











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Health is interpreted as the outcome of factors related to ways of life, lifestyles and quality of life, and recognizes the involvement of the following variables: (a) the oral and dental healthcare models in different countries as a result of the characteristics of their respective healthcare systems and (b) the characteristics of knowledge management implemented at graduate and postgraduate levels of healthcare studies 1-3 .
Dental caries is the outcome of complex interaction over time between acid-producing bacteria, fermentable carbohydrates, and the host’s internal and external factors. The risk of developing caries includes physical, biological, socio-environmental, and behavioral characteristics and factors related to living conditions and lifestyle. The micro-circumstances for caries development include different microorganisms, incompetent salivary flow, insufficient exposure to fluoride, and chemically propitious nutrition variables. The outcome of these processes causes a progressive net loss of minerals in dental tissues, enabling caries lesions to develop 4 . The initial caries lesion is intended to maintain or recover the health of the affected tooth/teeth 5 . Available indicators for addressing dental caries conceptually and operatively must conform to the theoretical framework on which studies are based and enable precise identification of the process of clinical development of the disease from its early stages to its complications. The available indicators may be simple or complex. The transfer of the results expressed by the different values must help to systematize diagnosis and guide proactive, efficacious, effective, and long-lasting interventions. The various indicators that have been developed can be classified according to the different variables that they address 6 : the past history of caries; the risk factors involved 7 ; the stages in the development process of dental caries lesions 8-9 ; and the integration between the process of caries lesion development in terms of magnitude (severity and extension) and the treatments recommended according to the approach for risk control 10-11 . Also, it is necessary to clarify the differences between caries diagnosis and lesion identification. Diagnosis involves the dental professional’s interpretation regarding the sum of available data, while lesion identification involves applying an objective method to determine whether or not the lesion is present, and once it has been identified, the assessment can be established. Pitts et al. 12-14 and Ekstrand et al. 15 , 16 developed the International Caries Detection and Assessment System (ICDAS II) - a system for caries detection and assessment that integrates three dimensions based on the lesion development process, which synthesizes substantial evidence for making political, sanitary and clinical decisions.
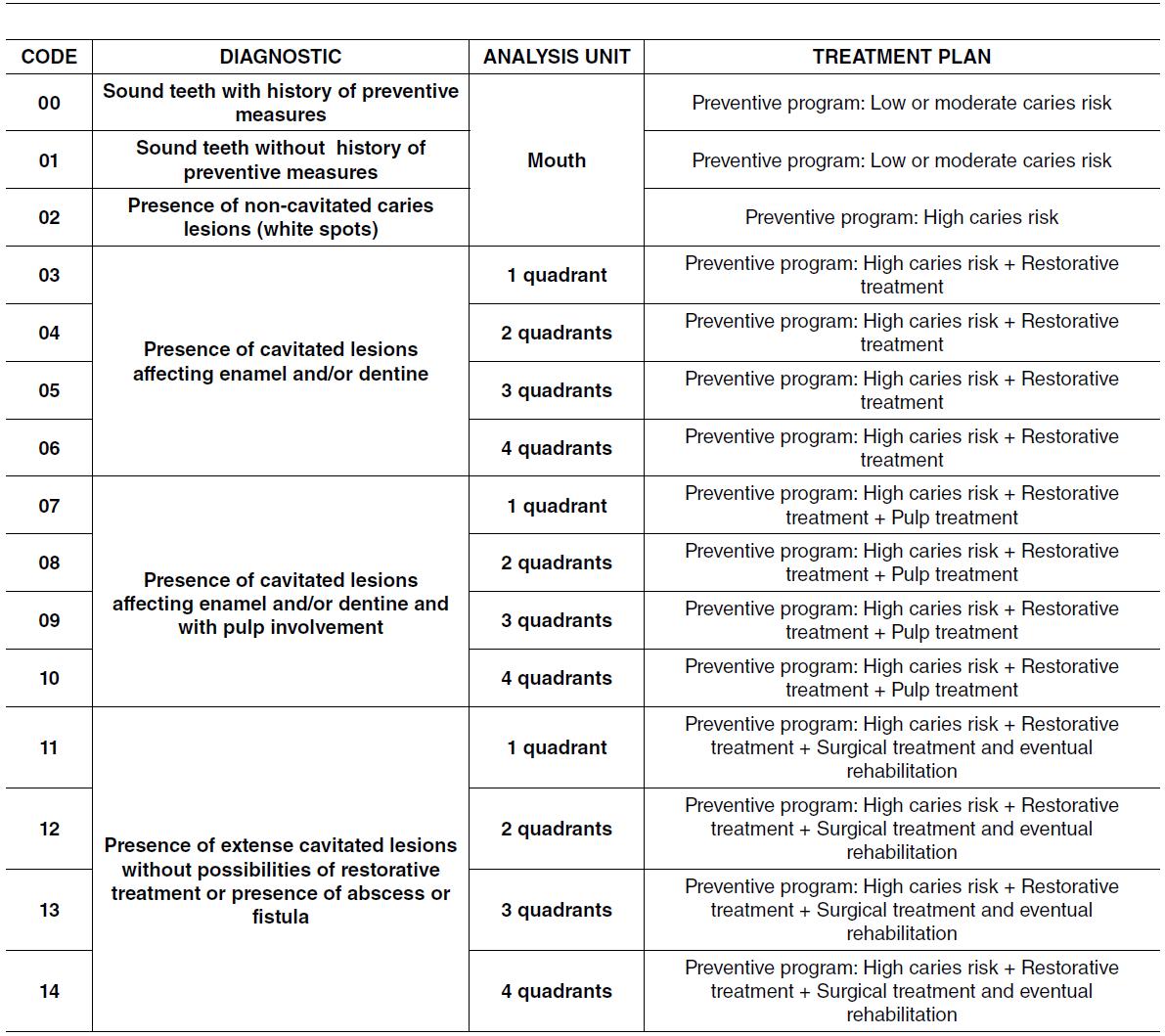
In 1993, the Caries Treatment Needs Index (CTNI) ( Fig. 1 ) was designed and applied. The CTNI is based on the interaction of two axes: one based on the lesion’s progression and the other based on the technological resources needed to control the risk of dental caries 17-18 . The progression axis identifies the magnitude of severity and extent. The component referring to the magnitude of severity identifies the process of tissue compromise of the dental caries lesion, going from a clinical threshold recognized as white spot 19 , which is distinct from the white spot caused by hypomineralization to subsequent progression in cavitation, including dental tissues. The magnitude of extent in the “mouth unit” is expressed by the number of mouth quadrants with visible lesions. The technological axis includes the risk component and the available technological development component. The risk component results from variables identified and often caused by the previous omission of appropriate actions for controlling the process. Technological development is based on contextualized scientific evidence and expressed as the proper strategies and their application per mouth unit and teeth, according to the magnitude recorded in dental quadrants.
