











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
There is increasing scientific interest in people’s wellbeing, and research seeks to understand the relationship between multidimensional constructs such as quality of life or self-esteem, and health 1 . Oral health conditions have been found to exert major impact on quality of life, giving rise to the term oral health-related quality of life (OHRQoL) 2, 3 . The literature has shown the negative impact of oral conditions such as malocclusion on the OHRQoL of young people, with strong repercussions on oral functions, and emotional and social wellbeing 4, 5 . Orthodontic treatment with a fixed appliance seeks to correct tooth positions and skeletal discrepancies, providing more functionally and esthetically favorable occlusion, and, consequently, better quality of life 6 .
Changes in OHRQoL have been observed during the orthodontic treatment of adolescents wearing fixed appliances. Deterioration in quality of life is common during the first months of wearing an orthodontic device, mainly due to the oral symptoms and functional limitations it causes 7 . However, interestingly, other studies have found a positive impact on adolescent emotional wellbeing, even during the initial stages of orthodontic therapy, thanks to their expectation of having their teeth corrected 7, 8 . The longitudinal studies available in the literature evaluate the impact of orthodontic treatment on adolescent quality of life by means of generic questionnaires to evaluate a condition-specific outcome of wearing a fixed appliance. Condition-specific questionnaires are more sensitive and more responsive, and thus provide more reliable results for evaluating a construct as complex as OHRQoL 9 .
A recent cross-sectional study used a condition-specific questionnaire on wearing a fixed appliance to compare the impact of orthodontic treatment between boys and girls in the sixth month of wearing the appliance. The impact on quality of life was more negative in girls than in boys. Girls expressed a more negative perception of the pain caused by the fixed device, difficulty in hygiene, and social impact, especially regarding interaction with their peers 10 . In the context of orthodontics, more in-depth evaluations of the differences between boys and girls are relevant, given that they may have different perceptions and expectations regarding health outcomes 11 . The aim of this longitudinal study is to compare boys and girls concerning the impact of the first year of orthodontic treatment with a fixed appliance on their OHRQoL, by means of a condition-specific instrument.
METHOD
Study design
This longitudinal study follows the guidelines set forth in Strengthening the Reporting observational Studies in Epidemiology (STROBE) 12 .
Participants, study location, data collection period, and ethics
The sample consisted of 79 male and female adolescents, 10 to 18 years of age, who were in the third month of orthodontic treatment with a fixed appliance at the School of Dentistry of the Federal University of Minas Gerais (UFMG), located in Belo Horizonte, Brazil. Any adolescents with cognitive disorders reported by their parents/guardians or with craniofacial anomalies were excluded from the study. Participants were recruited from January 2017 to December 2018, and data were collected from January 2017 to February 2020. This study was approved by the UFMG Research Ethics Committee concerning research involving human beings (No. 62116216.2.0000.5149).
Study Variables Dependent Variable: OHRQoL
The impact of wearing a fixed appliance on adolescent quality of life was evaluated with a condition-specific instrument - Impact of Fixed Appliances Measure (IFAM). This instrument was developed in England 13 , translated to Brazilian Portuguese, cross-culturally adapted, and subsequently validated for use in the Brazilian population 14 , resulting in a national version of the questionnaire, called B-IFAM.
The B-IFAM consists of 43 questions. The answer choices for each question follow the Likert scale of 1 to 5, with 1 = completely disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = completely agree. The overall B-IFAM score ranges from 43 to 215. Higher scores indicate more negative perception regarding the impact of wearing a fixed appliance on the respondent’s quality of life. These 43 questions can be broken down into nine domains: aesthetics (5 questions), functional limitations (3 questions), dietary impact (6 questions), oral hygiene impact (3 questions), maintenance (2 questions), physical impact (9 questions), social impact (5 questions), time constraints (5 questions), and travel/cost/inconveniences (5 questions). Each domain can also be scored individually. The B-IFAM was completed by the adolescents, without any help, with the exception of the questions in the two last domains, for which the parents/guardians helped them to answer the questions, as recommended by the authors. The adolescents answered the questionnaire to evaluate the impact of the wearing of a fixed appliance on their quality of life at two distinct times: three months (TI) and 12 months (T2) after beginning orthodontic treatment with a fixed appliance.
