











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
In December 2013, the Oriental Republic of Uruguay enacted law 19.172 establishing a regulatory framework for the cannabis market. The Institute for Regulation and Control of Cannabis (Instituto de Regulación y Control del Cannabis, IRCCA) was created to regulate plantation, cultivation, harvest, production, processing, stocking, distribution and sale of cannabis, and to promote actions to reduce the risks and damage associated to the problematic use of cannabis 1 . In June 2018, 35.246 people were registered for regulated access to marijuana, of whom 2.339 figured as members of 91 cannabis clubs 2 . Data for frequency of marijuana consumption in Uruguay according to age range show that approximately one out of every five persons between the ages of 26 and 35 years uses it daily, with this age range having the highest consumption. In addition, it was found that out of every 100 persons who had tried marijuana, 7 showed problematic use of the substance 3 . Xerostomia is one of the adverse effects observed in the oral cavity associated to cannabis consumption 4 . This condition is related to difficulties in adequate control of biofilm and to increased gingival inflammation 5 . Moreover, gingivitis and periodontal diseases are among the most prevalent diseases in in the world. World prevalence of total periodontitis has been reported as 5% to 70%, with differences among age ranges 6 . Moreover, it has been reported that approximately 11% of the population has severe periodontitis 7 . Risk factors for periodontitis, such as smoking and diabetes mellitus, have been extensively studied 8 , as have environmental and behavioral factors, and certain microbiological aspects.
Self-reporting of different medical conditions such as diabetes, hypertension or myocardial infarction has been used for several years as a basis on which to monitor health status and trends over time in populations. In 2003, in the USA, self-reported evaluation was promoted as an alternative measure for surveillance of periodontal disease, since clinical examination requires great use of resources, both human and logistic, substantially increasing costs 9 . Later, in 2007, results of the Australian National Survey of Adult Oral Health 10 were published. This survey included 11 questions (6 gingivitis and periodontal disease screening questions and 5 conventional risk indicators) in large population surveys, yielding useful levels of validity in predicting moderate/severe to severe periodontitis. A joint study by the Centers for Disease Control and Prevention (CDC) and the American Academy of Periodontology (AAP) 11 proposed to use eight questions in English and Spanish, which were subsequently assessed for validation in populations in the USA (including Spanish speakers) 12 . The use of this tool was studied further in Brazil, as part of a questionnaire consisting of 18 questions 13 , and in France, where an additional four questions were included 14 . Validation in Spanish was performed in
Spain, both in Madrid 15 and in Barcelona 16 , where a set of 12 questions, including the 8 mentioned above 11 , was used.
Verhulst et al 17 applied the questionnaire created by Eke and Genco 10 at the Academic Centre for Dentistry, Amsterdam (ACTA, by its acronym in Dutch), based on which they proposed 3 models for predicting total periodontitis and severe periodontitis. Model 1 uses self-reported answers on periodontal disease, demographic data and oral biomarker values, model 2 uses self-reported answers and demographic data, and model 3 uses only self-reported answers on periodontal disease. The authors found that model 3 provides acceptable values for predicting periodontitis.
A systematic review with meta-analysis published in 2016 18 shows that in general, self-reporting is useful for identifying presence of periodontitis. The sensitivity values for most of the questions were lower than the specificity values, therefore these questions are better at identifying people who do not have periodontitis.
Several epidemiological studies have addressed gingival and periodontal health status in cannabis smokers 19-22 , finding a positive association between smoking cannabis and periodontal health status. A recent systematic review 23 of a wide range of studies suggests this association may be dose-dependent, and recommends further studies with longer follow-up times and control for risk factors/indicators such as tobacco, diabetes and age. It also recommends reporting how long the substance has been used, use frequency, and substance composition and quantity. Thus, exploratory studies are still required to further address the issue of association between marijuana consumption and periodontal diseases.
The aims of this exploratory study are therefore to describe self-reported gingival-periodontal status and to estimate the prevalence of periodontitis based on a predictive model among members of cannabis clubs in Montevideo, Uruguay.
MATERIALS AND METHODS
A cross-sectional study was performed from July to October 2018, based on a convenience sample of cannabis club members in Uruguay. This survey was approved by the Ethics Committee at the School of Dentistry, University of the Republic (Uruguay).
In June 2018, there were 109 clubs with membership registered at the IRCCA, representing 2339 persons over 18 years of age. Fifty percent of these clubs were in Montevideo. Invitations to participate in the survey were extended through the president of the IRCCA, who informed the directors of the cannabis clubs via email, asking them to send club members the invitation to participate in the survey. People who expressed interest in taking part in the study were contacted by the research team to provide further information on the study and arrange a meeting for interviews. When there was no answer, invitations were sent for a second time after two months.
After reading and signing informed consent, each subject completed a voluntary, self-administered survey containing multiple-choice questions. With guidance from two researchers (SP and MM), questions were asked about identity data, sociodemographic characteristics, and profile regarding consumption of cannabis, alcohol and other drugs.
Self-reported gingival-periodontal health status was evaluated based on the Spanish version of a set of questions suggested by Eke and Genco 11 (Q1-Q8). Before beginning this study, the questions were assessed for clarity, ease of understanding and cultural adaptation by testing them on 20 patients at the Periodontics Clinic at the School of Dentistry, University of the Republic. Finally, the data collected in the surveys were entered in spreadsheets for subsequent analysis. Total exposure to tobacco was calculated in “pack years” for current smokers, following Susin et al 24 , forming 3 groups: Light (1 to 2734 packs), Moderate (2735 to 7300 packs) and Heavy (more than 7300 packs). Mean age ± standard deviation (SD) was calculated. Prevalence was estimated for total periodontitis (TP) and severe periodontitis (SP), based on two predictive models (models 2 and 3) proposed by Verhulst et al 17 . For total periodontitis, model 2 employs the data from questions Q2, Q3, Q4, Q8 and age, while model 3 includes data from questions Q2, Q3, Q4 and Q8. For severe periodontitis, model 2 employs data from questions Q2, Q3, Q4, Q8, age and sex, while model 3 uses questions Q2, Q3, Q4 and Q8.
RESULTS
A total 56 members of five cannabis clubs agreed to answer the questionnaire. Of these, 50 completed the survey and 6 decided not to participate due to lack of time. Table 1 provides respondent demographics, showing that the proportion of males was higher than females (68% vs. 22%), 60% had university-level studies, and 76% were employed or self-employed. It shows that the population is young, with mean age 32 (±7.8) years, with the age range 20 to 40 years making up 78% of the total.

