











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Skeletal anchorage has been widely used in orthodontics because it does not allow movement of the reaction unit, providing satisfactory results for anchorage control with less discomfort to the patient 1 . To be considered ideal, a skeletal anchorage system must have certain characteristics, such as easy installation, resistance to orthodontic forces, simple removal, small size, and being ready for early activation to minimize treatment time and maximize efficiency 2 .
According to the literature, among the means for achieving skeletal anchorage, the orthodontic miniscrew technique has shown the most significant clinical applicability compared to other skeletal anchorage systems such as integrated bone implants or mini-plates 3 .
Orthodontic mini-screws have distinct shapes and sizes. Most of them are manufactured in titanium alloy grade V (Ti-6Al-4V) specified by the ASTM F136 standard 4 . Skeletal anchorage can also be achieved using AISI 316L Austenitic stainless steel 5 Skeletal anchorage can be interradicular or extraalveolar. In interradicular anchorage, mini-screw insertion requires positioning guides with local radiographs and correct root inclination. Direct insertion, on a site with low bone thickness, should be performed avoiding inclination movements 6 .
In extra-alveolar anchorage, mini-screws are inserted into a great bone thickness. Inclination and torsions movements are usually necessary to avoid contact with dental roots. Extra-alveolar anchorage has been widely used because it is efficient in the treatment of certain deformities, especially for retractions of the entire upper or lower dentoalveolar complex 7 . However, mini-screws must be used adequately, considering the loads involved and their mechanical properties and structural resistance 8 . It is therefore essential to know the magnitude of the torques involved, and local anatomical structures. Gingival tissue and bone density must be taken into account as factors that can influence the installation of anchorage 9 . Professional experience is important at the time of selecting and using mini-screws, to minimize mini-screw losses and iatrogenic injury. Dental surgeons still have doubts about which miniscrew system to use, due to the high use of titanium, mainly in extra-alveolar anchorage, which requires a significant level of torque and angulation to avoid root contact.
The aim of this study was to test the structural strength of mini-screws of different brands using an in vitro model. Pig mandibules were used to test the ability of mini-screws to withstand insertion/removal torques without suffering deformation or fracture during the extra-alveolar insertion procedure.
MATERIALS AND METHODS
Fourty orthodontic mini-screws with the same diameters and lengths were used: 20 made of stainless steel (OBS Bomei/Taiwan, 2.0mm in length, 12 mm diameter (Gold standard) and 20 made oftitanium OBS Bomei/Taiwan (2.0 x 12 mm). We also tested another 40 titanium mini-screws of two popular Brazilian brands: 20 Morelli/Brazil (1.5 x 10 mm) and 20 Neodent/Brazil (1.6 x 11 mm), in the largest diameters and lengths available, but with smaller diameter and lengths than gold standard. We evaluate their capabilities in extra-alveolar inserts, since they are designed and manufactured for interradicular insertion. Fig. 1 shows the geometry of the tested mini-screws, and Table 1 shows the main characteristics of the mini-screws used in the extra-alveolar insertion tests.

Fig. 1 Geometric configuration of the mini-screws used in the tests. 1: MPO Bomei Titanium; 2: MPO Bomei Stainless Steel; 3: MPO Morelli Titanium; 4: MPO Neodent Titanium.

Experimental Setup for Extra-Alveolar Anchorage Tests
Extra-alveolar anchorage was simulated in the region of the buccal shelf with great bone thickness in pig mandibles. The density and bone metabolism of pig mandible are similar to those of human bones10, which makes them compatible for in vitro analysis. Eighty fresh mandible semi-arches of adult pigs with approximate weight and size were obtained from a slaughterhouse (Frigorífico Sao Pedro-Uberlandia/ MG-Brasil). During the procedures the mandibles were stored in a refrigerator at 6°C to 10°C.
A reference system (positioners made of 0.17” x 0.25” stainless steel wires) was used for positioning the angles (30° and 60°) during the insertion procedure (Figure 2a, 2b, 2c). Positioners were fixed between the selected molars to guide the initiation of the process with the appropriate inclination.

