











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Orthodontic treatments use 2D X-rays as a fundamental part of diagnosis to determine dental or bone injury, pathologies, root parallelism, tooth inclinations, and growth during treatment1. In dentistry, 3D radiology complements this tool. The company Quantitative Radiology (Verona, Italy) introduced the first Cone Beam Computed Tomography (CBCT) for dental use in the year 2000 in Loma Linda University, USA2. This new tool has significant advantages such as low radiation dose, a 1:1 ratio of bone structures and shorter shooting times than 2D X-rays and computed axial tomography (CAT). The companies involved in 3D tomography have provided different options to the orthodontist, making it important to analyze each tomogram and corroborate the accurate measurement of anatomical structures. The 1:1 ratio has been demonstrated in many cases; however, when highly accurate measurement of thin structures is required for cortical bone, the reliability of 3D tomography decreases3, 4.
The alveolar bone is formed by the projection of the external and internal cortical bone and provides support to the teeth and soft tissues. The determination of alveolar bone height helps to establish the limitations in orthodontic treatments, e.g., in biomechanical expansion or closure of spaces, movements could cause or aggravate fenestrations or dehiscences in the alveolar crest, especially if the diagnosis was incorrect. Biomechanical and biological factors are closely related and determine the collateral effects of potential treatment such as root resorption, gingival recession, dehiscence and fenestrations5, 6.
Three-dimensional imaging through a CBCT scan is important because it can reveal fenestrations and dehiscences. These types of alveolar defects are common, especially in hyper-divergent patients and increased lower facial height7,8. A previous study of 1872 teeth reported high prevalence of these defects in hyper-divergent (8.35%) and normo-divergent (8.18%)6 subjects. In another study, i-CAT™ was performed on 123 scans, showing that the presence of fenestrations and dehiscences did not vary significantly between skeletal I, II or III malocclusion9.
In terms of measurements on CBCT, it has been found that linear measurements are reliable, but the presence of soft tissue and voxel size influenced the results. Even when using a 0.125 mm voxel, the thin vestibular cortex of some external layers is not represented, hence, there is a considerable risk of overestimating the dehiscences or fenestrations viewed in a three-dimensional image10.
The correlation between linear measurements performed on a skull and the same measurements taken from tomographic images analyzed using
Dolphin® software has been assessed in the literature. It was demonstrated that many of the linear measurements differed significantly11. This highlighted the limitations of using this technology for studies in skulls. Several factors can influence the accuracy of the results, such as the attenuation of soft tissues, metal-based restorations and patient movement.
CBTC scans (0.4 mm voxel) were performed in pig jaws to measure the height of the vestibular alveolar bone in the molar region. The results showed that tomographic images can overestimate alveolar bone loss associated with rapid palatal expansion by 1.5 to 2 mm12.
The aim of this study was to investigate whether there is a significant correlation in the accuracy of the vestibular alveolar bone height measurement between direct and indirect techniques (0.16 mm voxel resolution CBCT), with the goal of validating this methodology and establishing its limitations. The importance of the present study is the observation of variables in living patients, and analysis of the representation of clinical reality in CBCT scans.
MATERIALS AND METHODS
This study was reviewed and approved by the Faculty of Dentistry Research Committee at the Benemérita Universidad Autonoma de Puebla (Mexico). The procedures adhered to ethical standards and there was no risk in the investigation according to the Regulation of the General Health Law on Research and Helsinki Declaration guidelines for research involving human subjects. The intraclass correlation coefficient for the vestibular alveolar bone height measurements of both researchers was 0.980. The inter-researcher's Pearson's correlation coefficient for the direct technique (Vernier caliper measurement) was 0.990, and for the indirect technique (CBCT at 0.16 mm) it was 0.986. Thus, direct and indirect measurements were consistent and reproducible for each researcher.
Eight patients were invited to participate in the study, under informed consent, to receive open curettage treatments. The protocol included a sample of 30 teeth that were exposed to a fullthickness flap during debridement. The study included incisors and premolars of patients of different ages and genders, and excluded teeth with extensive restorations that could affect the tomographic image.
The procedure included patients who required flap elevation for their periodontal procedure which enabled us to perform the measurements. A copy of the CBCT scan was delivered to the specialist who was treating the patients for diagnostic purposes without additional cost.
Patients were exposed to one CBCT scan after clinical procedures. Precautions were taken to minimize the radiation dose, in view of the "As Low as Reasonably Achievable" (ALARA) principles. Exposure time was kept as short as possible, good hygiene practices were followed and proper use was made of personal protective equipment such as lab coats, disposable gloves and safety glasses. The design and execution of this study were subjected to Institutional Review Board oversight (IRB). Patients who were scheduled to receive radiation from cone-beam tomographic images were prospectively enrolled in an IRB-approved study.
Direct measurement technique
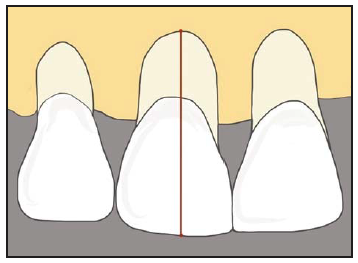
Once the flap was performed and after elimination of dental calculus, the height of the vestibular alveolar bone was measured from the incisal, occlusal edge or the vestibular cusp, along the longitudinal axis of the tooth to the end of the observable vestibular alveolar bone using a digital Vernier caliper Stainless Steel Professional, with an error range of 0.01 mm. Three independent measurements were carried out by two researchers before the periodontist placed the suture (Fig. 1).