Any index must be validated regarding the reliability and validity of the construct, contents, and criteria 20 . Rigorous application of indices by the examiner requires a calibration process including (a) theoretical knowledge ofthe indicator and cutoff points between its categories, (b) practical recognition in situations “on paper” and in the clinic, and (c) calibration per se, establishing inter-examiner differences between the “gold standard” or “reference examiner” and the new examiner, and intra-examiner differences, i.e., the variations recorded among observations made by one professional.
Dental caries is one of the most prevalent chronic diseases globally, affecting people throughout their lifetime 21 . Today, its distribution and severity vary among different regions, and its onset is strongly associated with environmental, sociocultural, economic, and behavioral factors 22-24 . The epidemiological profile of dental caries differs significantly between central and developing countries. However, variables that identify complex social issues such as poverty provide a perspective from which to analyze heterogeneity within the homogeneity of countries. In Argentina, Piovano et al. 22 studied the magnitude of dental caries, establishing the treatment needs in a sample of 2917 children, adolescents, and adults. Kassebaum et al. 23 conducted a worldwide systematic review and meta-regression using epidemiological data on untreated caries and subsequent estimates of internally consistent prevalence and incidence. Separate meta-regression was performed for untreated caries in primary and permanent teeth,
respectively, using the Global Burden of Disease
model 24 .
Different authors have compared dental caries indices. Campus et al. 25 compared ICDAS, CAST, NYVAD, and DMF indices. They demonstrated that the most significant difference among methods was shown by the number of sound teeth (p < 0.01). In a cross-sectional study, Sarno et al. 26 demonstrated that the mean time taken to apply the DMF was 3.8 min; for ICDAS, it took 8.9 min, and for CAST, 4.7 min. The mean numbers of decayed, missing, and filled teeth were 6.0 according to the DMF, 6.2 according to ICDAS, and 5.9 according to CAST. When the disease extension indicator was used, the following percentages of teeth were affected by caries: DMF 22.12%, ICDAS 49.11%, and CAST 33.2%. The DMF underestimated the occurrence of caries lesions in individuáis but was the fastest method to apply. ICDAS obtained detailed information regarding lesion severity, but it was a time-consuming method and challenging to analyze. A systematic review based on specificity and sensitivity studies of each system 27 revealed that sensitivity and specificity are greater with ICDAS than with the dmft/DMFT index and provide up to 43% more information in identifying non-cavitated lesions. Still, it takes longer to perform and involves more resources because it uses light, compressed air, and prophylaxis before the examination. Banava et al. 28 revealed that the ICDAS provides more accurate information than DMF for the investigators and epidemiologists. Similar findings were reported by Melgar et al., who informed that the DMFT index might underestimate 60% of non-cavitated lesions in children and 16.6% in adults 29 .
The objective of this study was to establish the correlation between an index for caries treatment needs and an index for caries lesions detection and evaluation.
MATERIALS AND METHODS
The study project was approved by the Ethics Committee of the School of Dentistry of the University of Buenos Aires. (PAIIO-02 2019-2024). A cross-sectional study was designed on a non-probabilistic sample of children and early adolescents (n=546) with no previous dental care during the last year ( Table 1 ):
A group 3-year-old children (n= 302) from an early childhood center (Avellaneda, Provincia de Buenos Aires).
A group of 5-year-old children (n= 183) from two kindergartens (Rio Grande, Provincia de Tierra del Fuego, Antártida e Islas del Atlántico Sur).
A group of 11 to 14-year-old early adolescents (n= 61) from a middle school (Ciudad Autónoma de Buenos Aires).

