











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Dental caries (DC) is a multifactorial, dynamic, non-transmissible, biofilm-mediated, diet-modulated disease that leads to loss minerals from tooth hard tissues. It is determined by biological behavioral, psychosocial and environmental factors1. Caries experience has declined noticeably in developed countries2. However, available data suggest that the population in Argentina is far from achieving a balanced oral health status and good quality of life regarding oral health. DC mainly affects children and the elderly, with a marked social gradient and greater impact on persons with high social vulnerability3.
Until not long ago, it was assumed that the only treatment for DC was surgical, and cariology was taught accordingly, being restricted to the restoration and limitation of damage to tooth hard tissues. In recent decades, however, it has been accepted that preventive measures are also an important part of dentistry. Thus, students of dentistry need to receive thorough, systematic training in cariology.
In Europe, the Association for Dental Education in Europe (ADEE) prepared a document called “Profile and competences for the European dentist”4, describing the general competences that dentists should have.
In 2011, the European Organization for Caries Research (ORCA) published the first consensus for developing the Core Curriculum in Cariology5, which in turn provided a basis for the same to be done in Colombia in 20146, USA in 20157, Chile in 20 1 88 and the Caribbean region in 20219.
Given that in Argentina there is no consensus among public and private faculties/schools of dentistry regarding cariology contents, and no previous national process to agree upon criteria on the subject, there is a need to define the contents and competences of cariology in the curriculum for undergraduate dentistry faculties/schools in the country.
AIM
To develop a consensus document on the contents and competences of cariology in the curriculum for Argentine faculties/schools of dentistry, at undergraduate level.
MATERIALS AND METHOD
The Organizing Committee (OC) of the Cariology and Public Health Group (GCySP, by its acronym in Spanish) of the Argentine Society of Dental Research (SAIO, by its acronym in Spanish) planned the process in stages (Fig. 1).
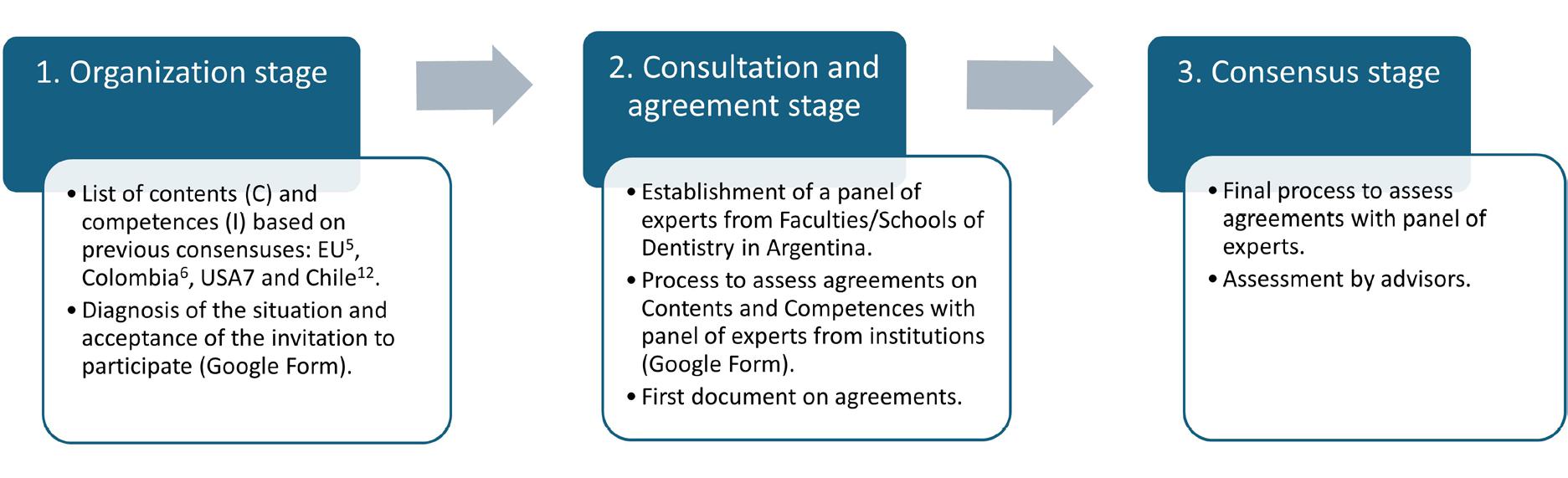
Stage 1. Diagnosis of the situation and acceptance of the invitation to particípate
The GCySP OC identified the 20 academic units that offer dentistry degrees in the Republic of Argentina (RA) and defined the list of contents and their clinical application, based on the 5 domains initially established by the European Union5, and subsequently adapted by the USA7, Colombia6, Chile8 and the Caribbean region9. The domains were defined as: 1- Basic knowledge; 2- Determination of risk, diagnosis of caries and detection of caries lesions; 3- Decision-making for non-operative/ non-surgical preventive management; 4- Decision-making for operative/surgical treatment, and 5-Evidence-based cariology in clinical practice and public health.
