










Serviços Personalizados
Journal

Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista argentina de cirugía
versão impressa ISSN 2250-639Xversão On-line ISSN 2250-639X
Rev. argent. cir. vol.111 no.2 Cap. Fed. jun. 2019
CARTA CIENTÍFICA | SCIENTIFIC LETTER
Quiste de conducto cístico
Cystic duct cyst
Enrique Petracchi, Nicolás Baglietto, Juan I. Rico, Carlos Canullán
División Cirugía General HGA Dr. Cosme Argerich. Buenos Aires. Argentina.
Correspondencia | Correspondence: Enrique Petracchi E-mail: petracchi@hotmail.com
Los autores declaran no tener conflictos de interés.
Conflicts of interest None declared.
http://dx.doi.org/10.25132/raac.v111.n1.1389.es
Recibido | Received 23-06-18
Aceptado | Accepted 29-10-18
Resumen
Los quistes congénitos de la vía biliar son infrecuentes y se definen por la dilatación quística del árbol biliar en cualquiera de sus porciones. Los quistes del conducto cístico son aún menos frecuentes. Su etiología permanece incierta y el tratamiento consiste en la resección debido a su potencial desarrollo de malignidad. Presentamos el caso de una paciente en la que se diagnosticó dilatación del conducto cístico y fue tratada por vía laparoscópica.
Palabras clave: Quiste congénito; Conducto cístico; Biliar.
Abstract
Congenital biliary duct cysts are rare and are defined as cystic dilatations of the biliary tree in any of its portions. Cystic duct cysts are more uncommon. Their etiology remains uncertain and they should be resected due to the possible development of malignancy. We report the case of a female patient with a diagnosis of dilation of the cystic duct that was treated with laparoscopic surgery.
Keywords: Congenital cyst; Cystic duct; Biliary.
Los quistes congénitos de la vía biliar son infrecuentes y se definen por la dilatación quística del árbol biliar en cualquiera de sus porciones. Usualmente se diagnostican antes de los 14 años, aunque hasta un 20% pueden encontrarse en adultos. La relación mujerhombre es de 4:11. Su etiología permanece incierta y el tratamiento consiste en la resección debido a su potencial desarrollo de malignidad. La dilatación aislada del conducto cístico es una entidad extremadamente infrecuente. Una paciente de 19 años de edad es derivada a nuestro Servicio con el antecedente de colecistectomía laparoscópica 6 meses atrás por un cuadro de colecistitis, con el hallazgo en la colangiografía intraoperatoria (CIO) de dilatación quística de la vía biliar interpretada por el cirujano como tipo II de la clasificación de Todani. No presenta otros antecedentes médicos ni quirúrgicos de importancia. La anatomía patológica de la vesícula reveló colecistitis crónica. El examen físico es normal y los exámenes de laboratorio no tienen parámetros de colestasis.
Imágenes: se le realiza como primer estudio una ecografía abdominal y se observa una imagen hipoecogénica de aproximadamente 3 × 4 cm con ecos en su interior compatibles con microlitiasis múltiple. Las vías biliares intrahepática y extrahepática no se encuentran dilatadas. La colangiorresonancia magnética (CRMN) muestra ausencia de la vesícula biliar y dilatación aislada del conducto cístico con microlitiasis. El resto de la vía biliar y la unión biliopancreática no presentan alteraciones. Se interpreta como quiste de vía biliar tipo VIa (Fig. 1).

Figura 1. CRMN que muestra dilatación quística del conducto cístico con litos en su interior (cabeza de flecha). Indemnidad de la convergencia biliopancreática (flecha).
Tratamiento: se planifica la resección laparoscópica. Colocamos cuatro trocares en ubicación habitual para colecistectomía. Se liberan adherencias previas hasta lograr identificar los clips del conducto cístico. Una vez identificados, realizamos CIO que muestra la dilatación quística del conducto cístico con imágenes negativas en su interior e indemnidad del resto de la vía biliar, sin imágenes litiásicas y con buen pasaje a duodeno. Interpretando la lesión como un quiste tipo VIa, ligamos el cuello del quiste en su unión con la vía biliar principal con nudo extracorpóreo de PDS tipo endoloop (Fig. 2) y resecamos el quiste. Enviamos el margen distal a anatomía patológica para su congelación informándolo como epitelio biliar sin displasia. El quiste se extrae en bolsa por el puerto de 10 mm.