According to existing national criteria, the three institutional settings were classified as belonging to marginal urban level neighborhoods.
Before including children in the study, their legal guardians were asked for informed consent, and each child’s formal assent was verified. All participants and their legal guardians were informed of the results of the examinations and diagnoses and included in and/or referred to a dental care program at local institutions.
Clinical diagnoses were performed by one researcher who was calibrated in caries diagnosis according to CTNI (18) and ICDAS II criteria (kappa 0.75). Results of dental examinations were recorded in individual charts and used to design individual treatment plans.
On each patient, the indexes were operationalized as follows: CTNI grouped according to 4 standardized categories: code 00-02 (sound teeth with or without preventive measures or presence of non-cavitated caries lesions; code 03-07 (presence of cavitated lesions affecting enamel and/or dentine in 1 to 4 quadrants); code 07-10 (presence of cavitated lesions affecting enamel and/or dentine and with pulp involvement in 1 to 4 quadrants); and code 1114 (presence of extense cavitated lesions without possibilities of restorative treatment or presence of abscess or fistula in 1 to 4 quadrants).
ICDAS II were grouped in 7 categories: Code>0; Code >3; Code 1-2; Code 3; Code 3-4; Code 5-6 and Codes 4-5-6. In all cases, only active caries lesions were included. Also we grouped for other analysis ICDAS codes in 3 categories: Category ICDAS >0 (number of surfaces with lesions ICDAS code 1 to 6); category ICDAS 3 to 6 (number of surfaces with lesions ICDAS code 3 to 6); and category ICDAS =0 (number of surfaces without lesions ICDAS code =0).
Statistical analysis
Frequencies, percentages, median, and quartiles were calculated for the values recorded using both diagnostic methods. The Jonckheere-Terpstra ordered alternatives test for independent samples was used to compare the distribution of lesions ICDAS = 0, ICDAS>0, and ICDAS 3 or higher among the 4 CTNI groups. For pairwise comparison, they were adjusted using Bonferroni’s correction. Correlation between CTNI and ICDAS was established by Spearman’s rho coefficient. For comparison between indices, the ROC curve was used with Hanley and McNeil's approximation method. Area under the curve was calculated with 95% confidence intervals; cutoff variable was established as CTNI 00-02 / 0314 and CTNI 00-06 / 07-14; and variable dependent on the distribution of affected surfaces as ICDAS > 0, ICDAS 3-6, ICDA 4-6, and ICDAS 5-6.
RESULTS
Analysis of correlation of surfaces diagnosed according to ICDAS II and CTNI
The distribution of lesions ICDAS = 0, ICDAS > 0 and ICDAS 3 or greater with CTNI grouped as: 00-02, 03-06, 07-10 and 11-14 is shown in Fig. 2. Statistically significant differences are observed upon comparing CTNI grouped in 4 categories to the distribution of surfaces according to ICDAS=0, ICDAS>0, ICDAS 3 or greater (p<0.000). Pairwise comparison of CTNI according to distribution of ICDAS lesions showed statistically significant difference except between categories 07-10 and 11-14, with non-significant differences in the three comparisons performed. As the complexity of the record of lesions according to CTNI increases, there is an increase in the number of surfaces diagnosed with ICDAS>0 and with ICDAS > 3, and a decrease in caries-free surfaces recorded with ICDAS II., except between categories 07-10 and 11-14, with non-significant differences in the three comparisons performed. As the complexity of the record of lesions according to CTNI increases, there is an increase in the number of surfaces diagnosed with ICDAS>0 and with ICDAS > 3, and a decrease in caries-free surfaces recorded with ICDAS II.

