











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Clinical decision-making, which is a relevant area of healthcare, is based on both clinical and non-clinical factors 1 . Non-clinical factors are subjective determinants such as time since graduation or patient socioeconomic status 1 . Thus, the clinical decisions regarding techniques and materials may vary according to the profile of both patients and professionals. Knowledge of the factors involved in this process is relevant to defining behavior and implementing more effective strategies for promoting healthcare services 2 . Dental professionals are strongly encouraged to apply evidence-based dentistry (EBD) when making decisions 3 . Nonetheless, most dental treatments cannot be truly described as based on experimental evidence 3 . Diagnostic errors are common and recognized as a source of preventable adverse events, but they are rarely evaluated because of the complex decision-making process 4 . In this regard, the factors associated with dental clinical decision-making still need to be explored.
The concept of EBD advocates minimally invasive dentistry, and adoption of a philosophy of prevention and avoidance of invasive treatments, with minimum removal of healthy tissues 5 . Some studies have associated several subjective determinants to dentists’ decisions on whether to treat patients with either more aggressive or more conservative approaches 1, 2 . However, literature is still scarce on other factors such as the association between graduate programs and the application of minimally invasive dentistry.
Another point that requires further study is dental professionals’ clinical decision-making regarding esthetics. Some studies have detected the controversial replacement of satisfactory amalgam restorations by composite resins because of amalgam’s inferior esthetics 2, 6 . The current study evaluates whether non-clinical subjective factors influence the treatment decision-making of Brazilian dentists based on technical and esthetic matters.
MATERIALS AND METHODS
This study was approved by the University Ethics Committee (32149220.7.0000.5291). The present research is a cross-sectional analysis based on a self-administered electronic questionnaire.
Study design and target population
The target population consisted of professionally active dentists throughout the Brazilian territory. Participants were invited to take part in this study via e-mail contacts provided by the Regional Dentistry Council and via available dentistry-related social media.
Development and structure of the data collection instrument
The data collection instrument was developed following a strict order to ensure reliability of results: (1) Establishment of conceptual structure, objectives of the instrument and target population, (2) Preparation of the questionnaire, (3) Application of the questionnaire to scientific consultants, (4) Pre-testing of the questionnaire with the target population, (6) Sample calculation, and (7) Data collection.
The data collection instrument was prepared according to the definitions and objectives established. The instrument was divided into 2 sections: the consent form and the questionnaire. After receiving an invitation to participate in the survey, participants accessed the informed consent form, which presented the objectives, methods, risks, and benefits of participating in the study. The professionals were only redirected to the questionnaire if they chose to participate voluntarily in the research. For the second section, extraoral and intraoral photographs obtained with informed consent from 2 patients were used to produce a clinical case with technical and esthetic questions. Treatment 1 (T1) of the clinical case involved the right mandibular first molar, which showed significant destruction of more than 2/3 of the crown and associated spontaneous pain (Fig. 1). Treatment 2 (T2) involved the adjacent right mandibular premolars, which had extensive Class II cavities with amalgam restorations and no carious lesions or any other associated complaint (Fig. 2). After preparing the clinical case, questions were developed based on a previously validated questionnaire 2 and literature review. The most appropriate treatment decisions for T1 and T2 were defined as root canal treatment followed by indirect restoration 7 and no treatment 2, 8 , respectively.

Fig. 1 Clinical case 1 presented in the questionnaire (T1), showing the intraoral occlusal view of the right mandibular first molar with extensive crown destruction.

Application of the questionnaire to scientific consultants
Once the initial questionnaire had been designed, it was applied to scientific consultants to test the hypothesis that the prepared items represented and adequately contemplated the domains of the desired construct 9 . A committee of 20 scientific consultants (reply rate = 85%), made up of dentistry university professors, was invited to make comments, suggestions and modifications on the questionnaire. Next, a quantitative evaluation was performed, in which the scientific committee’s agreement rate (%) was calculated for each question as the ratio between the number of consultants that made a suggestion for improvement and the total number of consultants. An agreement rate lower than
90% determined that the question needed to be discussed and modified, while an agreement rate of 90% or higher indicated that the question was adequate. In addition, a qualitative assessment was performed, in which the suggestions of scientific consultants were discussed to ensure the necessary changes.
Pre-testing of the questionnaire with the target population
A pilot study was carried out in December 2020 with 29 professionally active dentists in different regions of Brazil to assess the understanding, adequacy and applicability of the questionnaire. After each question, participants were asked about their understanding of the items, and to make any suggestions in the space provided. Based on the performance of pre-testing, the questionnaire was considered adequate and reliable. Participants’ answers and suggestions of were analyzed and considered for improvement of the questionnaire.