Independent variable: sex
Sex was the main independent variable, and participants were divided into two groups: female and male.
Confounding variables: demographic, socioeconomic, and clinical data
In addition to the sex variable, age and family income variables were collected. The family monthly income was evaluated according to the Brazilian minimum salary at the time of data collection, and established by adding together the monthly income of all the active family members. This variable was dichotomized by the median into adolescents whose families had a monthly income <2 minimum salaries and adolescents whose families had a monthly income >2 minimum salaries. The age variable was also dichotomized through the median in individuáis who were <12 years old and individuals who were >12 years old.
During clinical data collection, the adolescents underwent clinical examinations, performed in a room with dental equipment, under artificial light, using a WHO (World Health Organization) probe, and a clinical mirror. During this examination, the orthodontic indication of the extraction of pre-molars (yes/no) and the severity of the malocclusion were evaluated through the Dental Aesthetic Index (DAI) 15 . The DAI is a cross-cultural index that enables the evaluation of 10 occlusal characteristics related to dental-facial anomalies, according to three components: dentition (number of absent incisors, canines, and pre-molars), crowding and/or spacing (crowding in the region of the incisors, spacing in the incisor region, diastema between the maxillary central incisors, greater irregularity in the maxillary anterior teeth, and greater irregularity in the mandibular anterior teeth), as well as occlusion (horizontal trespass, anterior crossbite, open bite, and anterior-posterior molar relationship). Scores for each occlusal characteristic were multiplied by a coefficient and added to the constant of 13 in order to obtain the total score of the DAI for each participant. Based on the DAI scores, the adolescent could be classified into one of four levels of severity of malocclusion: slight malocclusion (DAI<25), defined malocclusion (DAI=26-30), severe malocclusion (DAI=31-35), and highly severe malocclusion (DAI>36) 15 . In this study, the severity of the malocclusion was dichotomized into slight/defined malocclusion (DAI< 30) and severe/highly severe malocclusion (DAI>31). The researcher responsible for data collection underwent a calibration process with another researcher who had experience and ability in the application of DAI. The calibration process took place in two stages, with the first stage being theoretical and the second, clinical. The theoretical stage consisted of discussing the criteria used in the DAI to classify the severity of the malocclusion and the need for orthodontic treatment. The clinical stage consisted of evaluating 15 plaster models and clinical exams of 15 adolescents who were not included in the main study. The evaluations were conducted separately by the two researchers in order to calculate inter-examiner agreement. After one week, the plaster models and the adolescents were re-evaluated by the researcher who collected the data in order to calculate intra-examiner agreement. The Kappa values were 0.80 and 0.90 for inter- and intra-examiner evaluations, respectively, being considered satisfactory values 16 . Finally, data on the type of fixed appliance worn (conventional, self-ligating, or aesthetic) were collected.
Pilot Study
A pilot study to evaluate the data collection strategy was conducted with 10 adolescents who were not included in the main study. No change in the data collection strategy was necessary.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science (SPSS, version 25.0, IBM Inc., Armonk, USA). First, the Kolmogorov-Smirnov test demonstrated that the total B-IFAM scores in TI and T2, as well as the difference between TI and T2, had normal distribution, For the latter, the negative sign (-) indicated a more negative perception of the OHRQoL from TI to T2, Participants with complete data were compared to individuáis excluded beeause of the loss of data, using the Fisher test for categorical variables (sex, age, monthly household income, severity of malocclusion, and orthodontic tooth extraction), and the t test for numerical variables (overall B-IFAM score in TI),
Females and males were compared for the variables age, family monthly income, malocclusion severity, and indication of orthodontic extraction of pre-molars, as well as for the outcome variables overall score of B-IFAM in TI, T2, and the difference between TI and T2, Fisher’s test and Pearson’s test were used for categorical variables and the t test was used for the numerical variables,
The erude and adjusted associations between sex and the variables difference in the overall B-IFAM score between TI and T2 were tested with linear regression. Regression coefficients and 95 % confidence intervals (CI) were determined as association measures, The adjusted regression model ineluded the control of the variables age, family monthly income, malocclusion severity, indication of orthodontic extraction, and the overall B-IFAM score in TI,
The domains of the B-IFAM were also compared between females and males, using the t test, The differences between girls and boys, the effeet size (the magnitude of the difference), and the 95 % CI were determined, As a referenee, effeet size values elose to 0,20 were small, values elose to 0,50 were médium, and values elose to 0,80 were large 17 , The minimal clinically important difference (MCID) was ealeulated by multiplying the standard deviation of the domain assessed for the entire sample (pooled standard deviation) by 0,5 18 ,
Finally, covariance was analyzed for comparisons of the domains of the B-IFAM between females and males, controlling for the type of fixed appliance.
