











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Supragingival plaque removal is undeniably the best way to ensure better oral health in the population. It has been proven to prevent caries, periodontal diseases and tooth loss and, more recently, to improve the outcome of dental implants 1, 3.
Oral hygiene routine demands time, dexterity and motivation. Therefore, the limits of the clinical effectiveness of self-performed oral hygiene are evident. Some studies have demonstrated the presence of remaining biofilm despite efforts to remove dental plaque2,4. The new classification of periodontal diseases and conditions established 10% as maximum number of bleeding sites for patients to be classified as healthy, which is achieved with good oral hygiene habits3,5. Some studies have investigated the use of oral hygiene products, showing that there has been an increase worldwide. For example, while in Brazil in the 1990s, less than one toothbrush per capita was used per year4,6, this use had virtually doubled by 20105,7. However, the estimation of use of oral hygiene products does not necessarily imply better clinical results in effectiveness of plaque control. Toothbrushes are the gold standard product used to remove plaque from teeth. They differ in texture, tip, hardness, and even in their material, which may be natural or synthetic. The literature contains few studies comparing the efficacy of available toothbrushes. The use of a soft-bristle toothbrush has been recommended to improve plaque reduction while minimizing gingival tissue lesions8,9. Studies comparing the efficacy of available products are therefore important to better support the indication of any given toothbrush.
The aim of the present examiner-blind randomized controlled clinical study was to compare the efficacy two soft-bristle toothbrushes in terms of plaque removal with regular fluoride toothpaste in controlling established dental plaque over a 7-day period.
MATERIALS AND METHODS
Study Design
This study was designed as a phase III randomized, single-center, two-cell, examiner-blind, parallelgroup clinical study.
Ethical Considerations
The protocol was approved by the Institutional Review Board of the Federal University of Rio
Grande do Sul, Brazil and all the volunteers signed an informed consent form. The study was conducted according to good clinical practice standards 10.
Sample Size Estimate
Sample size was estimated after a pilot study. Based on the standard deviation for the response measures of 0.58, a significance level of a=0.05 and 80% level of power, the present study was powered to detect a minimal statistically significant difference between study group means of 15%, and 32 individuals per group were considered necessary. A 10% possible attrition rate was added. Thus, 35 individuals per group were considered for participation.
Participants
Seventy healthy male and female individuals, aged 21-70 years, were enrolled. Recruitment was performed at the Federal University of Rio Grande do Sul, Brazil. The following inclusion criteria were used: good oral health; initial mean plaque index of at least 0.6, determined by the Improved Plaque Identification Index6,11; and >20 natural uncrowned teeth, excluding third molars. Individuals were not included in the study if they had orthodontic bands, removable partial dentures, tumor or significant pathology in the soft or hard tissues of the oral cavity, moderate or advanced periodontal disease (purulent exudate, tooth mobility, and/or extensive loss of periodontal attachment or alveolar bone), antibiotic use in the month prior to entering the study, participation in any other clinical study, pregnant or breast-feeding status, dental prophylaxis in the 2 weeks prior to the baseline examination, history of allergy to oral/personal care consumer products or their ingredients, use of any prescription medicine that might interfere with the study outcome, medical condition preventing abstinence form eating/drinking/chewing gum for 4 hours prior to the scheduled visit, and history of alcohol or drug abuse.
Experimental Procedures
Participants were instructed to refrain from any oral hygiene measure for 12 hours before reporting to the clinical site, and from eating, drinking or smoking for 4 hours. The baseline examination comprised evaluation of the oral cavity soft tissue and perioral region followed by plaque disclosure with 10ml of 0.04% basic fuchsine solution (Replasul; Iodontosul, Porto Alegre - RS, Brazil). On Day 0, plaque examination was performed using the Improved Plaque Identification Index before toothbrushing 11. Supragingival plaque was assessed on the facial and lingual surfaces of each tooth. Scores of 0 to 4 were assigned to all disclosed surfaces of the maxillary and mandibular teeth using a dental light and dental mirror. Teeth were divided into nine units (Fig. 1, A-I). From these site-wise scores, a whole-mouth plaque score was determined for each participant by calculating the proportion of sites in the mouth at which plaque was present. Three areas are near the gingival margin, two are interproximal, and four are on the body of the tooth. This index enables stratification of area(s) that are of concern during the analysis.

Simple randomization was performed by a computergenerated list by an external researcher responsible for allocation concealment. Toothbrushes were kept inside numbered opaque plastic bags. The experimental groups were:
Group A. A soft-bristle, tapered-tip toothbrush Group B. A soft-bristle, end-rounded toothbrush.