The OC prepared a list of all the Schools of Dentistry in the Republic of Argentina and sent a letter of invitation to the Deans, Academic Secretaries or Directors of the degrees, as relevant to each higher education institution, asking them to participate in the discussion and definition of contents and their corresponding clinical indicators. For such purpose, the people in charge of academic affairs were asked to designate cariology representatives from their respective faculties/schools. This process of invitation, constitution and consent of expert representatives lasted two months. The first step in this stage was to send a Google Form with 11 questions to identify the institution and its representative, and the cariology curriculum at each academic unit.
The purpose of this stage was to conduct an analysis within the Faculties/Schools of Dentistry on some curricular aspects of the teaching of cariology to undergraduates, and to evaluate interest in working towards a consensus for teaching cariology in Argentina.
The inclusion criterion was Academic Units with at least one graduation class.
Stage 2. Content and competence agreement assessment process
During the second stage, the first virtual workshop was organized. It took place in two phases: the first phase included a conference providing context regarding the importance of a consensus curriculum and the need to generate a list of contents and their indicators for clinical application. This conference was given by the project’s foreign advisor. During the second phase, the participants from the different academic units were distributed in a heterogeneous and balanced manner into five working groups. There were 19 participating representatives. Work was conducted on content and competence agreement assessment in the five domains: D1- Basic Sciences; D2- Dental caries risk and diagnosis; D3- Decision-making for non-invasive treatments; D4- Decision-making for invasive treatment, and D5- Evidence-based cariology at community level. Each group was assigned one domain to analyze for 40 minutes in separate virtual rooms, and the items discussed were entered into electronic forms (Google Forms). After group work, a plenary session was held during which each group presented its proposals, agreements, contributions or modifications regarding contents and indicators, as part of the feedback process.
The OC drafted the document: “Cariology in the
Curriculum of Schools of Dentistry in the Republic of Argentina”, which included the observations made at the workshop. The draft was sent to all participants, who then individually analyzed each domain, and returned the draft with or without modifications.
The purpose of this stage was to prepare a document to submit for consensus and validation of the proposal.
Stage 3. Consensus stage
During the third stage of the consensus, the second virtual workshop was held. It was a plenary session to work on the assessment of agreements with the panel of experts. Agreements and consensuses were submitted for approval or rejection to all attendees, taking into account the experience, assessment and relevance of the domains in future curricular plans. Contents and indicators were approved unanimously. The OC wrote the final document for publication, which was copyedited by members of the OC and the national and foreign advisors.
RESULTS
Stage 1
Of the total 20 forms sent to the Academic Units, 13 responses were received (65%) - 7 from National Universities in the provinces of Tucumán, Mendoza, Rio Negro, Corrientes, Santa Fe, Córdoba and Buenos Aires, and 6 privately managed universities: 3 from Buenos Aires City and 3 from the provinces of Mendoza, Córdoba and Entre Ríos (Fig. 2).