RESULTS
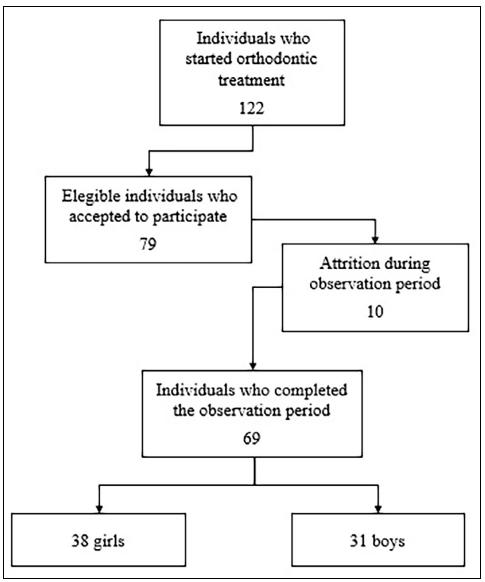
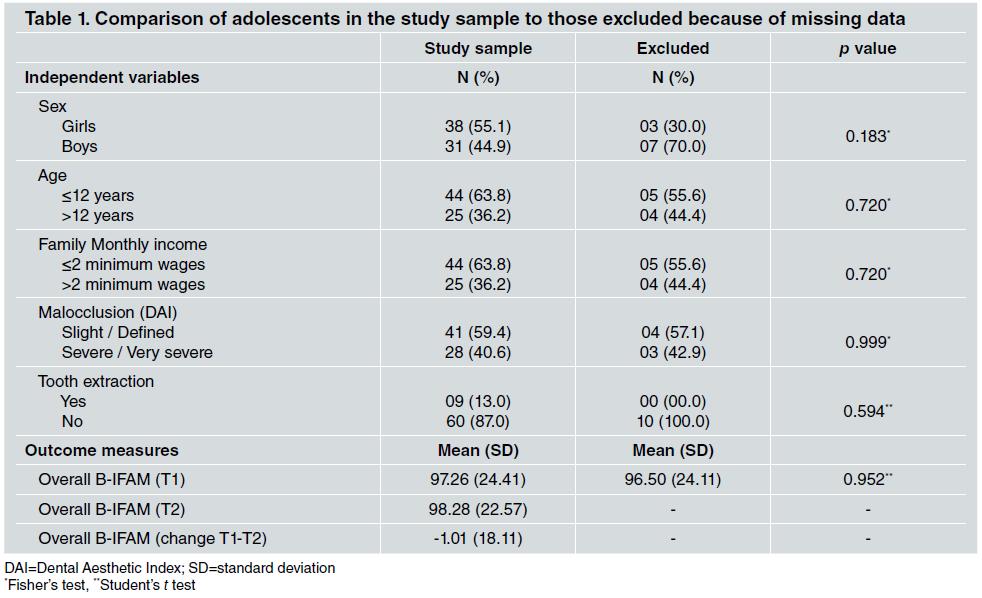
Of the 79 adolescents that began the study, 10 were excluded due to missing data (they did not fill out the B-IFAM at T2, or some other information was not provided), No difference was found between the 69 adolescents who participated in the entire study and the 10 who were excluded, for the variables sex and age, monthly family income, malocclusion severity, indication of tooth extraction, and the overall score of B-IFAM in T1 ( Table 1 ), Of the 69 adolescents who participated in the study, 38 were female (55.1%) and 31 were male (44.9%). Mean age was 12.32 years (±1.63). Fifty-five adolescents used a conventional fixed appliance, 13 used a self-ligating appliance, and one used an aesthetic device. Fig. 1 shows the flowehart of the study.