For toothbrushing frequency, 90% ofthe respondents reported brushing their teeth twice a day or more, while 10% reported doing so only once a day or less. Regarding tobacco use ( Table 2 ), the number of smokers was equal to the number of former smokers and similar to the number of people who had not smoked tobacco previously. Table 2 also shows the characteristics of tobacco consumption and the number of “pack years” 24 for respondents who agreed to report how long they had been smokers and how much they consumed, of whom 10 were light, 5 moderate and 2 heavy smokers.

Table 3 shows consumption of alcohol and other drugs. Most respondents reported consuming alcohol one to four times a week (62%). In addition, 21 respondents reported using other recreational drugs (e.g., cocaine, designer drugs or others), of whom 12 declined to provide frequency of use.

Table 4 shows time and frequency of cannabis use, showing that 56% had smoked cannabis for more than 10 years and 70% did so daily. Half the sample reported using less than 20g per month, with the other half reporting more than 20 g per month, among whom 6 persons used more than 40 g per month.

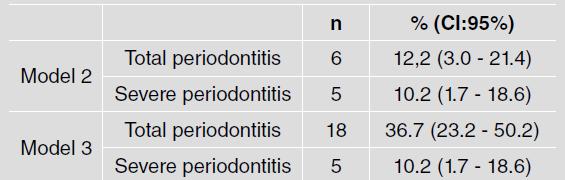
Evaluation of the 8 specific questions on self-reported periodontal disease ( Table 5 ) found that only one person did not answer any of the questions, so that the answer rate was 98% for all questions. Table 6 shows prevalence of total periodontitis (TP) and severe periodontitis (SP). With model 2, prevalence of total periodontitis was 12% (6 cases) and prevalence of severe periodontitis was 10% (5 cases), while with model 3, the values were higher, TP 36% and SP 10%.