All participants were instructed to brush their teeth for one minute under supervision with the assigned toothbrush and a commercially available standard fluoride toothpaste (Colgate Cavity Protection; Colgate, Sao Paulo, Brazil), after which plaque was evaluated (Day 0 after toothbrushing). They were instructed to use the product at home twice daily (morning and evening) for the next 7 days and to refrain from any interproximal cleaning. On day 7, all participants returned to the clinical facility and the procedures performed on Day 0 were repeated. The same examiner (CKR), who was unaware of group allocation, performed all plaque examinations.
Statistical Analysis
The main study outcome is plaque score reduction, determined by the Improved Plaque Identification Index. Plaque Index was dichotomized into absence of dental plaque (scores 0 or 1) and presence of dental plaque (scores 2, 3 or 4). The percentage of sites with presence of dental plaque was calculated for each individual for both experimental periods (Day 0 and Day 7). The percentage reductions of plaque before and after toothbrushing were calculated for each experimental period as follows: percent of dental plaque after toothbrushing x 100 / percent of dental plaque before toothbrushing.
Separate statistical analyses were performed for whole-mouth, interproximal, and gumline plaque scores. A per-protocol analytical approach was used. The statistician was blinded to participants' product allocation. Percentage reductions between before toothbrushing and after toothbrushing were calculated for both Day 0 and Day 7 for whole-mouth, interproximal and gumline regions. Comparisons between groups were performed using the Mann-Whitney test, as a non-parametrical data distribution was observed (Kolmogorov-Smirnov test showed a p-value <0.05).
Non-parametrical distribution was also identified for the number of present teeth, so the Mann-Whitney test was used to compare the number of teeth between groups. Age was compared between groups by t-test for independent samples. Categorical data (sex and smoking exposure) were compared between groups by chi-square test. A significance level of a=0.05 was established for all analyses. Data analysis was performed using the statistical package SPSS 21.0 (SPSS Inc., Chicago, USA).
RESULTS
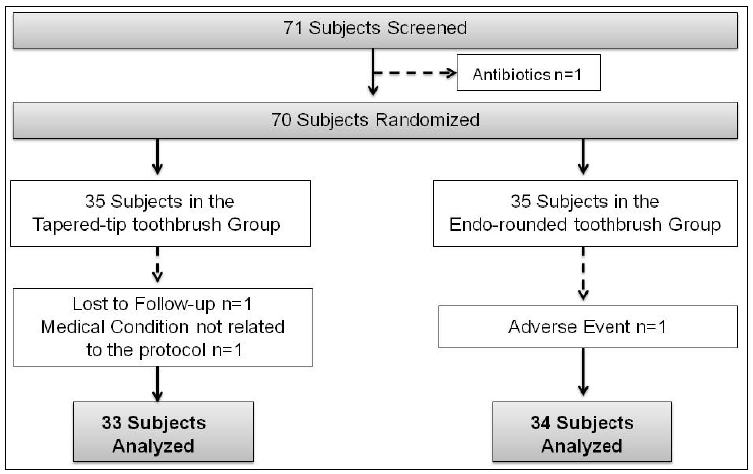
One individual of the 71 initially screened for the study was not included (Fig. 2). Out of the 70 included participants, 67 completed the 7-day clinical trial. Three participants - 2 in Group A and 1 in Group B did not complete the study. Reasons for dropouts are mentioned in Fig. 2). Groups did not differ in gender or mean age (Table 1).

With relation to scores on Day 0 before toothbrushing, a statistically significant difference between groups was detected (P<0.001) (Table 1), and therefore the present study analyzes percent reductions rather than means. Fig. 3 shows the mean percent reduction (from before toothbrushing to after toothbrushing) on Day 0, considering the whole-mouth, interproximal and gumline and surfaces. Group A showed significantly greater reduction in mean whole-mouth (21.39±12.44%), interproximal (10.82±10.49%) and gumline (6.32±7.37%) plaque scores compared to Group B, in which reductions were 11.4±11.17%, 5.21±7.68% and 2.89±4.57%, respectively (Fig. 3).