Fig. 2 Positioners made of 0.17" x 0.25" stainless steel wires a) 30°, b) 60°, c) in position between molars.
The pig mandibles were fixed in a vice supported on a bench. A single experienced surgeon inserted the mini-screws at the mucogingival junction in the posterior region between the 1st and 2nd molars, into the external oblique line (buccal shelf), using the insertion tools provided by each manufacturer. Two insertion procedures were carried out:
- Direct insertion at 30°: The mini-screws were positioned at 30° relative to the long tooth axis and inserted in this position up to the end of the thread or beginning of the transmucosal profile (Fig.3a). Ten direct insertion procedures were performed at 30° for each type of screw tested.
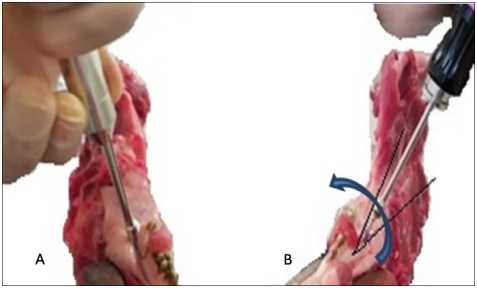
- Indirect insertion at 60° positioning, ending at 30°: This procedure begins by positioning the mini-screws initially at 60° in relation to the long tooth axis (Fig. 3b). After inserting approximately 2 mm, the mini-screws are gradually inclined to the 30° position, while inserting up to the end of thread or beginning of the transmucosal profile, according to the extra-alveolar technique recommended by Chang7. Thereby, there is a gradual bending effect on the mini-screw during the insertion process. Ten indirect insertion procedures were performed at 60° for each type of screw tested.
The mini-screws were then removed from the mandibles by the same surgeon using the same tool as for the insertions.
Optical Microscopy and Scanning Electronic Microscopy (SEM)
Mini-screw strain was analyzed using a CLS 100 Leica optical microscope at magnifications of 1.0, 1.6, 2.5 and 4.0 X, considering head, transmucosal profile, thread and tip.
Strain was then accurately analyzed using scanning electron microscopy of the samples which were mounted on aluminum bases with double-sided carbon tape, in an EVO model MA 10 (Zeiss, Germany) in the high vacuum range. Photomicrographs at 28x magnification of the head, transmucosal portion and thread portion of the miniscrews were used
Statistical analysis
Strain was evaluated only as present or absent, since any level of strain that occurred could compromise the quality of extra-alveolar anchorage. Each type of mini-screw was compared to controls without strain considering the regions analyzed. Deformed and undeformed mini-screws were counted to evaluate the level of structural resistance.
Score 0 (zero) was assigned to mini-screws which remained intact and score 1 (one) for mini-screws which suffered any strain or fracture. This procedure was used because from a structural standpoint, any level of strain could lead to early failure of the mini-screw or change the stabilization conditions expected in an extra-alveolar anchorage process. Gold standard 2.0 x 12 mm stainless steel miniscrews recommended in the Chang technique7 were compared to titanium alloy mini-screws of the same diameter and length, both made by the same manufacturer (Bomei-Taiwan). Two other titanium mini-screws manufactured by Morelli-Brazil (1.5 x 10mm) and Neodent-Brazil (1.6 x 11mm), which were smaller in diameter and length, were also evaluated.
The Kruskal-Wallis non-parametric test was applied. After confirming statistical differences, the Tamhane post hoc test was used to reduce statistical errors and to determine which pairs presented significant statistical differences (p< 0.05).
RESULTS
Figs. 4 and 5 show the strain and fractures in the mini-screws evaluated by SEM microscopy. The steel mini-screws did not suffer deformations during the direct insertion process at 30o, showing the greater resistance in this type of fixation.

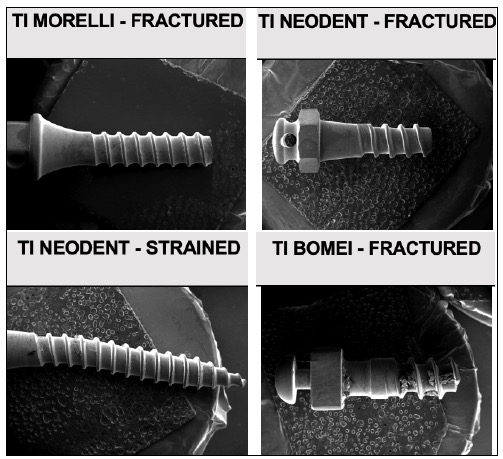
Taken as a whole, the number of strained titanium mini-screws was high among those subjected to direct insertion, and even higher in those subjected to indirect insertion. Statistically significant difference was found between percentages of strained and nonstrained groups. (Fig 6 and Table 2).

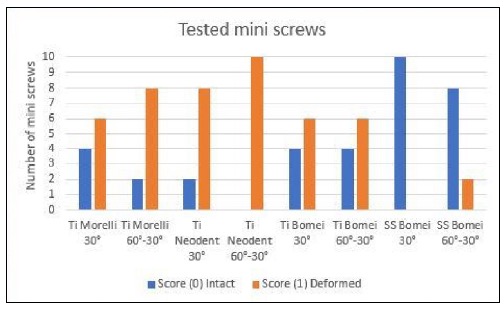
Evaluation of strain generated by direct insertion showed that the structural condition was better in stainless steel mini-screws than in titanium miniscrews (Table 3).

