











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The root canal system (RCS) has complex internal anatomy, which needs to be clearly understood in order to ensure successful endodontic treatment. Since anatomical variations offer a high degree of technical complexity and may even result in treatment failure, the practitioner should be fully aware of both internal tooth anatomy and anatomical variations observed in daily practice1,2.
Incisors have rectilinear roots, so their anatomy is not considered to be complex, nevertheless, mandibular incisors may present variations such as oval and flattened root canals, as well as a second root canal in 11% to 45% of teeth2.
Several imaging methods have been used to evaluate root canal anatomy, but many of these techniques are time consuming and present certain difficulties such as artifacts and distortion3. Thus, in order to ensure successful root canal treatment, more accurate imaging methods should be used to analyze internal canal morphology 2.
Although computerized microtomography (micro-CT) is not yet available for daily clinical use, it is rapidly gaining popularity for scientific research in the field of dentistry. The micro-CT imaging method has several advantages compared to other methods, mainly because it is fast, reproducible and non-invasive, provides high-quality results which can be viewed in 2D and 3D, and enables simultaneous observations of both internal and external tooth anatomy3.
In this context, the present study aims to evaluate the internal morphology of incisors using computed microtomography (micro-CT) images.
MATERIALS AND METHODS
This study was approved by the Research Ethics Committee of Federal University of Juiz de Fora (approval number 2.754.921). Forty lower central incisors and 49 lower lateral incisors were selected from the Biobank, totaling 89 teeth presenting healthy crowns and closed apices.
After cleaning the external surfaces using ultrasound (ProfiClass, Dabi Atlante Ltda. - Ribeirao Preto, SP, Brazil), the teeth were stored in universal collectors (Farmax - Distribuidora Amaral, Divinópolis, MG, Brazil) and identified. Images were acquired using a SkyScan 1173 microtomograph (Bruker Micro-CT Kontich, Belgium) applying the following parameters: 50Kv, 160 pA, 1mm thickness aluminum filter with 360° rotation, 0.8° rotation step, pixel size 12.11pm, in 2240 x 2240 (small pixel size) camera mode, totaling a scanning time of approximately 28 minutes per specimen. Subsequently, three-dimensional (3D) specimen images were reconstructed using NRecon v1.6.6.0 software (Brucker MicroCT, Kontich, Belgium) and reduction of possible artifacts. This process resulted in an average 794 slices per specimen (range 636 to 918 slices), from the apex to the level of the cemento enamel junction, enabling internal microstructures to be viewed. The reconstructed images were then saved in bitmap format (bmp).
The following quantitative 3D parameters were evaluated: volume, root canal surface area, structure model index (SMI). When the SMI was close to 0, the root canal was considered flat, a value close to 3 was considered cylindrical and a value close to 4 spherical4,5. The following two-dimensional (2D) parameters were assessed: perimeter, root length from cementoenamel junction (CEJ) to the apex and shape of the canal mouth, cervical, middle and apical thirds, circularity, smallest and largest anatomical canal diameter at 1 mm from the apex. The cross sections of the root canals were classified as round, oval or long oval according to the smaller and main canal diameter at 1 mm from the apex6. The 3D analysis plug-in and morphometric analysis tools from CTAn software were used to obtain these measurements. The presence and location of accessory canals and the amount of foramina at 4 mm from the apex were also evaluated.
The following anatomical parameters were evaluated using the CTAn V.1.13 and CTVol v.2.2.1 software (Bruker microCT) in the qualitative analysis: number of root canals, main root canal classification, occurrence and location of lateral root canals7, curvature degree of the main canal8, position of the anatomical foramen in relation to the apex, and presence or absence of apical constriction and its classification, when present9.
The qualitative and quantitative results of the anatomical parameters were presented descriptively, without statistical analyses.