All participants agreed to be part of the consensus. Regarding analysis of whether cariology contents were adequately included in the curriculum, 84.6% of the representatives agreed. In response to the question of whether the contents were included in one or more subjects, 92.3% of the participants reported that they were included in several subjects. Learning goals in the different curricula were analyzed. Academic unit representatives identified the following contents in the basic and clinical subjects: risk-based approach (evaluation and control criteria), decisions for preventive/non-operative caries management, cariology in public health and community dentistry, evidence-based dentistry and analysis of social determinants.
All academic units identified cariology contents in the clinical subjects. However, in basic subjects, contents were variable, with 92.3% for risk-
based approach and decisions for non-operative management of caries, 76.9% for decisions for operative management, 84.6% for evidence-based dentistry and analysis of social determinants, and 76.9% for cariology and public health/community dentistry (Table 1).
Table 1 Cariology contents in curricula
| Basic Subjects | Clinical Subjects | |
| Risk-based approach | 92.30% | 100% |
| Decision-making for non-operative management of caries | 92.30% | 100% |
| Decision-making for operative management | 76.90% | 100% |
| Evidence-based dentistry | 84.60% | 100% |
| Analysis of social determinants | 84.60% | 100% |
| Cariology in public health/community dentistry | 76.90% | 100% |
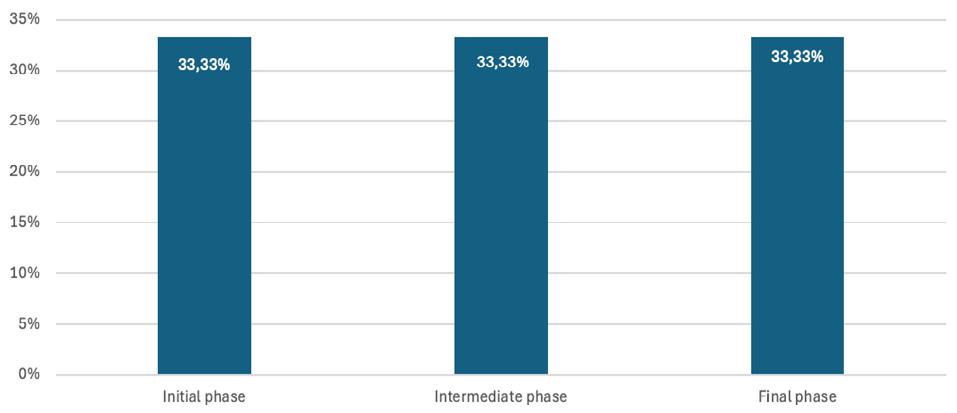
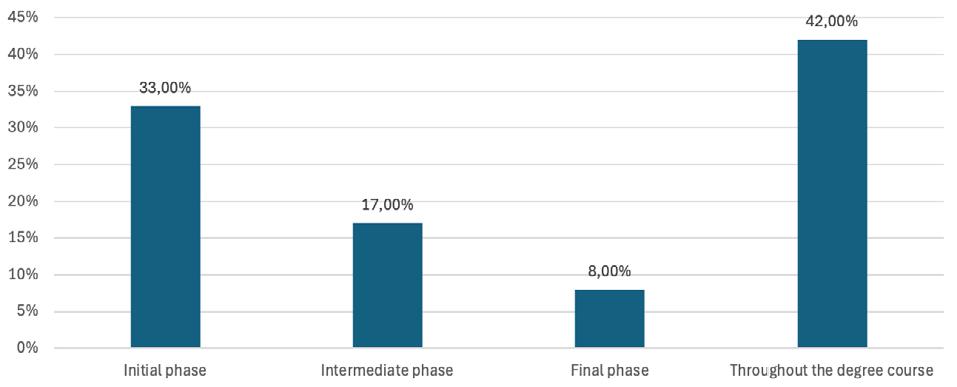
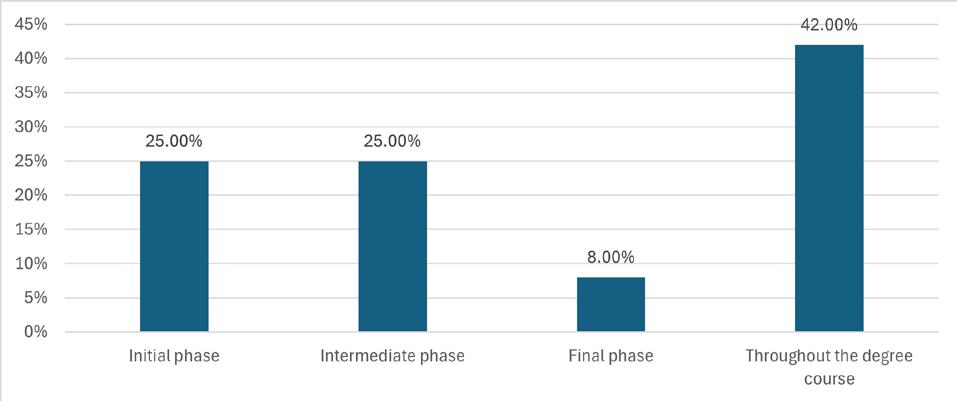
Analysis of the opinions of the academic unit representatives regarding criteria for evaluating students showed that grades were preferably given to operatory and preventive interventions. Exploration of the stage of the course of studies at which the aforementioned contents were incorporated showed that the