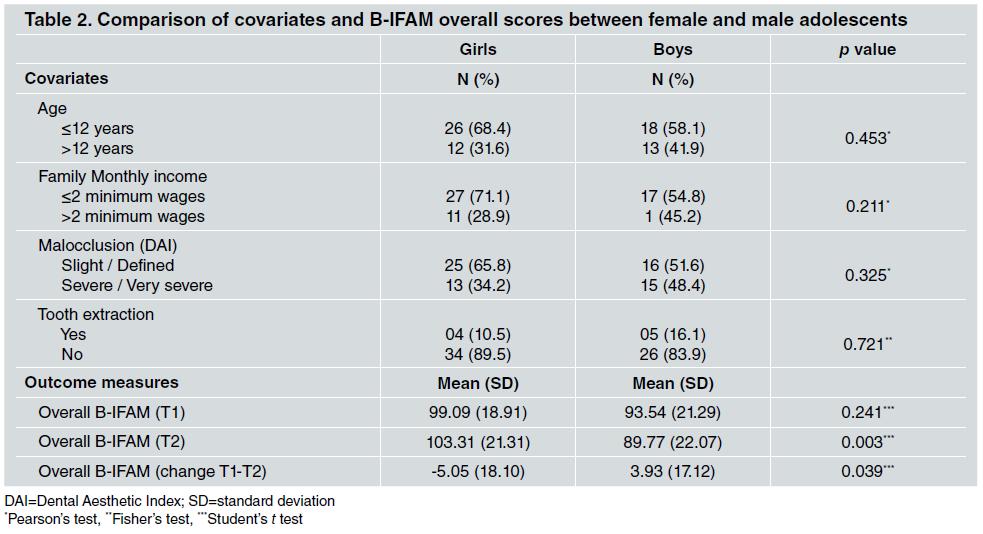
For the comparison between females and males, no signifieant difference was found for age, family monthly income, malocclusion severity, orthodontic tooth extraction, or the overall B-IFAM score in T1 (p>0.05). For the overall B-IFAM score in T2 (p=0.003), and for the difference of the overall B-IFAM score between T1 and T2 (p=0.039), girls had a more negative perception of the OHRQoL than boys ( Table 2 ).
In the adjusted regression model, girls had a significantly greater increase in overall B-IFAM score than boys, indicating a more negative perception of the OHRQoL during the observation time (TI to T2) (Coefficient = 11.77, 95 % CI = 3.47 - 20.60, p=0.006). In addition, a greater overall B-IFAM score in T1 was associated with a reduction in the overall B-IFAM score over time (coefficient = 15.62; 95 % CI = 7.55 - 23.69, p=0.001) ( Table 3 ). Comparison of the scores of the B-IFAM domains showed that females had a significantly greater increase in