the visual access to retrocavity peripheral areas and deteriorates the adequate evaluation of dye penetration, not simulating a real clinical situation18 29.
Periapical surgeries are additional therapeutic procedures for teeth maintenance that may and must be applied in cases of failure of treatment and/or of endodontic retreatment, provided they are well prescribed and performed8,20.
With the development of dental materials, more desirable properties have been obtained for different clinical scenarios. Among such materials, MTA should be pointed out. MTA is undergoing extensive research and has shown to have physical and chemical features that make it appropriate for retrofilling, specially because it is biocompatible and helpful in tissue repair processes9-13. It is considered that this favorable biological response of MTA results in hydroxyapatite formation, useful in post-surgical bone repair28.
The manufacture of ultrasonic angled tips has turned apical bevelling unnecessary as these tips allow clinicians to perform more uniform retropreparation, with parallel walls that make it easier to insert and adapt the filling material. Besides, it minimizes major leakage episodes associated with the augmented exposure of tubules caused by the 45° resection, as shown in this research study17 18 3031.
Lin et al. compared two retropreparation techniques -with ultrasonic tips and with the traditional spherical bur technique - using stereomicroscopy for evaluating the quality of the shape and size of a given retropreparation. The outcomes of such research study showed that the preparations with ultrasonic tip were more conservative and that there was a smaller number of root perforations than in the preparations with the spherical drills19.

