










Servicios Personalizados
Revista

Articulo
 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista argentina de cirugía
versión impresa ISSN 2250-639Xversión On-line ISSN 2250-639X
Rev. argent. cir. vol.111 no.2 Cap. Fed. jun. 2019
IMAGEN EN CIRUGÍA | IMAGES IN SURGERY
Vólvulo gástrico
Gastric volvulus
Micaela Mandacen1, Martín Varela Vega2, Fabio Madera2
1 Servicio de Imagenología. Hospital de Clínicas. UDELAR. Montevideo. Uruguay.
2 Servicio de Cirugía Esófago Gástrica. Hospital Central de las Fuerzas Armadas. Montevideo. Uruguay.
Los autores declaran no tener conflictos de interés.
Conflicts of interest None declared.
Correspondencia | Correspondence: Martín Varela Vega E-mail: martinvarelav@gmail.com
http://dx.doi.org/10.25132/raac.v111.n1.1373.es
Recibido | Received 16-07-18
Aceptado | Accepted 23-10-18
Presentamos el caso de una paciente de sexo femenino de 81 años con un aceptable estado general, que consulta en la emergencia por dolor abdominal tipo cólico intenso acompañado de vómitos profusos de todo lo ingerido, sin bilis, de 5 días de evolución. Como antecedentes relevantes, la paciente refiere episodios similares en los últimos dos años, y ser portadora de una hernia hiatal.
Al examen se nota una paciente deshidratada, dolorida, con taquicardia y distensión abdominal asimétrica, con predominio del abdomen superior. La sonda nasogástrica obtiene líquido de retención gástrico con ausencia de bilis.
La tomografía computarizada (TC) muestra en el topograma dos imágenes radiolúcidas en continuidad, una a nivel del epigastrio y otra a nivel del hemitórax izquierdo formado una imagen en reloj de arena. Corresponde al cuerpo gástrico francamente distendido en situación infradiafragmática, y por encima del diafragma al fundus gástrico contenido dentro de la hernia hiatal. Se observa la porción distal de la sonda nasogástrica dentro del estómago distal (Fig. 1). En la reconstrucción sagital oblicua se observa la hernia hiatal paraesofágica en su pasaje transdiafragmático (Fig. 2).
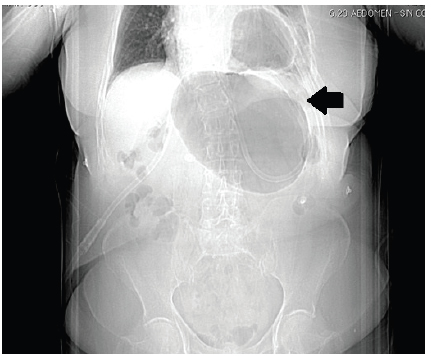
Figura 1. TC. (topograma): se identifica la silueta gástrica en reloj de arena, con gran distensión infradiafragmática, compatible con vólvulo gástrico (flecha negra). En su interior se visualiza la sonda nasogástrica

Figura 2. TC de tórax y abdomen sin contraste intravenoso (iv). Reconstrucción sagital oblicua. Hernia hiatal paraesofágica (flecha negra)
No hay engrosamiento parietal o tumoraciones en la zona de transición píloro- duodenal que hagan sospechar una compresión tumoral intrínseca o extrínseca.
En la pared gástrica se pueden ver pequeñas burbujas aéreas sugestivas de neumatosis parietal, e indicadoras de sufrimiento isquémico del mismo. El diagnóstico presuntivo es de vólvulo gástrico, y la fibrogastroscopia de urgencia lo confirma.
Se realiza la reposición hidroelectrolítica y se procede a realizar la cirugía de urgencia, con el doble objetivo del tratamiento integral de la hernia hiatal y del vólvulo gástrico, a fin de evitar recidivas.
Dado que la paciente está hemodinámicamente estable y no presenta dolor de tipo perforativo, se decide efectuar procedimiento por vía laparoscópica.
Se realiza la reducción del estómago a la cavidad abdominal y su devolvulación, así como la resección del saco herniario y cierre de los pilares diafragmáticos.
Dado que el estómago no presenta áreas de necrosis ni perforación, se decide realizar una gastropexia anterior fijándolo con puntos separados de sutura irreabsorbible al peritoneo anterolateral de la cavidad abdominal, a fin de evitar futuras volvulaciones. Cirugía de 90 minutos de duración. Luego, la paciente pasa a sala de cirugía general, con buena evolución posterior, y a las 24 horas ya tolera líquidos. Alta al cuarto día. A los tres meses se realiza estudio contrastado de esófagogastroduodeno que muestra el estómago enteramente en la cavidad abdominal, sin recidiva de la hernia hiatal.
English version
We report the case of an 81 year-old female patient who visited the emergency department due to intense colicky abdominal pain that started five days before, accompanied by nonbilious vomiting after eating. Her general status was acceptable. She had a history of hiatal hernia and reported similar episodes over the past two years.
On physical examination, the patient had signs of dehydration and complaint of pain; she presented tachycardia and asymmetrical abdominal bloating, particularly in the upper abdomen. Nonbilious gastric retention fluid was drained from the nasogastric tube.
The computed tomography (CT) scanogram showed two continuous radiolucent images, one at the level of the epigastrium and another at the level of the left hemithorax, forming an hourglass image which corresponded to the distended body of the stomach below the diaphragm, and to the gastric fundus contained within the hiatal hernia above the diaphragm.
The distal portion of the nasogatric tune was observed inside the distal stomach (Fig. 1). The oblique sagittal reconstruction showed the paraesophageal hernia passing through the diaphragm (Fig. 2). The absence of wall thickening or tumors in the transition area between the pylorus and the duodenum ruled out the presence of intrinsic or extrinsic tumoral compression.
CT. (scanogram): an hourglass stomach is identified, with significant distension below the diaphragm, suggestive of gastric volvulus (black arrow). The nasogastric tube is identified inside the stomach.
CT scan of the thorax and abdomen without intravenous contrast. Oblique sagittal reconstruction. Paraesophageal hernia (black arrow)
Small air bubbles were seen along the gastric wall suggestive of pneumatosis, indicating gastric ischemia. The presumptive diagnosis was gastric volvulus and was confirmed by urgent upper gastrointestinal endoscopy.
Fluid and electrolyte therapy was started and surgery was performed on an urgent basis to treat the hiatal hernia and the gastric volvulus to prevent recurrences.
As the patient was hemodinamically stable and did not present pain suggestive of perforation, a laparoscopic approach was used. The procedure included reduction of the stomach to the abdomen, reduction of the volvulus, resection of the hernia sac and closure of the diaphragmatic pillars. As the stomach did not present areas of necrosis or perforation, an anterior gastropexy was performed suturing the stomach to the anterolateral peritoneum of the abdominal cavity with separate stitches of nonabsorbable suture in order to avoid future recurrences.
Operative time was 90 minutes. Then, the patient was admitted to the surgical ward and presented favorable outcome, tolerating oral fluids 24 hours later. She was discharged on postoperative day 4. Three months later.
An upper gastrointestinal series showed the entire stomach in the abdominal cavity with no recurrence of the hiatal hernia.

