











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Although there has been a worldwide reduction in the prevalence, incidence and severity of dental caries among children aged five to twelve years old over the past 30 to 40 years, the disease remains widespread. Untreated cavitated dentine carious lesions are still the most common disease that affects humans worldwide1,2 and, especially in poor communities, children's oral health status remains a challenge yet to be resolved1.
Untreated carious lesions and their clinical consequences are the main cause of pediatric dental pain3,4. Toothache is a complex phenomenon and its occurrence is relatively frequent in dental diseases, resulting in school absenteeism and impairing the child's quality of life5,6. The progression of untreated dental caries to odontogenic infection is the result of lack of public policies and children's lack of access to health services3.
Dental pain measurements enable better assessment of the need for oral health care and foster the establishment of treatment priorities7. The implementation of public health strategies for vulnerable populations is essential, especially in low- and middle-income countries, where caries disease and its related painful episodes continue to be polarized and strongly influenced by the socioeconomic status of the population3.
Even though it is well known that dental sepsis causes biological disorders in children, there are few studies analyzing it effect on children's self-perceived quality of life. Therefore, the present study was designed to assess the prevalence of untreated carious lesions which developed odontogenic infection and to evaluate its association with the subjective variables of quality of life and dental pain among low-income schoolchildren aged eight to ten years.
MATERIALS AND METHODS
Ethical approval
This study was approved by the Ethics Committee of the Federal University of Alagoas (Protocol No. 2.970.527 /18) and conducted in accordance with the World Medical Association Declaration of Helsinki. Consent for undertaking the research was obtained from the school director, all children, and their parents or caregivers. Only students whose parents or caregivers signed a written informed consent were included in the study.
Participants
A cross-sectional study was conducted with children enrolled in a public school in the city of Maceio, Alagoas, located in the Northeast Region of Brazil. Sample size was calculated using an 18.3% prevalence rate from a previous study8, with 95% confidence level and 5% standard error.
Hence, the minimum sample size was defined as 227 schoolchildren.
The public school was chosen randomly, and the students were randomly selected from the school attendance lists. Inclusion criterion was children aged eight to ten years old at the time of the clinical examination. Exclusion criteria were children with physical or mental disability or developmental dental anomalies, in order to avoid incorporation bias.
Oral examinations
Data were collected in a classroom from January to May 2019. The oral survey was performed with children sitting on regular school chairs, under natural light, by a single dentist calibrated for visual examination, following the criteria established by the World Health Organization for dental caries9. The examinations were carried out with the aid of a dental mirror (Golgran®, Sao Paulo, Brazil) and wooden spatula. Tooth surfaces were dried with sterile gauze.
The Kappa coefficient for intra-rater agreement was K = 0.85. Prevalence of dental caries was determined using the DMFT/dmft index. The decayed component (D/d) was used as an indicator of untreated carious teeth. The existence of infection as a consequence of untreated dental caries were evaluated using the PUFA/pufa index10, K = 0.84. The PUFA/pufa score per person was calculated in the same cumulative way as the DMFT/dmft. The PUFA for permanent teeth and pufa for primary dentition were reported separately. A combination of the decayed component and PUFA/pufa score was applied to measure the severity of untreated dental caries. Thus, the untreated caries-pufa ratio was calculated using the following equation, providing the percentage of teeth with untreated caries that developed odontogenic infection10.
Quality of life questionnaire (CPQ8-10)
After the clinical survey, children were invited to respond individually to an interview performed by a trained examiner. The independent variable of this study was children's oral health-related quality of life (OHRQoL), assessed using the Child
Perceptions Questionnaire (CPQ8-10)n, validated to Brazilian Portuguese by Martins et al.12. The interview script involved information on the child's name, age and sex, followed by the OHRQoL instrument.
The questionnaire contains 25 items arranged into four subscales: oral symptoms (n = 5), functional limitations (n = 5), emotional well-being (n = 5) and social welfare (n = 10). The responses are graded on a five-point Likert scale as: "never" (score = zero); "once or twice" (score = one); "sometimes" (score = two); "often" (score = three); and "every day or almost every day" (score = four). The scores for all questions were added to provide the overall CPQ8-10, with possible values ranging from zero to 100. The scores for each domain were also calculated. Higher scores evidenced a greater negative impact on OHRQoL8.