RESULTS
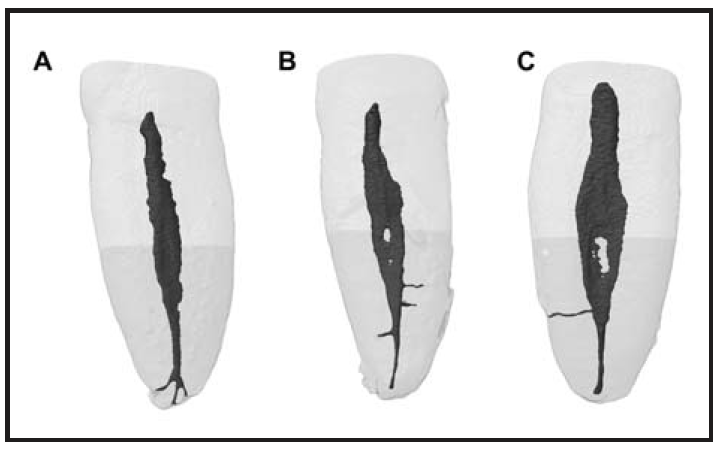
The analysis of 89 human incisors indicated that 89.9% of the canals had a single main root canal and were therefore classified mostly as Vertucci type I canals. Type II (6.7%) and type III (3.4%) conformations were found only in lower central incisors (Fig. 1). Only 5.6% of the specimens presented lateral root canals, 4.5% and 1.1% in the apical and middle third, respectively. However, no lateral root canal was observed in the cervical third. Only 1.1% of the sample presented an apical delta (Fig. 2).
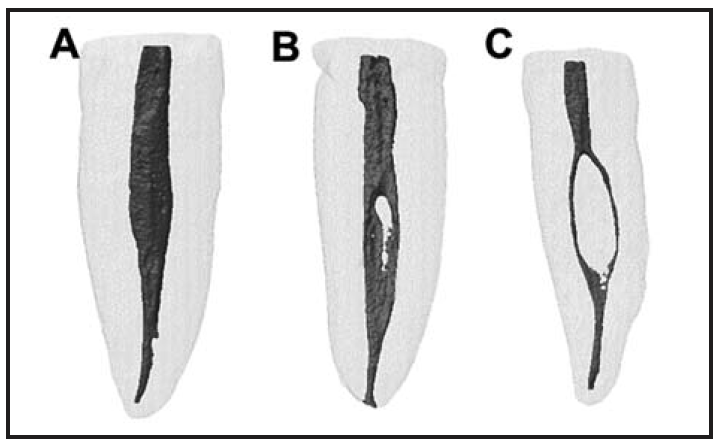
Fig. 1 Representative image of the most common main root canal classifications: A- type I, B- type II and C- type III
Regarding the quantitative three-dimensional parameters, the central incisor canals had mean volume and surface area of 27.31 ± 7.68 mm3 and 82.81 ± 15.04 mm2, respectively. For lateral incisors, average volume was 35.88 ± 11.11 mm3 and average surface area was 97.64 ± 18.83 mm2. The SMI indicated that the root canal geometry of the central and lateral incisors resembled a cylinder, with SMI = 2.12 ± 0.39 and 1.94 + 0.55, respectively.
The two-dimensional analysis results (perimeter, circularity, and largest and smallest diameter) of the central and lateral incisors are shown in Table 1. Root length measured from the pulp chamber to the apical foramen ranged from 11.76 to 20.84 mm (15; 89 ± 1.96mm) and the average number of apical foramina 4mm below the apex was 1.10 ± 0.45. Regarding the shape of the root canal mouths at CEJ level, central incisors had prevalence of circular (58%), followed by oval (20%), "bowling pin" (10%), kidney-shaped (5 %), triangular, fish and hourglass (3% each). In lateral incisors, prevalence was oval (35%), followed by circular (27%), fish and bowling pin (12% each), triangular (6%), kidney-shaped (4%) and hourglass-shaped (2%). (Fig. 3).

