










Services on Demand
Journal

Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista argentina de cirugía
Print version ISSN 2250-639XOn-line version ISSN 2250-639X
Rev. argent. cir. vol.111 no.4 Cap. Fed. Dec. 2019
CARTA CIENTÍFICA | SCIENTIFIC LETTER
Endometriosis del apéndice cecal como causa de dolor abdominal crónico y masa apendicular
Appendiceal endometriosis as a cause of chronic abdominal pain and appendiceal mass
José A. Acevedo, Julio G. Caballero, Patricia M. Cabaleiro, Cecilia S. Aiello, Martín Córdoba, Matías Pesquín
Servicio de Cirugía General â Policlínico Neuquén. Neuquén. Argentina.
Cátedra de Medicina II y Cirugía â Facultad de Ciencias Médicas Universidad Nacional del Comahue. Neuquén. Argentina.
Correspondencia Correspondence: José A. Acevedo E-mail: drjosealbertoacevedo@gmail.com
Los autores declaran no tener conflictos de interés.
Conflicts of interest None declared.
http://dx.doi.org/10.25132/raac.v111.n4.1425es
Recibido | Received 28-02-19
Aceptado | Accepted 21-05-19
RESUMEN
Presentamos el caso de una paciente en edad reproductiva con dolor abdominal crónico y antecedente de endometriosis pelviana. Los estudios por imágenes muestran masa en topografía apendicular. Se decidió exploración laparoscópica programada y se realizó la resección del tumor apendicular. La anatomía patológica mostró endometriosis del apéndice cecal. Posteriormente se realiza una revisión bibliográfica de esta patología y se hacen consideraciones sobre su frecuencia, presentación clínica, hallazgos intraoperatorios, forma de estudio y posibilidades terapéuticas.
Palabras clave: Apéndice cecal; Dolor abdominal; Endometriosis.
ABSTRACT
We report the case of a female patient in childbearing age with chronic pain and a history of pelvic endometriosis. The image tests showed the presence of a mass at the level of the cecal appendix. The patient underwent a scheduled diagnostic laparoscopy and the appendiceal tumor was resected. The pathological examination revealed appendiceal endometriosis. We performed a review of the literature and made considerations about its prevalence, clinical presentation, interoperative findings, diagnostic tests and therapeutic management.
Keywords: Cecal appendix; Abdominal pain; Endometriosis.
La endometriosis del apéndice cecal es una patología poco frecuente que puede presentarse en el contexto de una endometriosis pelviana con compromiso apendicular, o en forma aislada (solo compromiso endometriósico del tracto intestinal). También puede hacerlo como una masa apendicular que simule patología neoplásica, lo que obliga a revaluar nuestra conducta en la interpretación de la clínica, la forma de estudio, los hallazgos intraoperatorios y la terapéutica elegida.
Presentamos el caso de una paciente de sexo femenino, de 34 años, con dolor crónico en cuadrante inferior derecho del abdomen, sin otros síntomas asociados y antecedentes de endometriosis peritoneal. Examen físico: dolor en cuadrante inferior derecho del abdomen, sin defensa ni peritonismo. Laboratorio normal. Ecografía: imagen quística en fosa ilíaca derecha, con sugerencia de completar estudios. Tomografía computarizada: en topografía del apéndice cecal, formación hipodensa de contornos ligeramente lobulados que mide 5 Í 3 Í 3 cm: probable mucocele apendicular, sin descartar otras etiologías (Fig. 1). La resonancia magnética nuclear no aporta datos.
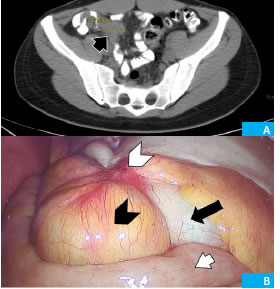
Figura 1. A: TC. Estructura sólido quística en zona apendicular (flecha corta negra). B: Campo operatorio, tumor apendicular (cabeza de flecha negra), ciego (flecha larga negra), íleon (flecha corta blanca), foco endometriósico (cabeza de flecha blanca).
Ante diagnóstico de tumor de apéndice cecal (con alta sospecha de endometriosis apendicular) se decide su exploración laparoscópica en forma electiva. De común acuerdo con la paciente (quien es médica) se decidió realizar biopsia por congelación solo si el aspecto macroscópico lo justificaba, esperar el estudio anátomo-patológico diferido y proceder posteriormente según correspondiera.
La laparoscopia muestra focos endometriósicos en peritoneo pelviano, peritoneo diafragmático, en íleon terminal y en mesenterio. Se ve una masa (sin inflamación aguda ni compromiso peritoneal) que involucra todo el apéndice, y que mide aproximadamente 4 cm de longitud por 2 cm de ancho, con focos endometriósicos en su peritoneo (véase Fig. 1). Se plantean distintos diagnósticos intraoperatorios. Ante la alta probabilidad de estar en presencia de un endometrioma apendicular (con base apendicular no comprometida), se decide realizar apendicectomía laparoscópica según técnica habitual.