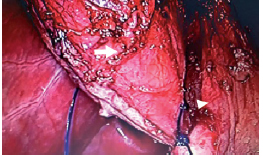
Figura 2. Ligadura del cuello del quiste. Quiste cístico (flecha). Vía biliar principal (cabeza de flecha).
Evolución posoperatoria satisfactoria. Externación a las 24 horas con tolerancia a dieta y deambulación. La anatomía patológica diferida informa “inflamación crónica, fibrosis subserosa y metaplasia enteral y pseudopilórica focal. También se observan múltiples formaciones litiásicas”. En el seguimiento de 2 años, la paciente continúa asintomática. Los quistes de colédoco fueron clasificados originalmente por Alonso-Lej en el año 1959 en 3 tipos de acuerdo con su localización y morfología. Todani y col. ampliaron la clasificación en 1977 a 5 tipos. Esta última es la más difundida actualmente; sin embargo, Serradel y col., en 1991, sugirieron una nueva variedad de quistes no incluidos en ella, que son los quistes aislados del conducto cístico y los llamaron tipo VI2. Más recientemente, Rohit y col. ampliaron la clasificación en tipo VIa a aquellos en los que la dilatación es solo del conducto cístico y tipo VIb a aquellos en los que se encuentran dilatados el conducto cístico y el colédoco3. La ampliación de la clasificación de Todani sería un tema para evaluar tal como lo sugieren estos autores2,4. Los quistes de colédoco son infrecuentes (1 caso cada 100 000-150 000) y, entre estos, los quistes aislados de conducto cístico (tipo VI) son aún menos frecuentes: se han informado solamente 21 casos en la literatura hasta el momento, según nuestro conocimiento. Las únicas publicaciones que existen acerca de esta patología son informes de casos. Este tipo de quistes suelen ser diagnosticados en el intraoperatorio y algunas veces confundidos con quistes tipo II de la clasificación de Todani debido a su apariencia similar5,6.
El tratamiento de estas lesiones consiste en la resección quirúrgica por el posible desarrollo de malignidad. La razón del posible desarrollo de cáncer sobre estas lesiones parecería deberse a reflujo de líquido pancreático debido a anormalidad en la desembocadura en la unión biliopancreática. La anormalidad en la desembocadura biliopancreática como etiología de los quistes tipo VI y su posible desarrollo de malignidad son cuestiones aún por esclarecer. Cabe destacar que, de todos los casos de quistes del conducto cístico que han sido publicados, solo uno presentaba anormalidad en la unión biliopancreática. Existen, según nuestro conocimiento, solamente 21 casos publicados en la literatura de habla inglesa, y solo 3 fueron abordados por vía laparoscópica. Nuestro caso muestra que la resolución por vía laparoscópica es factible; esto resulta más fácil en los quistes tipo VIa y, entre estos, en aquellos en los que el cuello del conducto cístico en su unión con el colédoco es fino y pueden colocarse clips o ligarse. En estas situaciones, la cirugía es similar a la que se realiza para los quistes tipo II de la clasificación de Todani. El abordaje por cirugía abierta adoptado en la mayoría de los casos publicados parecería deberse a error diagnóstico y a la falta de entrenamiento para realizar una derivación biliodigestiva por laparoscopia.
English version
Congenital biliary duct cysts are rare and are defined as cystic dilatations of the biliary tree in any of its portions. They are usually diagnosed before the age of 14, but may be found in adults in up to 20% of cases, with a female to male ratio of 4:11. Their etiology remains uncertain and they should be resected due to the possible development of malignancy. The isolated dilation of the cystic duct is extremely uncommon. A 19 year-old female patient was referred to our service. She had undergone laparoscopic cholecystectomy six months before with a diagnosis of cholecystitis. The intraoperative cholangiography showed a cystic dilation of the bile duct that was interpreted by the surgeon as a type II bile duct cyst of the Todani classification. She did not have history of other significant medical or surgical conditions. The pathological examination of the gallbladder revealed chronic cholecystitis. Physical examination and liver panel were normal.
Image tests: the abdominal ultrasound showed a hypoechogenic image measuring 3 x 4 cm filled with echoes suggestive of multiple microscopic gallstones. The intrahepatic and extrahepatic bile ducts were not dilated. The magnetic resonance cholangiopancreatography (MRCP) demonstrated absence of the gallbladder and isolated dilation of the cystic duct with microscopic gallstones. The rest of the bile ducts and the pancreaticobiliary junction were normal. A diagnosis of type VIa bile duct cyst was made (Fig. 1).