Questionnaire and data collection
The electronic questionnaire was structured using the QuestionPro survey software (Question Pro, Seattle, WA, USA) and applied from January 2021 to March 2021. The final version of the questionnaire consisted of 2 technical questions, in which the previously prepared clinical case was presented and the participants were asked about clinical decision-making. The patient’s socioeconomic status was not disclosed to avoid possible bias in the treatment selected. The following clinical case was presented: “A 40-year-old female patient visited the dental care service complaining of spontaneous pain in the right mandibular first molar. What would be your first treatment option for this tooth?”. The treatment options were (a) Extraction, (b) Extraction followed by three-unit fixed prostheses, (c) Extraction followed by dental implant, (d) Root canal treatment followed by indirect dental restoration, and (e) Root canal treatment followed by direct dental restoration. Then, the second question was presented: “The presence of amalgam restorations was also identified in the right maxillary premolars. The patient did not report any symptoms or complaints associated with these teeth. The radiographic examination did not show the presence of a carious lesion. What would be your first treatment option for these teeth?”. The treatment options were (a) Replacement with new amalgam restoration, (b) Replacement with composite resin restoration, (c) Replacement with ceramic onlay, (d) Replacement with ceramic crown, (e) Finishing and polishing, and (f) No treatment required. Professionals could select any treatment option for the cases presented, without restrictions.
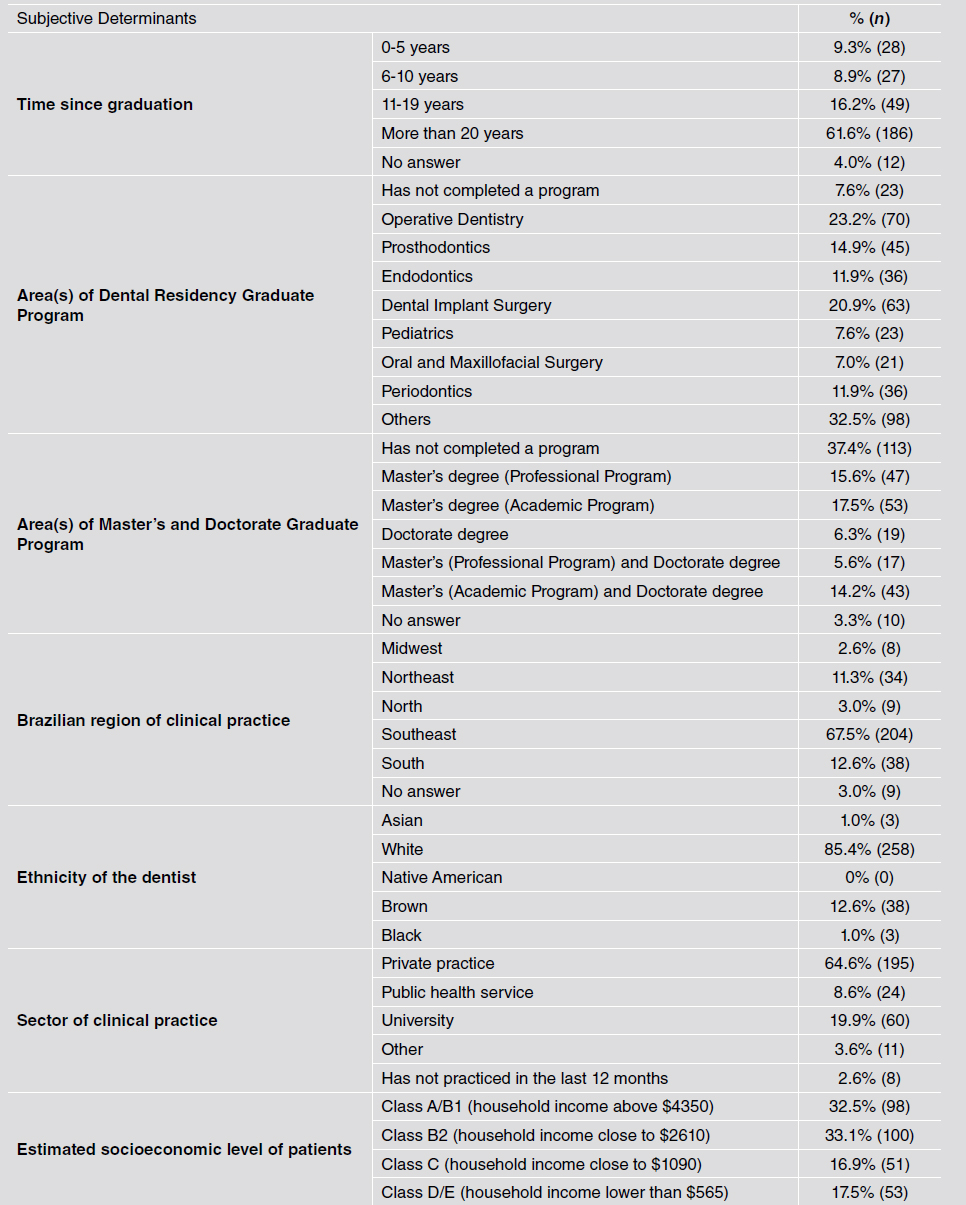
The questionnaire also included 7 questions on dentists’ sociodemographic and professional characteristics, to characterize their profile. The following sociodemographic and professional determinants were evaluated: (1) Time since graduation, (2) Area(s) of Post-Graduate Program/ dental residency Program, (3) Area(s) of Master’s and Doctorate Graduate Program, (4) Brazilian region of clinical practice, (5) Ethnicity of the dentist, (6) Sector of clinical practice, and (7) Estimated socioeconomic level of patients.