reference people agreed that they were taught throughout the course of studies in different periods, considering 1st and 2nd year as early, 3rd and 4th year as intermediate, and 5th and 6th year as final (for 5-year courses, 5th year was taken as final, while for 6-year courses, the two last years were considered). Analysis of each content shows that risk-based approach (criteria for evaluation and control) is taught with equal intensity throughout the course of studies, i.e., during all three periods described. Decision-making for non-operative preventive management of caries is taught to an equal extent in the early and final periods of the course of studies. Evidence-based dentistry is more intensively taught during the first years (early period) and declines as the course of studies progresses. Decision-making for operative management is taught equally during the early and intermediate periods. Cariology and public health is taught almost constantly throughout the course of studies. Analysis of social determinants is taught in the early and final periods, and less intensively during the intermediate period (Fig. 3a-f)



Stages 2 and 3
With the participation of 20 representatives from 10 academic units in the country, corresponding to 50% of the Faculties/Schools of Dentistry at Universities in Argentina, the list of core contents and clinical application indicators for teaching cariology was approved unanimously.
A total 23 core contents and 31 clinical application indicators were agreed upon for teaching cariology in Argentina. The number of contents (C) and indicators (I) per domain were: Domain 1-: Basic Knowledge: 5 C and 7 I; Domain 2: Risk, Detection and Diagnosis: 6 C and 6 I; Domain 3: Decision-making for non-operative and preventive management (considering patient risk and diagnosis): 5 C and 5 I; Domain 4: Decision-making for operative treatment: 4 C and 9 I; Domain 5: Evidence-based cariology in clinical practice and public health: 3 C and 4 I (Tables 2-6).