Figure 1. Magnetic resonance cholangiopancreatography showing cystic dilation of the cystic duct with gallstones inside (arrowhead). The pancreaticobiliary junction is normal (arrow).
Treatment: laparoscopic resection was scheduled. Four trocars were placed in the usual position for cholecystectomy. After releasing previous adhesions, the cystic duct clips were identified. Then, we performed intraoperative cholangiography which showed the cystic dilation of the cystic duct with negative images inside. The rest of the bile ducts were normal, without gallstones and adequate passage of the contrast the agent to the duodenum. We interpreted that the lesion was a type VIa cystic duct. The neck of the cyst was ligated in the junction with the main bile duct with and extracorporeal knot of PDS (as an endoloop) (Fig. 2) and the cyst was resected. Frozen section biopsies of the distal margin were analyzed and were reported as biliary epithelium without dysplasia. The cyst was removed with an endoscopic bag through the 10-mm port.
Figure 2. Ligation of the neck of the cyst. Cystic duct cyst (arrow). Main bile duct (arrowhead).
The postoperative outcome was satisfactory and the patient was discharged 24 hours after surgery tolerating solid food and being able to walk. The pathological examination reported chronic inflammation, subserous fibrosis, focal intestinal and pseudopyloric metaplasia and multiple gallstones. After two years of follow-up, the patient remains asymptomatic. Choledocal cysts were initially classified by Alonso-Lej in 1959 in three types, according to their location and morphology. In 1977, Todani et al. divided choledochal cysts into five groups. This classification is the most used currently; however, in 1991 Serradel et al. proposed that isolated cystic duct cysts, a new type of biliary cyst, should be included as type VI lesions in the Todani’s classification6. More recently, Rohit et al. proposed that type VI cysts should be further divided into two types: type VIa involving isolated dilatation of the cystic duct and type VIb involving combined dilatation of cystic duct as well as the common bile duct3. The inclusion of these varieties of the Todani’s classification would a matter of evaluation as these authors suggested2,4. Choledocal cysts are rare, with an incidence of between 1 in 100,000 and150,000) and isolated cystic duct cysts are even rarer; as far as we know, only 21 cases have been reported in the literature. These cysts have been only described in case reports and are generally diagnosed during surgery and sometimes diagnosed as type II cysts of the Todani classification due to their similar appearance5,6.
These lesions should be resected due to the possible development of malignancy. The reason for the possible development of cancer on these lesions would be due to reflux of the pancreatic secretion into the biliary tract due to an anomalous pancreaticobiliary junction. The association of anomalous pancreaticobiliary junction with type VI cystic duct cysts and biliary tract malignancy is still unclear. Of importance, among all the published cases of cystic duct cyst, only one presented an anomalous pancreaticobiliary junction. As far as we know, there are only 21 case reports published in English, and only three 3 were approached with laparoscopy. Our case shows that resolution by laparoscopy is feasible; this is easier in type VIa cysts and, among these, in those in which the neck of the cystic duct at its connection with the common bile duct is thin and can be clipped or ligated. In these situations, the surgery is similar the one performed for type II cysts of the Todani classification. The open surgery approach used in most of the published cases seems to be due to misdiagnosis and lack of training to perform laparoscopic biliodigestive bypass.
Referencias bibliográficas | References
1. Nambiar L, Alex A, Siskind E, Shen AW, Fan C, Grimaldi G, et al. Type VI choledochal cyst-an unusual presentation of jaundice. Int J Angiol. 2016; 25:263-5. [ Links ]
2. Serena Serradel AF, Santamaría Linares E, Herrera Goepfert R. Cystic dilatation of the cystic duct: a new type of biliary cyst. Surgery. 1991; 109:320-2. [ Links ]
3. Rohit B, Shikha S. A variant of type VI choledochal cyst: combined dilatation of cystic duct and common bile duct. J Ultrasound. 2016; 19:71-2. [ Links ]
4. Shah OJ, Shera A, Shah P, Robbani I. Cystic dilatation of the cystic duct: a type 6 biliary cyst. Indian J Surg. 2013; 75:S500-2. [ Links ]
5. Samrat R, Bharath K. Isolated dilatation of the cystic duct-Type VI choledochal cyst: a rare case presentation and review of the literature. J Surg Case Reports. 2017; 4: 1-4. [ Links ]
6. Loke TK, Lam SH, Chan CS. Choledochal cyst: an unusual type of cystic dilatation of the cystic duct. AJR Am J Roentgenol. 1999; 173:619-20. [ Links ]