DISCUSSION
This study evaluated self-reported periodontitis among recreational cannabis users who were members of cannabis clubs in Montevideo, Uruguay. This study has no parallel in the literature because it was conducted in Uruguay, which regulates recreational cannabis use, allowing distribution and/or sale of cannabis in pharmacies, home cultivation and the so-called cannabis clubs. These clubs are associations that gather cannabis users and are located throughout the country. The clubs are registered at the IRCCA, a public, government-sponsored legal entity. The current study is one of the first to focus on cannabis club members with the aim of learning about situations of disease, and the first to address periodontal health issues. Possibly as a result of this, plus mistrust regarding the use of data, there were difficulties in collecting data.
Given the confidentiality required for the study, the sampling process was administered by the IRCCA, which sent the consent forms and the survey to the coordinators of each club. The coordinators sent the forms to club members, although some of them prevented the process from continuing. The response rate from clubs was very low - less than 5%. Questionnaires were applied to a total 56 Uruguayan cannabis club members. Thus, this study does not intend to claim external validity, but provides a first exploratory study in order to propose future research hypotheses so that, over time and when the use policy matures, other studies may be conducted with higher response rates.
Due to the peculiarity ofthe sample, it is not currently possible to achieve greater approximations by means of, e.g., clinical examinations or other additional parameters. This study used self-reported results for periodontitis provided by cannabis club members, as well as their sociodemographic characteristics, hygiene habits, and associated addictions, among other factors. Self-reported periodontitis was evaluated through the Spanish language version of the questions developed by Eke and Genco 11 .
Six of the subjects declined to respond to the questionnaire, alleging lack of time to answer. Therefore, although there is not a response rate for the total sample, about 10% did not respond effectively, a rate similar to those reported in previous studies such as Eke et al 25 .
The subjects who participated in this study were mainly male (68%), mostly in the age range 20 to 40 years (78%), and more than half had reached university-level studies. These situations are in line with the distribution data for recreational cannabis users 3 . In terms of occupation, distribution was similar to that of the general population, so it may be inferred that the study sample is very similar to the universe of cannabis users in Uruguay.
This study considered additional use of other illegal drugs which are often associated with recreational use of cannabis 26 . Prevalence of use of illegal drugs such as cocaine or other synthetic drugs was 42% of the sample. It is worth highlighting that, given the peculiarity of the question, 38% of the participants declined to answer, with an even higher percentage not answering the question about frequency of use of other drugs.
Ninety percent of the sample had consumed alcohol during the past year, which is higher than the percentage recorded in the country in previous years (71.1%) 3 . In turn, 62% of the sample reported consuming alcohol 1 to 4 times a week, which was also higher than previous data for the country 3 . With regard to smoking, one third of the sample were current smokers, which is similar to national data. However, frequency of tobacco consumption was lower than observed in the general population 3 .
The pattern of cannabis use shows that most respondents had been using it for over 10 years. This is considered long-term exposure., i.e., they were not occasional users or short-term users, so it may be inferred that at the time of reporting, any damage could already be detected. One of the important features of this study is that, in contrast to the occasional exposures reported in another study 27 , it evaluates frequent and regular cannabis users, since most of them consumed it on a daily basis and in considerable amounts per month, with 50% consuming more than 20 g per month. It is important to highlight that the values recorded for prevalence as well as frequency of use (daily and over the past 12 months) in cannabis users in Uruguay has increased relative to surveys conducted in 2016 3 and 2007 28 , with highest prevalence of use among men aged 18 to 34 years, with similar sociodemographic characteristics.
In the current study, the results for estimated prevalence of self-reported periodontitis differed according to the model applied, particularly for total periodontitis, which was 12.2% in model 2 versus 36.7% in model 3. In contrast, both models found the same percentage (10.2%) for severe periodontitis. This may be explained by the characteristics of this convenience sample, where there is predominance of male sex and persons younger than 40 years, which are variables that are employed in model 2 proposed by Verhulst et al 17 . These data are similar to the distribution found for Uruguay’s adult population in its 2015 National Oral Health Survey 29 , although it is interesting to note the difference in terms of age ranges, because the survey presents data for a population aged 35 to 44 years. It is therefore possible that exposure to cannabis could have a slight influence on the onset of periodontitis at an earlier age.
The main limitations of this study were the difficulty to access a larger sample, and the calculation of the response rate. However, among the advantages of this peculiarity is the fact that the sample consisted of recreational cannabis users who were officially registered at clubs. The fact that periodontitis was evaluated through self-reporting may also be considered a limitation, even though self-reporting is currently widely validated, despite the possibility of memory bias 30 .
To conclude, this study showed that among young people who are members ofcannabis clubs in Uruguay, the prevalence of self-reported periodontitis can be considered high compared to available data for the general population with similar sociodemographic and behavioral conditions. This suggests that smoking cannabis could have a potential detrimental effect on oral health status. This exploratory study provides a basis for further research using larger samples with the aim of evaluating how cannabis smoking affects the prevalence and progression (by means of longitudinal studies) of periodontitis in users who are members of cannabis clubs.