Sample size calculation
Based on a previous study with similar method 2 , in which an 83% agreement was obtained for a similar clinical approach, and using the Cochran equation, the standard significance level of 5% was applied and the minimum total sample size was determined as 217 individuals.
Statistical analysis
Data were processed using Excel software (Microsoft, Redmond, WA, USA) and analyzed with IBM SPSS 22 statistical software (IBM Corporation, Armonk, NY, USA). Chi-square test and Fisher’s exact test were used to analyze T1. For analysis of T2, a qualitative index presenting scores of 1 to 5 was developed to categorize the proposed treatment according to the loss of tooth tissues. Score 1 represented the lowest level of tooth tissue destruction (No treatment necessary), whereas score 5 characterized the most aggressive approach (Replacement with ceramic crown). Then, one-way analysis of variance was applied and, for the pairwise comparison of groups, the post-hoc Tamhane test was used. The significance level established for all analyses was a = 5%.
RESULTS
The electronic questionnaire was viewed by a total 1157 participants, of whom 385 started and 302 completed it (Completion rate = 78.4%). Average time spent answering the questionnaire was 4 minutes. The sociodemographic and professional characteristics of the participants are shown in Table 1. Most participants graduated 20+ years prior to this survey (61.6%) and worked in a private practice (64.6%). Most participants had completed a Post-Graduate Program/dental residency (92.4%).
The main choices for T1 and T2 were, respectively, “Root canal treatment followed by indirect restoration” (73.5%) and “No treatment needed” (55.3%) (Table 2).

Table 2 Distribution of treatments proposed by dentists for the clinical cases presented in the questionnaire:


Table 4 Treatments proposed for T2 (Premolars) according to the area of Dental Residency Graduate Program of the study participants:
The clinical decision-making for T1 was significantly influenced by the Brazilian región of clinical practice (p=0.005) (Table 3). In T2, having completed a residency program in Operative Dentistry (p=0.035) (Table 4), private practice (p=0.033) and most patients having higher estimated socioeconomic level represented by class A/B1 (household income above $4350) (p=0.002), significantly increased the loss of tooth tissues with the treatment proposed (Table 5). Most specialists in Operative Dentistry (58.6%) had graduated 20+ years ago, followed by 11 to 19 years for 16.8% of the respondents.

DISCUSSION
The results of this study indicated an association between some of the non-clinical factors tested and the treatments proposed in both T1 and T2. This is supported by the literature, in which determinants such as patients’ skin color were also associated to dentists’ clinical decision-making 1, 2 . The treatment proposed for the mandibular molar with extensive crown destruction and spontaneous pain indicative of irreversible pulpitis, presented in T1, had greater agreement among the study participants than T2. Only 3 professionals (1.0%) indicated T1 as tooth extraction followed by dental implant, whereas 299 dentists (99.0%) opted for more conservative treatments (root canal treatment followed by some type of crown restoration). This finding is favorable because the option of tooth extraction is considered an overtreatment for the case presented 7 . The only sociodemographic determinant that influenced the results of T1 was the Brazilian region of clinical practice. The growing regional differences in the index of decayed, missing and filled teeth (DMFT) of the Brazilian population may reflect the clinical routine and beliefs of professionals regarding treatments. The difference in the DMFT index among the Brazilian north and southeast regions was close to 20% in 1986, but this percentage increased considerably to 26% in 2003 and 43% in 2010 10 . The worst DMFT indexes are in the north and northeast regions due to spatial autocorrelation with low levels of access to dental care and higher levels of poverty, illiteracy, and lower levels of education 10, 11 . As a result, the northeast and north regions present a higher level of caries disease and a lower proportion of restored teeth compared to the southeast 10, 11 .