Dental pain measurement
The experience of dental pain was evaluated in four aspects: presence, frequency, duration and intensity, the latter by means of a verbal scale and a visual analogue scale (VAS).
The child was asked whether he/she had ever had toothache, and the answer categorized as present/ absent. Frequency was recorded as the recurrence of painful events during the week, and duration was assessed as the period presenting painful episodes. To analyze intensity, the child was asked to describe the dental pain using the verbal scale responses: "mild" (score = zero), "uncomfortable" (score = one), "stressful" (score = two), "horrible" (score = three) and "intolerable" (score = four). At this point, the child was shown a numerical/VAS tool to register the severity of the disease-related symptom on a scale from zero to ten.
Data analysis
After data collection and variables categorization, a database was created for statistical analysis using SPSS (Statistical Package for Social Sciences), version 23. Normal data distribution was verified by applying the Kolmogorov-Smirnov test. To test the association between variables, Mann-Whitney or Kruskal-Wallis test was used with post-test by Dunn's nonparametric comparison. The correlation between the impact on quality of life and aspects of dental pain was determined by Pearson's correlation test. The error margin used in the decisions of the statistical tests was 5%, with intervals at a 95% confidence level.
RESULTS
Two hundred and thirty children were surveyed. Mean age was 9±0.85 and 53.5% were male. Average dental decay was 2.59±2.59, and 74.3% (n = 171) of the children had cavitated carious lesions. The filling (F/f) component of DMFT/dmft was 0.20±0.806, showing that 91.7% of the evaluated children had not had any teeth restored.
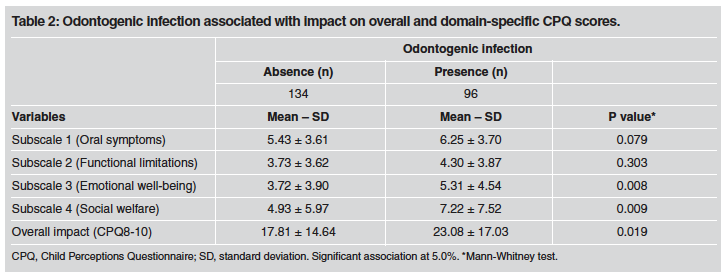
Of the surveyed children, 42.6% (n = 98) had odontogenic infection and the large majority (80%; n = 184) reported having had dental pain sometimes. Table 1 shows the association between odontogenic infection and sex (p = 0.558), age (p = 0.034) and past experience of toothache (p < 0.002). Among the self-reported quality of life variables analyzed, the presence of odontogenic infection was significantly associated with the child's emotional well-being (p = 0.008), social welfare (p = 0.009) and overall impact on quality of life (p = 0.019). (Table 2).

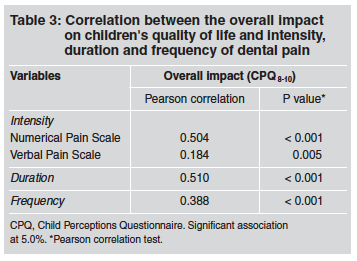
Using the verbal scale of pain responses, children reported the intensity of painful episodes as "horrible" (24.3%; n = 56), "mild" (18.3%; n = 42), "uncomfortable" (18.7%; n = 43), "stressful" (14.8%; n = 34) and "intolerable" (5.7%; n = 13). The mean score on the numerical pain scale was 5.17±3.63. Table 3 shows the correlation between the overall impact on children's quality of life and toothache intensity assessed by the verbal pain scale (r = 0.184; p = 0.005) and numerical scale of pain (r = 0.504; p < 0.001), toothache duration (p < 0.001) and frequency (p < 0.001).
DISCUSSION
Most orofacial infections are believed to have odontogenic origin, in which untreated dental caries plays a major role. The occurrence of dental decay has a contextual nature, in addition to its infectious progression13,14. The present school-based crosssectional survey evaluated the prevalence of odontogenic infection and its relation with children's OHRQoL and dental pain. It was observed that children's age and experience of dental pain were associated with the occurrence of dental sepsis, impacting negatively on their quality of life.