DISCUSSION
Knowledge of internal tooth anatomy is paramount for successful endodontic treatment10. In this context, the aim of this study was to analyze the internal morphology of mandibular and maxillary incisors by means of computed microtomography. Several studies have reported the prevalence of a single main root canal (Vertucci Type I) in incisors, ranging from 64% to 100%11-13. In the present study, 89.9% of the samples were classified as Vertucci type I, similar to the results reported by Lin et al.12 The divergences regarding the prevalence of a single root canal in incisors can be explained due to different populations, sample size and the proposed evaluation method, such as the use of diaphanization11, cone beam computed tomography12,13 and computed microtomography1. In addition, unlike in the present study, other assessment articles do not separate central incisors from lateral incisors, which increases the range of anatomical variations compared to the current analysis, which distinguishes between different teeth.
The presence of two separate root canals that join in the apical portion (type II) and a single root canal that divides in the middle third and then joins to form a single outlet root canal (type III) accounted for 6.7% and 3.4%, respectively, in lower central incisors only. These findings may be explained by the fact that a dentin bridge is formed inside the lower incisor pulp, creating two root canals within a single root, which can either merge and terminate in a single apical foramen or remain separate from each other throughout their length10.
Types IV, V, VI, VII and VIII were not observed in the current study, in agreement with previous studies11-13. However, the aforementioned studies indicate the presence of type IV cases - two root canals separated from the crown to the apex - and/ or type V cases - a single root canal that divides to form two root canals in the apical region. The analysis of different populations and the evaluation methodology applied may explain these differences. Root length measured from the pulp chamber to the apical foramen ranged from 11.76 to 20.84 mm, in agreement with the result of a previous study1. The largest and smallest root canal diameter 1mm below the apex contrasts between studies, ranging from 0.13 to 1.49 (largest diameter) and 0.02-0.43 (smallest diameter)1,14,15. In the present study, the largest and smallest diameters in the apical third were, respectively, 0.38 ± 0.19 and 0.21 ± 0.04 for central incisors and 0.52 ± 0.18 and 0.22. ± 0.08 for lateral incisors. These differences between studies may be explained by the fact that anatomical groups were separated in the present study, thereby reducing variations. By grouping upper (larger) incisors with lower (smaller) incisors, average diameter variation tends to increase.
The presence of an accessory canal, a branch that exits the main canal and communicates with the external surface of the root, an apical delta and several apical foramens enables the passage of pulp irrigants to the periodontium16 and, if not properly cleaned, may lead to endodontic treatment failure17. In the present study, only 5.6% of the specimens presented lateral canals, 4.5% and 1.1% in the apical and middle third, respectively, in agreement with findings reported in previous studies1,9,18. No lateral root canal was found in the cervical third of the teeth.
According to a previous study, only 1.1% of the sample had an apical delta, accessory canals were observed only in the apical third, and most of the central (60%) and lateral (74%) incisors had no accessory canals1. The average number of apical foramina 4 mm below the apex was 1.10 mm ± 0.45 mm.
Canals may have different cross-sectional shapes at different levels of the root in the same tooth15. In the present study, 73% of the incisors were classified as oval in the cross section 1mm below the apex. In the root canal mouth at CEJ level, the most prevalent central incisor type was circular (58%), followed by oval (20%), while for the lateral incisors there was prevalence of oval (35%), followed by circular (27%).
According to the literature, mandibular incisors usually have flat and oval canals, and oval canals in this group lead to difficulties and reduce the quality of endodontic treatment2. However, although the cross-sections in the apical third and canal mouth are oval and/or circular, the SMI along the entire canal in the assessed incisors indicates that root canal geometry varies from oval to cylindrical (SMI = 2.02 ± 0.49), facilitating extensive endodontic canal treatment in some in canals with this characteristic. The root canal morphology of anterior teeth is variable and may present additional canals and a variety of canal configurations, as observed herein. The dentist should be aware of possible variations, as they may lead to errors in the attempt to locate root canals and, consequently, endodontic treatment failure.
Although incisors have a single root with relatively simple anatomy, internal anatomical variations may offer a high degree of technical complexity, leading to treatment failure if not well understood by dental professionals.