.
Indirect measurement technique
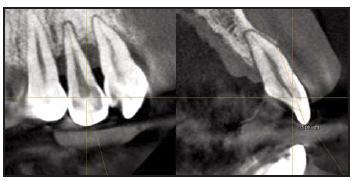
Subsequently, the patient was taken to the radiology department to perform the image study using an Orthophos XG 3D Sirona® scanner. This study was conducted according to the specifications suggested by the manufacturer: 12 mA, 90 kVp and 14.9-second exposure13. The field of view of the CBCT scans was 8x8x8 cm, with a resolution of 0.16 mm. The tooth was placed in axial, frontal and transverse views, taking care that the resulting tomographic sections always followed the longitudinal axis of the tooth. Using the measurement tool in the software, the digital ruler was placed from the incisal or occlusal edge to the end of the observable vestibular alveolar bone, as shown in Fig. 2. This measurement was repeated three times. An indirect measurement of the vestibular alveolar bone height of each tooth was previously measured directly.
.
The Kolmogorov-Smirnov test was employed to assess the data distribution. Means and standard deviations were calculated, and bivariate analysis, Pearson's correlation coefficients and paired t test were used to establish the significance of differences between the measurements. All the data were analyzed using IBM SPSS Statistics version 22 software. Tests were applied with p<0.05 level of significance.
RESULTS
The vestibular alveolar bone height based on 30 measurements for the direct technique (Vernier caliper measurement) was 11.92±2 mm, while for the CBCT indirect technique at 0.16 mm, it was 15.07±4 mm (Table 1). Mean dehiscences were overestimated by 3.15 mm (26%) on CBCT.
Paired t test demonstrated significant differences between direct measurement and SD CBCT (p= 0.001), as shown in Table 2.
Pearson's correlation coefficient (PCC) between direct and indirect measurements was 0.68, which is statistically significant (P<0.001) and indicates that linear correlation between parameters was moderate.
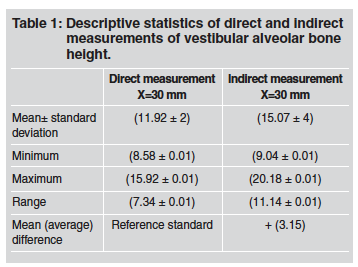
Table 2 Paired t test between measurement groups and limits of the confidence interval (95%) for the

DISCUSSION
Cone beam computed tomographic (CBCT) imaging has emerged as an important supplemental radiographic technique in different areas. In this study, low-resolution CBCT values differed significantly from the values measured using Vernier caliper. Even though the voxel size of the CBCT Orthophos XG 3D is one of the smallest and most accurate available, the results of this study are consistent with those of Sun et al.12, who reported discrepancies of up to 2 mm between direct and indirect measurements. The current study showed discrepancies of up to 3 mm between techniques, probably due to the thinness of the cortical layer. Leung et al.4 compared direct and indirect measurements, finding a threefold higher incidence of fenestrations when measuring using CBCT compared to direct measurement, and more false positives. There were also false negatives in which CBCT showed no real defects, with more than half of the dehiscences not detected by CBCT.
However, Patcas et al.10 and Timock et al.14 found no significant difference between direct and indirect measurements. The importance of the current study is that it considers the variables present in a living patient and shows the clinical reality of the tomograms. These variables may generate discrepancies between studies, as may other factors related to the in vitro technique, such as alcohol, glutaraldehyde or formaldehyde fixation, the presence or absence of restorations and soft tissues, or the nonexistent movement of the corpse or skull, all of which can generate changes in the density and architecture of the periodontium at the time of the scan1, 3, 4, 10, 14. However, the position of the skull does not affect the accuracy of the linear measurements2.
This study used the standard specifications provided by the manufacturer: 12 mA, 90 kVp and 14.9-second exposure, according to the scanner user manual13. Misch et al. suggested that in vivo studies should be undertaken as in previous studies that employed 47.7 mA, 120 kVp and a 20-second exposure15; or 98 mA, 120 kVp and a 20-second exposure16. Both studies showed that all alveolar defects (artificially created in vitro) were detected with high precision, although the radiation level was significantly increased. However, other studies used different values, such as: 1-3 mA, 7 mA, 2 mA and for example, 80 kVp and a 17-second exposure, or 0.5 mA, 110 kVp and a 5-7-second exposure, and obtained results with low accuracy and sensitivity12, 17, 18.
In addition, the use of CBCT as a reference standard is not appropriate, since all scanners showed errors in the measurements. The study explains that the lack of soft tissue affects the final image and the presence of tissue generates attenuation coefficients that affect image sharpness.
This study was conducted in periodontally compromised patients. Healthy patients might have longer and thinner cortical bones, which would be even more difficult to detect by CBCT.
The use of CBCT images to measure the vestibular alveolar bone of incisors and premolars provides inaccurate results when using SD resolutions in the Orthophos XG 3D (0.16 mm voxel), since it over estimates the size of dehiscences by an average 3.15 mm. SD CBCT measurements differed significantly from values measured with Vernier caliper.