Table 2 Domain 1. Basic knowledge: List of Contents and Indicators for clinical/community application
| DOMAIN 1 | Contents | Clinical/community application indicators |
|---|---|---|
| Basic knowledge | D1 C1 Anatomy and development of tooth tissues and support structures at macroscopic, microscopic and molecular/ionic levels | I.1 Describe, understand and analyze the development and morphology of dental and periodontal tissues |
| D1 C2 Concept of caries disease, caries lesions and non-carious lesions. Role of dental biofilm, diet, hygiene habits, saliva and progression of the disease in the individual and social context | I.2 Identify and use protocols to evaluate risk or factors associated to individual risk of the patient | |
| D1 C3 Chemical, physical and biological bases of changes in hard tissues, related to clinical and radiological detection. Evaluation of caries lesions and other non-carious lesions | I.3 Detect carious and non-carious lesions at clinical and radiographic level using a validated criterion | |
| I.4 Assess the activity of caries lesions at clinical level | ||
| D1 C4 Basic principles of professionalism: ethics, bioethics and social responsibility | I.5 Provide dental care respecting bioethical principles | |
| D1 C5 Psychological theories and techniques to change behaviors and habits in order to improve oral health. Basic tools for effective communication | I.6 Detect needs for changing behavior and habits in order to improve oral health | |
| I.7 Refer patient to a relevant health professional in a timely manner |
Table 3 Domain 2: Risk, Detection and Diagnosis: List of Contents and Indicators for clinical/community application
| DOMAIN 2 | Contents | Clinical/community application indicators |
|---|---|---|
| Risk, detection and diagnosis | D2 C1 Patient-centered diagnosis | I.8 Evaluate and integrate demographic, socio-cultural, behavioral, systemic, clinical and radiographic background to issue diagnostic judgment |
| D2 C2 Evaluation of the dental caries disease in the patient considering a life course approach | I.9 Identify and apply indicators, risk factors and prognostic factors at individual level, by determining patient social and community context, applied over time | |
| D2 C3 Evaluation of patient's systemic health and the oral effects deriving from patient's condition and/or treatments | I.10 Relate systemic diseases and their treatment to dental caries disease | |
| D2 C4 Criteria for clinical detection, severity, activity and effects of carious lesions on the pulp | I.11 Apply standardized systems for detection and clinical evaluation of carious lesions and pulp health status | |
| D2 C5 Detection and radiographic evaluation of caries lesions | I.12 Apply criteria to determine radiographic severity of caries lesions. | |
| D2 C6 Differential diagnosis of caries lesions | I.13 Apply criteria for detection and differential diagnosis of enamel and dentin effects; hypoplasia, amelogenesis imperfecta, dental crack, fluorosis, MHI, non-carious lesions (erosion, abrasion, abfraction, attrition), dental malformations, and evaluate their origin |
Table 4 Domain 3: Decision-making for non-operative and preventive management: List of Contents and Indicators for clinical/community application
| DOMAIN 3 | Contents | Clinical/community application indicators |
|---|---|---|
| Decision-making for non-operative and preventive management (consider patient risk and diagnosis) | D3 C1 Behavioral changes to promote oral health | I.14 Apply evaluation instruments associated to behavioral changes |
| D3 C2 Diet advice and monitoring. Effects of eating disorders on oral health | I.15 Identify and use instruments to evaluate and monitor diet-related behavior | |
| D3 C3 Mechanical, chemical and biological control of dental biofilm | I.16 Impart instructions on oral hygiene, monitor indicators, and define maintenance intervals. Professional removal of biofilm | |
| D3 C4 Fluorides: action mechanism, presentations and rational use according to risk level and age. | I. 17 Properly indicate, prescribe and clinically apply fluorides according to risk level and age | |
| D3 C5 Other anticaries and remineralization agents | I.18 Indicate agents other than fluoride according to risk level and age |
Table 5 Domain 4: Decision-making for operative treatment: List of Contents and Indicators for clinical/ community application
| DOMAIN 4 | Contents | Clinical/community application indicators |
|---|---|---|
| Decision-making for operative treatment | D4.C1. Rationale for minimally invasive treatment of caries lesions | I.19 Perform micro- and minimally invasive treatment on cavitated and active lesions |
| I.20 Prioritize repair and sealing of defective restorations over total replacement of the restoration | ||
| D4. C2. Designing biological preparations for the treatment of caries lesions determined according to activity, location, extension and depth | I.21 Perform minimum sufficient access to the lesion, using appropriate instruments | |
| I.22 Selectively remove carious tissue | ||
| D4. C3. Surgical management of caries lesions to ensure maintenance of oral health | I.23 Perform actions for pulp-dentin protection | |
| I.24 Perform morphological reconstruction of proximal contacts, dental contours, surface texture and functional occlusal contacts | ||