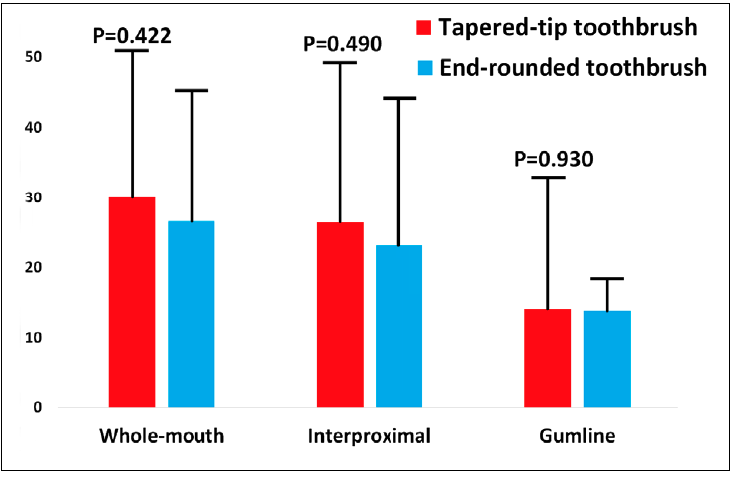
Fig. 3 Mean percent reduction of plaque for Group A (ta-pered-tip toothbrush) and Group B (end-rounded toothbrush) on Day 0.
In the Day 7 follow-up, a statistically significant difference was observed in the scores before toothbrushing (P<0.007) (Table 1) in whole-mouth surfaces. Participants in Group A showed no significant difference in the whole-mouth (29.94±20.91%), interproximal (26.41±22.77%) or gumline (14.04±18.82) percent reduction of plaque scores when compared to Group B, which had 26.58±18.64%, 23.12±20.98% and 13.78±17.63, respectively. However, no statistically significant difference was observed in mean percent reduction of plaque ( Fig. 4).
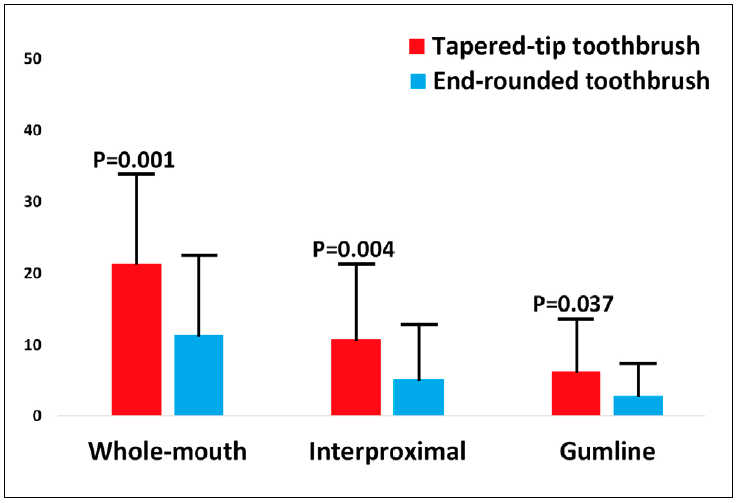
Fig. 4 Mean percent reduction of plaque for Group A (ta-pered-tip toothbrush) and Group B (end-rounded toothbrush) on day-7.
Three adverse events possibly related to the study were reported during the 7-day study: traumatic brushing, mouth ulcers and severe pain in teeth irradiating to ear and jaw as reported by the subjects. All three (3) adverse events were reported in Group B and one individual preferred not to continue in the study due to the discomfort. All participants who reported adverse events were carefully followed until the issue was resolved. As toothbrushing technique may explain these findings, all individuals received individualized oral hygiene instruction after all experimental periods were completed.
DISCUSSION
The present study was designed as a phase III randomized, single-center, two-cell, examinerblind, parallel-group clinical study, with the aim of comparing the plaque removal efficacy of two soft-bristle toothbrushes in 70 healthy volunteers. Plaque reduction was greater in Group A (taperedtip toothbrush) than in Group B (end-rounded toothbrush) in the first usage. This result was statistically significant in the percent reduction on Day 0 but was not significant on Day 7. Toothbrushing is known to be the most frequently used method of oral hygiene. The contemporary paradigm of oral hygiene is based on the highest efficacy with the least harm. In order to increase effectiveness and reduce the effects of improper brushing techniques, manufactures set the goal of evolving their toothbrushes in terms of design and bristle characteristics. It is well known that soft-bristle toothbrushes are efficacious and have less harmful potential8,9. Different toothbrushes have been developed with the aim of achieving better cleaning effect in the whole mouth, regardless of the type of movements used by the user12,13. A variety of studies can be found in the literature regarding different toothbrush designs and morphologies. It is not easy to compare the different studies, particularly due to high variety in design, follow-up, brands used, etc. The findings of such studies are important as different types of toothbrushes are launched on the market and there is constant need of support from sound studies in terms of efficacy and safety.