With Indirect insertion no statistically significant difference was found between the stainless steel and titanium mini-screws (2.0 x 12 mm), which both showed some deformations.
Contrary to expectations, the longer and larger diameter mini-screws (2.0 x 12 mm) suffered fewer alterations than those of shorter and larger diameters (1.5 x 10 mm and 1.6 x 11 mm), with both insertion procedures.
DISCUSSION
The aim of this study was to evaluate the performance of Morelli/Brazil mini-screws (Ti 1.5 x10mm) and Neodent/Brazil mini-screws (Ti 1.6 x11mm) in extra-alveolar insertion and to test and compare the structural resistance of two selected OBS Bomei/ Taiwan mini-screws, Ti 2.0 x12mm and SS 2.0 x12mm, the latter recommended by Chris Chang 7 , who was a precursor of the extra-alveolar insertion technique.
Pig mandibles used as a model for extra-alveolar skeletal anchorage were chosen because their bone density and metabolism are similar to those of human bone 10 .
We propose to evaluate the outcome of direct and indirect insertion with different mini-screws, to determine how suitable they are for this procedure and to reduce the risks of early failure. When extraalveolar anchorage is used in orthodontic treatment, several factors should be considered for the choice of the mini-screws, such as the bone thickness of the insertion site, the alloy, the diameter and length and the angle of insertion, and whether to use a direct or indirect process 11-14 .
The insertion sites in thick cortical bone, requires high torques for insertion and removal 15 . Appropriate bone density and thickness are critical for the success of the mini-screws 16-18 to ensure the greater stability 19-21 and higher torques 22 .
Since torque magnitude, for insertion and removal of orthodontic mini-screws, depends on cortical bone thickness 23 , 24 , areas with greater bone thickness should be selected in order to achieve better stability 25 . However, torque should not be excessive, since higher levels may cause bone tissue damage and necrosis, as well as fractures or strains in the mini-screws, thus compromising stability.
Among the longest and largerst diameter miniscrews, only 35% suffered alterations, while 80% of the shorter and smaller diameter screws showed deformation or fracture. Awareness of the insertion site is therefore important, since bone density and thickness are essential factors for instability and increase of torques.
The mechanical properties of materials are also essential for greater safety against failure of mini-screws 26 27, . The chosen material must have sufficient mechanical strength to withstand stresses due to the effect of torsion and bending on the threads during placement and clinical removal, without permanent strain 28 , 5 . Most orthodontic mini-screws for anchorage are manufactured from titanium alloys or stainless steel. They both meet the biomechanical requirements for anchorage 29 . However, stainless steel mini-screws have proven to be more resistant to failure than titanium 30 , 31 .
In thicker corticals, it was observed that insertion and removal torque are greater for titanium miniscrews than for stainless steel mini-screws. Fracture resistance, measured by maximum fracture torque, was higher in stainless steel mini-screws than in titanium mini-screws, showing that the insertion process is safer with the use of stainless steel mini-screws4. Stainless steel has better mechanical properties considering the effects of bending, because of its greater ductility. The torsional resistance of stainless steel provides greater sensitivity to the professional during insertion, thereby minimizing the risk of fracture. Titanium mini-screws do not provide tactile response during insertion, so it is difficult for professionals to notice when the rupture is about to occur 29 . Thus, ductility is a very important property because in extra-alveolar anchorage, the mini-screws will almost always require tilt adjustments, even when the insertions are made directly at 30°, as shown in this study.
The comparison of mini-screws of the same diameter and length showed that the mini-screws made of stainless steel alloy performed better than the mini-screws made of titanium alloy for the direct insertions at 30°. For indirect insertion, from 60° to 30°, deformations were observed in both alloys, demonstrating that the angular changes interfere in the structure of both titanium and stainless steel mini-screws. In the evaluation of the performance of mini-screws with smaller diameters and lengths, in both insertions procedures the deformations were large, being greater in the 60° to 30° insertions, also demonstrating that changes of angulation should be avoided if possible, thereby improving performance and decreasing failure rates.
Regarding the diameter and length of the miniscrews, they are factors that also affect the stability. The larger the mini-screws, the greater the insertion and pulling forces 32 , 33 . Greater lengths offer greater resistance to the pullout test, which presupposes greater primary stability 34 . Greater diameters influence the insertion torque 35 . The mini-screws with the largest diameter show greater strength36-38. Therefore, an increase in mini-screw diameter can efficiently reinforce the initial stability, and the insertion torque increases with the increasing diameter and length 39 , 40 .
The results of our study are in accordance with the literature, because it was observed that the different diameters (1.5; 1.6; 2.0 mm) and lengths (10; 11; 12 mm) correlate with performance, evaluated in terms of number of strained mini-screws.
The results of this study could help orthodontists in choosing mini-screws for extra-alveolar anchoring, which can be performed using direct (30°) or indirect insertion (starting at 60° and ending gradually at 30°, with continuous tightening and inclination of the mini-screws).
It is advisable to use mini-screws for extra-alveolar anchorage, but attention should be given to bone thickness, the diameter and length of the miniscrews, the type of alloy and its ability to flex, and especially to changes in the angle during insertions, in order to reduce failure rates and ensure that the best choice is made.