| D4. C4. Implementation of individual control and maintenance programs according to evaluation of risk and prognosis | I.25 Determine risk and prognosis at individual and/or community level | |
| I.26 Establish frequency for control and maintenance according to individual risk level, considering patient's community context | ||
| I.27 Apply control program in maintenance patients and monitor them |
Table 6 Domain 5: Evidence-based cariology in clinical practice and public health practice: List of Contents and Indicators for clinical/community application
| DOMAIN 5 | Contents | Clinical/community application indicators |
|---|---|---|
| Evidence-based cariology in clinical and public health practice | D5. C1. Development of programs for promotion, prevention y maintenance of oral health | I.28 Know, design and apply programs for promotion, prevention and maintenance of oral health |
| D5. C2. Epidemiology of caries in relation to determining factors of health | I.29 Use the qualitative and quantitative tools for epidemiology | |
| D5. C3. Base clinical tasks on the available scientific evidence | I.30 Apply the concepts of dentistry based on available scientific evidence | |
| I.31 Apply validated clinical guides for managing dental caries |
DISCUSSION
The list of cariology contents for the degree, as defined in Argentina, aligns with the six previous consensuses, with the basis provided by European consensus (European core curriculum in cariology, 2011)5 prepared by the ADEE (Association for Dental Education in Europe) and ORCA (European Organisation for Caries Research) and 75 participants invited from 24 European countries and three countries in North and South America. The following consensuses were subsequently developed: Colombia (2014), Chile (2018), and
Caribbean (2021) in LAC, in the USA (2016) and in Spain (2020). These documents propose 5 domains in the teaching of cariology, arranged in Principal and Specific Competences. These curricula focus on competences, whereas our consensus analyzed core contents.
In Argentina, there is a broad range of sociodemographic conditions, and the academic units are distributed according to the situation in each region. In the Northwest region, both La Rioja and Tucumán Provinces have a public university.
In the Northeast región, in Corrientes City, there is only one public university. The provinces of Córdoba, Santa Fe and Mendoza each have both a public and a private university. Entre Ríos Province has only one private university, while Buenos Aires Province has one public and two private universities. The Autonomous City of Buenos Aires has one public and five prívate universities. In the Patagonian region, Río Negro Province has one public university. A study conducted at some schools of dentistry in Latin America describes cariology as part of the curricula but reports high variability in terms of planning and achievements10.
During the discussion of this proposal, none of the contents was discarded. However, some of the contents were combined because they addressed knowledge, skills and behaviors in common. The items which were most discussed were the contents associated to the concept of caries disease, caries lesions and non-carious lesions. The role of dental biofilm, diet, saliva and disease progression (D1-C2), mechanical, chemical and biological control of dental biofilm (D3-C3), and implementation of control and maintenance programs according to evaluation of risk and prognosis (D4-C4) pose a challenge to dental student training. During the plenary session, discussion and reflection addressed a range of factors such as changes in prevalence of the disease, development of materials and technology, and competences for managing behavioral and communicational variables, establishing the possibility of achieving a student/professional who is competent in planning intervention strategies in the community in order to act upon what has been diagnosed. There was general agreement on the need for the curriculum to develop competences in risk evaluation, preventive management of caries lesions, and the way in which this knowledge is applied at individual and community levels.
In agreement with León et al.11 and Giacaman et al.12, the main advantages of this proposal for contents and indicators are its flexibility and the gradual insertion of contents across the degree. It can thus be included in the curricula of different educational models - both competence-based and learning outcome- or objective-based. Indeed, the core contents in the consensus need not be delivered exclusively through a single subject, but may be distributed over the curricular network as content in various subjects. The contents may be included in the three learning cycles: basic, pre-clinical and clinical, and their indicators enable evaluation of the transfer of theoretical content to clinical practice.
CONCLUSIONS
Cariology contents for undergraduates at both public and private faculties/schools of dentistry in the Republic of Argentina refer to the learning objectives expressed in the different subjects across the curriculum. To conclude, an unprecedented consensus in Argentina was able to lay out the core contents and clinical application indicators for cariology for undergraduate students at universities across the country, providing an important contribution to quality education in dentistry.