the score from T1 to T2 (more negative perception of the OHRQoL over time) than males for the aesthetic domain (p=0.034) and physical impact domain (p=0.011). As these were greater than the MCID, these differences were clinically significant. For these two domains, the effect size (the magnitude of the difference) was moderate ( Table 4 ).
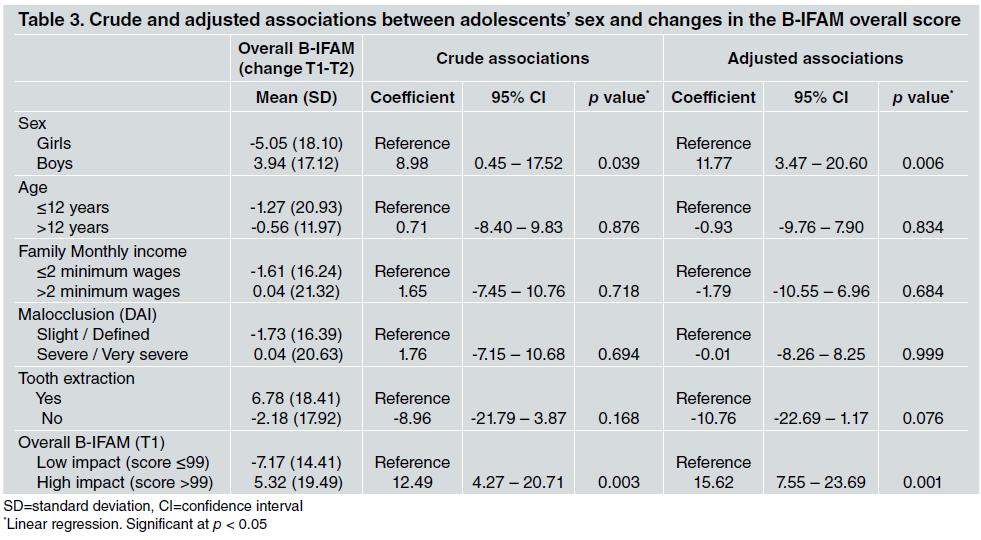
Table 3 Crude and adjusted associations between adolescents’ sex and changes in the B-IFAM overall score
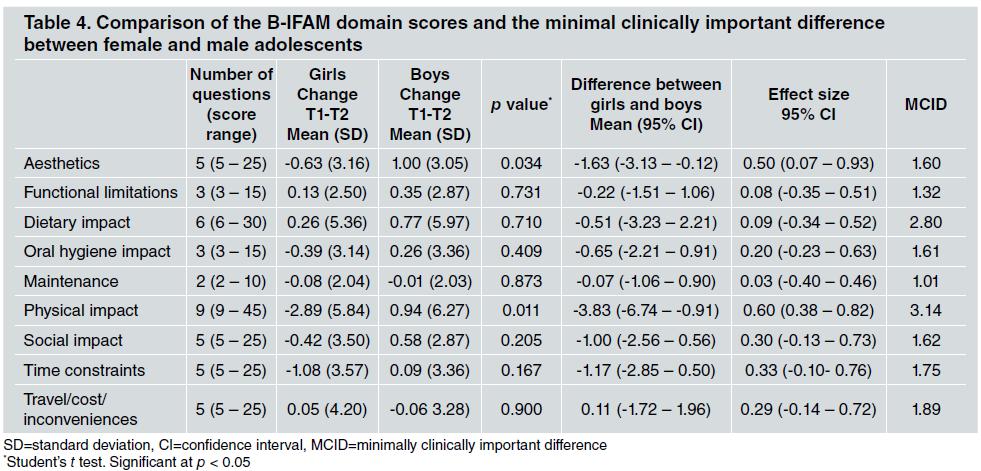
Table 4 Comparison of the B-IFAM domain scores and the minimal clinically important difference between female and male adolescents
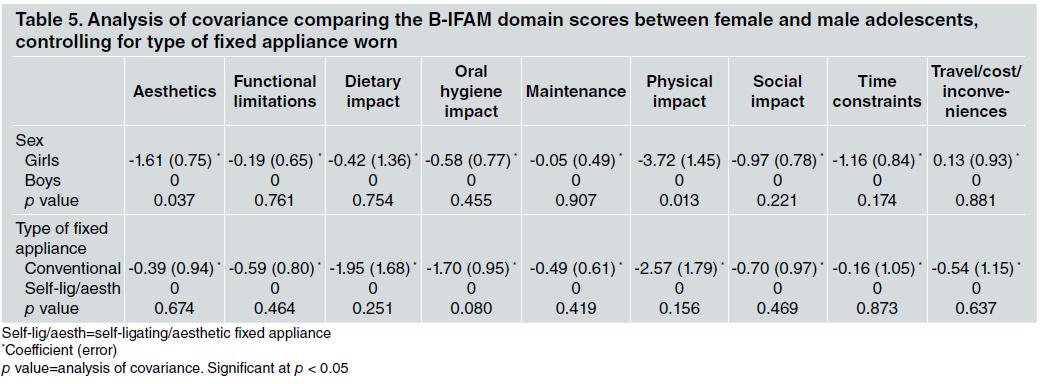
The analysis of covariance showed that the increase in the score from TI to T2 (more negative perception of the OHRQoL over time) in females than in males for the aesthetic domain (p=0.037) and physical impact domain (p=0.013) remained, regardless of the variable type of fixed appliance used ( Table 5 ).