Buena evolución posoperatoria y alta hospitalaria a las 24 horas posquirúrgicas.
El estudio anatomopatológico muestra: macroscopia: apéndice cecal de 3 Í 1,5 cm. Serosa congestiva. Al corte, obliteración de la luz a nivel distal. Microscopia: apéndice cecal con serosa congestiva. Paredes con hipertrofia muscular lisa que engloba glándulas endometriales rodeadas por estroma citógeno, obliterando totalmente la luz a nivel distal. Diagnóstico: endometriosis apendicular (Fig. 2).

Figura 2. Patología. A: Macroscopía. B: Microscopía. Hipertrofia muscular lisa (flecha corta negra), glándulas endometriales rodeadas por estroma citógeno (cabeza de flecha negra).
La paciente es controlada por el Servicio de Ginecología con tratamiento específico para su endometriosis peritoneal.
La endometriosis apendicular es una patología poco frecuente. Arif Emre y col. publicaron (2013) una revisión retrospectiva de 1255 piezas de apendicectomías (operados con diagnóstico clínico de apendicitis aguda, excluyendo otros diagnósticos). Encontraron solo dos casos de endometriosis apendicular (0,15%, siendo el 0,36% considerando la población femenina: 543). En esta serie, 88 pacientes no presentaban apendicitis. De estos, los dos casos de endometriosis apendicular constituyen el 2,27%.1.
Dincel y col., en 2017, en una revisión de 1970 piezas (por diagnóstico de apendicitis aguda), encontraron 59 pacientes con hallazgos inusuales (no apendicitis). En este grupo, encontraron solo una endometriosis apendicular (0,05% del total de las piezas, 1,69% de las piezas donde el diagnóstico fue distinto de apendicitis aguda)2.
En 2014, Hakan Guven y col. comunicaron el análisis de 48 pacientes sometidos a hemicolectomía derecha por masas cecales (imitando apendicitis aguda), entre los que encontraron 2 casos de endometriosis apendicular (4,16%). Estos dos casos fueron interpretados macroscópicamente como parte de 16 pacientes en los que de entrada se sospechó malignidad3.
El diagnóstico preoperatorio de endometriosis apendicular es muy dificultoso, sobre todo en aquellas pacientes en las cuales la presentación clínica resulta poco clara. Si bien se han sugerido protocolos de estudio sobre todo para pacientes que se saben portadoras de endometriosis pelviana, como la evaluación adicional de imágenes de resonancia magnética nuclear para detectar focos de endometriosis extrapélvica intestinal4, el diagnóstico preoperatorio de certeza aún es dificultoso( la mayoría de las veces se alcanza por estudio anatomopatológico de la pieza quirúrgica)1-3.
La situación en la cual la paciente es intervenida quirúrgicamente es variable: desde una exploración laparoscópica por dolor abdominal crónico, pasando por la exploración por clínica de apendicitis aguda, hasta la resección de masas tumorales en cuadrante inferior derecho del abdomen. Por lo tanto, la conducta terapéutica se debe adecuar a los hallazgos intraoperatorios, yendo desde la apendicectomía hasta las resecciones intestinales en grado variable, sobre todo en los casos de sospecha de patología maligna.
Algunos autores abogan por la apendicectomía de rutina en mujeres con dolor abdominal recurrente inexplicable durante una laparoscopia diagnóstica (sabiendo que la endometriosis puede afectar el tracto gastrointestinal sin la participación de órganos reproductivos)5, 6. Esta conducta estaría más justificada en pacientes con endometriosis y dolor pélvico crónico, mostrando que mujeres con endometriomas ováricos y endometriosis profunda infiltrante del tracto intestinal tienen tasas más altas de endometriosis apendicular. Incluso podría prevenir futuras apendicitis secundarias a la endometriosis apendicular6.
Ante la presencia de masas apendiculares y sospecha de neoplasia está indicado realizar resecciones mayores3.
ENGLISH VERSION
Appendiceal endometrosis is a rare condition presenting either in the setting of pelvic endometriosis with involvement of the appendix, or isolated within bowel involvement. It can also appear as an appendiceal mass mimicking a neoplasm, which requires re-evaluating the interpretation of the clinical signs, which tests to order, the intraoperative findings and therapeutic management.
We report the case of a 34-year-old female patient with chronic pain in the lower right quadrant of the abdomen with no other symptoms and a history of peritoneal endometriosis. On physical examination, the lower inferior right quadrant of the abdomen was painful, soft and without defense or peritoneal signs. The laboratory tests were normal. The abdominal ultrasound revealed the presence of a cystic image in the right iliac region. The computed tomography scan showed a hypodense formation at the level of the cecal appendix with slightly lobulated borders measuring 5 Í 3 Í 3 cm that was suggestive of an appendiceal mucocele, without ruling out other etiologies (Fig. 1). The magnetic resonance imaging scan did not provide additional information.
Figure 1. A: CT. Solid cystic structure in appendicular area (short black arrow). B: Operative field, appendicular tumor (black arrow head), cecum (long black arrow), ileum (white short arrow), endometriosis focus (white arrow head).