The present study was designed to compare the effect of a novel soft-bristle toothbrush (Group A) with a toothbrush that is already well established on the market (Group B). It should be emphasized that even though both brushes are considered soft, the brush being tested in the study (Group A) has softer bristles. Although it is well known that softer bristles can be less efficacious 14, there is no doubt about the benefit of their being less harmful 8. This is not a double-blind study, since the participants received different toothbrushes. However, all additional procedures were identical for both groups. The study was designed as an efficacy study, which demonstrates the potential of a novel device. Even though initial plaque scores were numerically similar, they differed significantly between groups, so in order to normalize data, the present study analyzes percent reduction in plaque scores. The results showed that Group A presented higher efficacy in reducing whole-mouth and interproximal plaque on Day 0 (which was the first contact with the brushes), even though the bristles were softer. The results after 7 days did not present a statistically significant difference. The separate analyses performed in his study are important because they consider the ability of the different types of toothbrushes to act on specific parts of the teeth. Their ability to remove plaque from interproximal areas, where other devices (such as dental floss) present limitations, is of special interest in terms of occurrence of dental caries, gingivitis and periodontitis.
Plaque was measured using the Improved Plaque Identification Index 11, which was designed to quantify the presence of dental plaque in each of the 9 regions identified on teeth by the Navy Plaque Index. The Improved Plaque Identification Index could be more sensitive and provide more accurate demonstration of differences in plaque levels. However, this kind of quantification tends to generate regression to the mean, so we dichotomized the index to facilitate clinical interpretation. The results showed higher efficacy in Group A upon the first usage. The leveling of the results on Day 7 might be explained in part by the Hawthorne effect, since participant behavior may be expected to change in response to awareness of being observed 15. In addition, the effect of a learning curve should not be disregarded.
Tapered bristle toothbrushes have been tested and shown to be more effective in reaching not only interproximal areas of the teeth along the gingival margin and under gumline, where plaque accumulates the most, but also to reach fissures, when compared to end-rounded bristles. This result was also positive in an in vitro study with artificial plaque in which tapered-tip bristles have demonstrated significantly better results in reducing plaque scores in the interproximal area 16. The use of tapered-tip bristle toothbrushes could benefit patients who do not include flossing in their daily hygiene routine, as it was shown in an updated review 17 that flossing did not necessarily reduce dental caries and periodontal disease.
As in the study by Rösing et al. 2016 18, a 12-hour period established to refrain from any type of oral hygiene before both evaluations showed that plaque accumulation was sufficient to test the efficacy of the toothbrushes, although it was significantly different before toothbrushing Day 0 in Group A. It should be noted that no brushing technique was imposed on the participants, in order to highlight the outcome of their real daily brushing techniques.
Three adverse events were reported in the present study, none of which was related to the study protocol. Most of the reported adverse events could be explained by causes related to patients' brushing habits. One of the participants was excluded. It is also important to highlight that soft and extra-soft bristle toothbrushes have been reported in a systematic review to be safer than other toothbrush stiffness when oral injuries are evaluated, with tapered or rounded bristle end-shape 8 presenting no clinical relevance concerning soft oral tissue damage. Participants were asked to brush their teeth for one (1) minute. Many studies have used the same brushing time, the main reason being to avoid the patient needing to brush excessively18-20. Moreover, it has been demonstrated that patients do not spend longer than one minute on toothbrushing in general. This study has strengths and limitations that should be noted. Among the strengths are the study design, with randomization of the participants, use of a standardized brushing time, examiner reproducibility, examiner and statistician blinding, and very high compliance rate. The limitation of the study is the efficacy design, in which a short time (7 days) was used. Neither effectiveness nor effect on gingival inflammation can be ascertained from our results.
Despite the abovementioned limitations, it should be noted that there were better interproximal results in Group A, which may be relevant, considering that toothbrushes were not meant to reach this area. Other studies have demonstrated similar results with tapered-tip toothbrushes18-20. It is important to remember that a systematic review published by the Cochrane collaboration and revisited in 2019 showed concerning results regarding the levels of periodontal disease and caries in dental floss users, concluding that dental floss users do not necessarily have less diseases 17. Thus, it is always important to study newly designed toothbrushes, especially as a possibility of compensating for the limited effects of flossing, according to how they are used. Longer term randomized controlled trials are warranted, including the analysis of adverse events, in order to prevent gingival tissue harm.
The tapered-tip toothbrush performed better than the end-rounded toothbrush in terms of efficacy at the first evaluation.