DISCUSSION
Significant changes were found in the OHRQoL of females over the first year of orthodontic treatment with a fixed appliance. After 12 months of wearing of the fixed appliance, girls had a more negative perception of the OHRQoL than boys. The literature shows favorable effects on the OHRQoL of adolescents, regardless of sex, after the first year of wearing a fixed appliance, showing improvement in their overall OHRQoL, as a result of the strong positive repercussions on their emotional and social wellbeing 19 . However, there are no longitudinal studies comparing the difference between sexes regarding the impaet of the first year of wearing a fixed appliance on the OHRQoL. Studies that evaluated the impact of the need for orthodontic treatment and the OHRQoL of adolescents have shown that girls with occlusal disharmony have a more negative perception of their OHRQoL than boys in a similar condition. Females seem to have greater aesthetic concern and can feel more upset by dental disharmony and extremely exaggerated skeletal changes in the face 20 . Although the literatee shows that girls seek orthodontic treatment more often to correct malocclusion 20, 21 , the present study found that girls, when compared to boys, have a more negative perception of the OHRQoL between the third month and the first year of treatment with the fixed appliance. This finding illustrates that the more negative perception of the quality of life before orthodontic treatment 20, 22 seems to perpetuate itself throughout the 12 months after the fixed appliance has been installed. In the adjusted regression for the evaluated confounding variables, the girls continued to have a more negative perception of the OHRQoL throughout the orthodontic treatment with the fixed appliance, when compared to the boys. In this regard, a study conducted in 2014 evaluated the relationship between adolescents’ OHRQoL and self-esteem during the first year of orthodontic treatment. It found that adolescents with better self-esteem at the beginning of the orthodontic treatment demonstrated minimal variability in the OHRQoL after the first year of wearing a fixed appliance 23 . The differences in self-esteem between adolescents of different sexes 24 may be useful to explain how orthodontic treatment impacts their quality of life 25 . Females had a more negative perception of the OHRQoL during the first year of orthodontic treatment in the aesthetic domain. Adolescents undergoing orthodontic treatment with a fixed appliance seem to need aesthetic approval from their peers and parents. They often compare their looks to those of their friends and people on the media, and feel that their own teeth should be similar to the dental and facial aesthetic standard imposed by others 22 . The results of the present study suggest that girls feel more uncomfortable and embarrassed, and avoid smiling when wearing a fixed appliance, because they might perceive the orthodontic device as ugly.
Pain and discomfort in the oral mucosa are common complaints during orthodontic therapy. In the present study, girls reported more complaints than boys regarding pain and sores (physical impact) during the first year wearing a fixed appliance. A previous cross-sectional study using the B-IFAM questionnaire on patients in the sixth month of wearing a fixed appliance, also found differences in the perception of pain between boys and girls. It reported that girls appeared to be more anxious about the possibility of pain caused by the activation of the fixed appliance 10 . The results of the present study showed that this fear of pain caused by the activation of the fixed appliance persists in the girls even after the first year wearing it. It is important to highlight that the adolescents answer the questionnaire shortly after the dental appointment to activate the fixed appliance, which may influence the perception of pain, given that three days after activation, its perceived tension often subsides 26 .
It is important to emphasize that the statistically significant differences between girls and boys for the domains of aesthetics and physical impact appear to be clinically significant, as they were greater than the MCID. The MCID reflects the changes of a specific outcome during a specific intervention, which are expressive and significant for the patients who undergo that type of intervention. In other words, it would be the smallest difference in a given outcome considered to be beneficial and which would imply, in the absence of side effects and excessive costs, a change in the management of the patient 27 . In studies that evalúate quality of life, a significant change in the OHRQoL ís considered as one which results in a significant reduction in the symptoms or an improvement in function and wellbeing 28 , This concept helps resolve one of the greatest challenges of transforming scientific evidence into practice, which ís the interpretation of research data in the light of clinical relevance 29 . Moreover, within our results, the MCID implications were confirmed by effect size for the two domains, which were modérate to high 30 .
The results of studies on quality of life can be important to help the clinician to understand the physical, functional, and wellbeing consequences of orthodontic treatment. Based on the results of the present study, girls have a more negative perception of wearing a fixed appliance for reasons of aesthetics and probable pain and discomfort caused by the orthodontic device. Thus, early advice regarding the repercussions of orthodontic treatment should place greater emphasis on girls, to provide greater understanding of the possible complications of wearing a fixed appliance 10 to correct occlusal discrepancies, thereby improving the patient’s quality of life at the end of the treatment 31 . Moreover, it ís of utmost importance to clarify the effects of orthodontic therapy with a fixed appliance to the decision-makers, to enable improvement and better organization of the Services providing orthodontic care 9 .