In T2, the most prevalent treatment selected for the maxillary premolars with amalgam restorations was “no treatment necessary” (55.3%), followed by “finishing and polishing” (24.2%). These options are also consistent with current concepts of minimally invasive dentistry supporting the removal of the least possible amount of healthy dental tissues. However, replacement of the satisfactory amalgam restoration by composite resin, ceramic dental crown, and ceramic onlay were selected, respectively, by 39 (12.9%), 12 (4.0%), and 9 dentists (3.0%); adding up to the considerable number of 60 dentists (19.9% of the total sample) selecting a procedure that is not justified. The esthetic component is subjective and depends on individual perception, and no complaint was associated to the restorations.
The motivation and effects of the specific barriers in the implementation of evidence-based dentistry should be investigated in future studies because dentists may be overestimating treatment options when compared to laypeople’s perception of smile. The clinical decision to replace restorations, particularly those that do not have an associated infection, should always be based on high professional criteria and consideration of patient feedback to avoid misconceptions. Restoration substitutions should be avoided because they usually result in increasing cavity size, and thus in loss of healthy tooth structure, easily leading to a costly, repetitive restorative cycle 8, 12 . Esthetics play an important role in people’s lives and are directly associated with quality of life 13 . Some authors have suggested that the cosmetic industry and the dental profession have leveraged this importance to increase demand and, consequently, profits 2, 6 .
The clinical decisions made for T2 showed greater influence of subjective determinants. Having completed a residency program in Operative Dentistry significantly raised the mean aggressiveness of the treatment proposed. Most Operative Dentistry specialists would recommend “no treatment necessary” (38.6%), but this percentage was the lowest among all areas of Dental Residency Program. At the same time, Operative Dentistry professionals were the most likely to select the treatment options “finishing and polishing” (34.3%) and “replacement with composite resin” (21.4%), involving higher scores for tooth tissue loss, compared to other professionals. Generally, Operative Dentistry specialists routinely check restorations and esthetic dental procedures, resulting in a high level of smile esthetic demand 14 . The finishing and polishing procedure is considered favorable because it reverses the decision to replace old amalgam restorations and may extend the durability of restorations 15-17 , but it can cause loss of tooth tissue, contradicting the principles of minimally invasive, evidence-based dentistry. The choice of Operative Dentistry professionals to replace the presented amalgam restoration with composite resin may be explained by the differences among dentists in the esthetic perception of smiles, which is significantly impacted by the highest degree they have earned and area of clinical practice 18-19 .
Other determinants that increased the rate of tooth tissue loss in T2 were private practice and having more patients of high socioeconomic level (as estimated by respondents). The high cost of esthetic dental treatments and the difference in DMFT index according to socioeconomic status may explain these findings 11 .
The choice of treatment was more conservative in the present study than in the study by Chisini et al. 2 . This may be related to the information provided, considering that our study stated that the patient did not report any symptoms or complaints associated with these teeth, including esthetic factors. Another explanation may be related to the population evaluated, considering that the present study surveyed the entire national territory, not just the northeast and south regions.
This study used an electronic questionnaire because it provides fast, accurate data; is affordable, and follows the technological and dynamic trends of scientific method 20, 21 . Based on these characteristics, electronic questionnaires are preferred by most participants in epidemiological studies 22 . Traditional approaches (e.g., face-to-face interviews, telephone interviews and printed questionnaires) have shown a gradual reduction in participation rates, mainly in the last decade 23, 24 . Among the reasons suggested for the drop in response rates are the greater demand for participation in surveys, the use of smartphones, and a general decrease in volunteering 24 . It is also important to consider the challenges of conducting traditional interviews during the coronavirus (COVID-19) pandemic, which has had unprecedented effects on society. COVID-19 led to a massive rise in survey-based analysis, and the resources to conduct ethical, reliable, accurate research on digital platforms are increasingly being emphasized and explored 21 .
The strict sequence used to develop the data collection instrument for this study aimed to ensure the reliability of the method 25 . Questionnaire items were constructed and organized based on a pre-existing questionnaire and literature review 2 . Literature review is the most frequently used method for developing survey-based analysis instruments, though it is also appropriate to use an existing questionnaire resource because it ensures that the questions have been previously tested for psychometric qualities 25 . The application of the questionnaire to scientific consultants and the pre-testing stage with the target population, prior to data collection, are essential steps in survey-based methods. In conclusion, dentists’ clinical decision-making varies according to professional profile, mainly regarding the replacement of restorations because of esthetic concerns. Having completed a residency program in Operative Dentistry, working in the private sector, and most patients having a high estimated socioeconomic level are factors that reduce the use of minimally invasive dentistry in esthetic treatments.