Fig. 2 Distribution of quantity of ICDAS surfaces per grouped CTNI ICDAS>0: number of surfaces with lesions ICDAS 1 to 6 ICDAS 3to 6: number of surfaces with lesions ICDAS 3 to 6 ICDAS=0: number of surfaces without lesions ICDAS =0
The correlation between CTNI scores and distribution of surfaces for ICDAS>0, ICDAS=3-6, ICDAS=4-6, ICDAS=5-6, ICDAS=3-4, ICDAS=1-2 and for the number of surfaces without lesions ICDAS=0 was calculated for the age groups studied and for the total sample (Table 2; Fig. 3). In all cases, the results of Spearman’s correlation were statistically significant, except for the group 11-14 years for distribution of lesions ICDAS=1-2. The correlation between CTNI scores and the distribution of surfaces for ICDAS>0, ICDAS=3-6, ICDAS=4-6, ICDAS=5-6, ICDAS=3-4 for each age group was very high. For distribution of lesions ICDAS=1-2, the correlation was low but statistically significant. The correlation between CTNI score and distribution of lesions ICDAS=0 (number of surfaces without lesions) was very high, and high and inverse (negative) for each age group. Fig. 3 describes the correlation between CTNI and ICDAS>0.

Table 2 Spearman’s correlation between CTNI and different groupings of ICDAS lesions for the 3 age groups and for the total

Analysis of the results of the ROC curve for distribution of lesions ICDAS for CTNI 00-02 vs. 03-14 and CTNI 00-06 vs. 07-14.
For CTNI 00-02 / 03-14, area under the ROC curve is very high for ICDAS>0 and ICDAS=3-6, and high for ICDAS=4-6 and ICDAS=5-6 (Table 3; Fig. 4). For CTNI 00-06 / 07-14, area under the ROC curve is very high for ICDAS>0, ICDAS=3-6, ICDAS=4-6 and ICDAS=5-6 (Table 4; Fig. 5).

Table 3 Area under the curve and CI95% for cutoff values CTNI: 00-02 vs. 03-14 for distribution of surfaces ICDAS>0, ICDAS 3 or greater, ICDAS 4 or greater, ICDAS 5 or greater

Fig. 4 ROC Curve. Cutoff values CTNI: 00-02 vs. 03-14 for distribution of surfaces ICDAS>0, ICDAS 3 or greater, ICDAS 4 or greater, ICDAS 5 or greater

Table 4 Area under the curve and CI95% for cutoff values CTNI: 00-06 vs. 07-14 for distribution of surfaces ICDAS>0, ICDAS 3 or greater, ICDAS 4 or greater, ICDAS 5 or greater.

DISCUSSION
In general terms, health indicators represent summary measurements capturing relevant information on different attributes and dimensions of health status and healthcare system performance which, viewed jointly, intend to reflect the health situation and can be used for surveillance. Indicators must be easy for analysts to use, interpret, and understand to users, such as decision-makers and managers.
A set of health indicators with quality attributes that are appropriately defined and maintained provide information for preparing an epidemiological profile and other kinds of analysis of the health-disease-attention-care situation. The selection of such a set of indicators -and its levels of disaggregation- can vary according to the availability of information systems, data sources, resources, needs, and specific priorities in each region or country.
It is essential to monitor indicator quality because it conditions users’ confidence level in health information, and therefore, the regular use of indicators.
Health indicators also depend on the policy for disseminating them, including the timeliness and frequency they are compiled. Availability of a basic set of indicators provides the raw material for analyzing health. Moreover, it can facilitate the monitoring of health objectives and goals, foster analytical capacities in healthcare teams, and serve as a platform for promoting the development of intercommunicated health information systems. Valid and reliable health indicators are essential tools required by epidemiology for health management. The indices compared in this study provide the possibility of analyzing the impact on health scenarios. Clinical discrimination among different stages in caries lesion processes, activity, and arrest, supported by various histological and histochemical studies, finds appropriate clinical instruments.
In statistics, a proxy variable is a measure that enables other more valuable variables to be found, whether for designs or for including the results indistinctly in information technology. For such purpose, the proxy variable must have a strong correlation -though not necessarily linear or positive- with the inferred value. Both the indices analyzed in this study meet this requirement. When comparing results obtained by other authors, the INTC takes as criteria for categorizing the development process of dental caries, identifying the first of the visual differences with healthy tissue. In such a sense, it coincides with the ICDAS in all its formulations.
The CTNI index. Based showed a higher correlation than other indicators with ICDAS II. It is worth highlighting the frequent calibrations requiring and verifying the equivalence between the therapeutic criteria recommended in the CTNI and the ICDAS II. The indices analyzed in this study (CTNI and ICDASII) show reasonable equivalence for use in clinical and epidemiological studies based on the statistical analysis. Comparing these indicators to other indicators, including their application in studies on different life stages, would enable their validity and relevance to be considered for global health studies.