Of the evaluated children, 42.6% had odontogenic infection. The prevalence of infectious process in schoolchildren reported in the literature ranges from 7.1% to 85%15-21. These widely differing results are believed to result from differences in the diagnostic methods used by the examiners, study design and population surveyed. It is still important to emphasize that the prevalence of dental infection may be underestimated since the manifestation of dental abscesses might be episodic. Our study found no significant association between odontogenic infection and sex. In contrast, previous studies demonstrated an association between these two variables, arguing that odontogenic infection and tooth decay are significantly higher in boys17,21.
The child's age was found to be associated with the occurrence of odontogenic infection, with prevalence and severity of dental infectious process increasing with age. This might be explained by the early complete formation of the primary dental arches and consequently, their longer exposure time to cariogenic diet in the dynamic oral environment. The long time elapsed between the tooth eruption and examination may enable the development of extensive carious lesions that may lead to odontogenic sepsis21. Family beliefs and attitudes are determinant factors in children's oral health status, possibly placing them at risk for disease. Parent's past adverse experiences during dental treatment and the fact that they do not value deciduous teeth potentially lead to the lack of care for caries prevention in their children's primary dentition, enabling pathology to advance as teeth mature22,23. Nevertheless, from a biomedical perspective, nobody should have odontogenic sepsis20.
The dental infectious process revealed an association with the past experience of dental pain among the surveyed children, of whom 80% reported having felt dental pain at some time in their lives. The prevalence of toothache reported in previous papers varies widely, ranging from 16.5% to 60%3-6,15,18,24. However, it should be noted that there were differences among these studies in the manner of assessing and measuring painful episodes, such as sample size, age surveyed and time elapsed since toothache.
In our study, the child's emotional well-being and social welfare were associated with the occurrence of odontogenic infection. Schoolchildren's emotions and social coexistence are still maturing and clearly affect their self-concept and self-esteem. These psychosocial variables have been shown to interfere in oral health behavior, determining clinical oral conditions25,26. Similarly, the incidence of dental decay and toothache impair children's individual and social confidence, disturbing their educational performance and social interactions, thereby leading to a chain of circumstances6,15,27,28. Poor access to oral health services in socioeconomically disadvantaged groups can lead to the progression of the untreated disease, trapping children in a vicious circle with evident disturbances in their emotional and biological well-being, such as deficient development and growth, odontogenic sepsis and pain3,5,13,16.
The domains of functional limitations and oral symptoms were not associated with odontogenic infection. This suggests that the infectious process analyzed may not have occurred at a time close to the time of examination (memory bias), and may also be related to the following: (1) the sensation of pain is inherently peculiar and private for children, manifesting as an essentially subjective multifactorial event; (2) as the pediatric infection can rapidly become chronic, it may produce unperceived painful sensation and this could also be related to the child's cognition level; and (3) the special anatomical and physiological characteristics of children's bones allow the suppurative complications of pulp infection diffuse more rapidly than in adults7,14,29. However, the current study found that the overall self-reported impairment of children's quality of life was associated with odontogenic infection.
It is interesting to note that painful episodes in pediatric patients include the interaction of psychological, physiological and developmental circumstances. In this context, we verified a strong correlation between the numerical/visual analogue scale (VAS) format and self-reported impact on children's quality of life, whilst the verbal pain scale demonstrated low association. The greater effectiveness of the numerical/VAS tool as a measurement of toothache intensity may be due to the age of the children in the group surveyed. The psychometric scale may have achieved more accurate responses than the verbal model, because the latter requires certain cognitive and linguistic development7. Toothache frequency and duration were also associated with the overall impact on children's quality of life, with relation to disturbances in psychological well-being, mood, self-perception and school environment caused by intense dental pain30, possibly inducing school absenteeism6. Studies on the effect of odontogenic infection and its related pain on psychosocial elements of children are scarce, even though they would provide significant understanding of the population evaluated and its interaction with social aspects. Although the present cross-sectional survey suggests that dental sepsis and painful symptoms have a direct influence on determinants of quality of life in children, further studies are still needed to identify cause-effect determinants. This survey also shows that previous approaches to public health services have not been successful or did not even reach the examined children, thus reinforcing the assumption that disparities in socioeconomic and environmental levels still affect the incidence of odontogenic infection and toothache among schoolchildren. Restructuring public health policies and designing community-based dental services should be desirable targets in order to reduce the persistent inequalities in children's access to health and pain relief.