With the diagnosis of appendiceal tumor (with high suspicion of appendiceal endometriosis), a diagnostic laparoscopy was scheduled. The patient (who is a doctor) agreed to undergo frozen section biopsy only if the macroscopic appearance of the tumor was suggestive of malignancy, and to proceed accordingly once the pathology report was ready.
The laparoscopy showed foci of endometriosis in the pelvic peritoneal cavity, diaphragmatic peritoneum, terminal ileum and mesentery. A mass of about 4 cm in length by 2 cm in width was seen involving the entire appendix, with foci of endometriosis within its peritoneum. There were no signs of acute inflammation or peritoneal involvement (Fig. 1). Several differential diagnosis emerged during the procedure. In view of the high probability of appendiceal endometriosis (without involvement of the base of the appendix), laparoscopic appendectomy was performed with the usual technique.
The postoperative period was uneventful and the patient was discharged 24 hours after the procedure.
The macroscopic pathological examination reported that the appendix measured 3 x 15 cm and the serous layer had signs of congestion. The cross-section of the specimen showed distal obliteration of the lumen. On microscopic examination, the serous layer of the appendix had signs of congestion with aggregates of endometrial glands embedded in a cytogenic stroma surrounded by smooth muscle hypertrophy with complete obliteration of the distal lumen. Diagnosis: appendiceal endometriosis (Fig. 2).
Figure 2. Histopathology. A: Surgical specimen. B: Microscopy. Smooth muscle hypertrophy (short black arrow), endometrial glands surrounded by cytogenic stroma (black arrowhead).
The patient is followed-up in the outpatient clinic of the department of gynecology and is taking specific treatment for peritoneal endometriosis.
Appendiceal endometriosis is a rare condition. In 2013, Arif Emre et al. published a retrospective review of 1255 appendectomy specimens from patients with an initial diagnosis of acute appendicitis, excluding other diagnosis. Only two cases of appendiceal endometriosis were found (0.15% in the entire cohort and 0.36% in the female population of 543 patients). In this series, as 88 patients did not present appendicitis, the incidence of appendiceal endometriosis among these patients was 2.27%1.
In 2017, Dincel et al. reviewed 1970 appendectomy specimens with diagnosis of acute appendicitis and found 59 cases of rare histopathological findings (other than appendicitis). They found only one appendiceal endometriosis (0.05% of all the specimens and 1.69% in the specimens with unusual findings)2.
In 2014, Hakan Guven et al. reported the analysis of 48 patients undergoing right hemicolectomy due to cecal masses mimicking acute appendicitis and found two cases of appendiceal endometriosis (4.16%). These two patients were part of 16 patients in whom malignancy was suspected3.
The preoperative diagnosis of appendiceal endometriosis is difficult, particularly in those patients with unclear clinical presentation. Several protocols have been described to evaluate patients with pelvic endometriosis, as magnetic resonance imaging to detect foci of extrapelvic bowel endometriosis4. However, the preoperative diagnosis is difficult and in most cases the final diagnosis is made by pathological examination of the surgical specimen1-3.
The indication of surgery may be due to laparoscopic examination because of chronic abdominal pain, probable diagnosis of acute appendicitis or resection of tumor masses in the lower right quadrant of the abdomen. Thus, the therapeutic management will be guided by the intraoperative findings, either appendectomy or bowel resections in cases where malignancy is suspected.
Some authors recommend routine appendectomy in women with unexplained and recurrent abdominal pain during a diagnostic laparoscopy, as endometriosis may involve gastrointestinal organs without any involvement of reproductive organs5,6. This approach would be more justified in patients with endometriosis and chronic pelvic pain, showing that patients with ovarian endometriomas and deeply infiltrative endometriosis of the gastrointestinal tract have higher rates of appendiceal endometriosis. It could even prevent future appendicitis secondary to appendiceal endometriosis6.
Major resections are indicated in case of appendiceal masses and suspicion of malignancy3.
Referencias bibliográficas | References
1. Emre A, Akbulut S, Bozdag S, Yilmaz M, Kanlioz M, Emre R, et al. Routine histopathologic examination of appendectomy specimens: Retrospective analysis of 1255 patients. Int Surg. 2013; 98(4):354-62. [ Links ]
2. Dincel O, Goksu M, Turk B, Pehlivanoglu B, Isler S. Unexpected findings in the routine histopathological examinations of appendectomy specimens. A retrospective analysis of 1970 patients. Ann Ital Chir. 2017; 88:519-25. [ Links ]
3. Guven H, Koc B, Saglam F, Bayram I, Adas G. Emergency right hemicolectomy for inflammatory cecal masses mimicking acut appendicitis. World J Emerg Sur. 2014; 9:7. [ Links ]
4. Gimonet H, Laigle-Quérat V, Ploteau S, Veluppillai C, Frampas E. Is pelvic MRI in women presenting with pelvic endometriosis suggestive of associated ileal, appendicular o cecal involvement? Abdom Radiol (NY). 2016; 41(12):2404-10. [ Links ]
5. Shen AY, Stanes A. Isolated appendiceal endometriosis. J Obstet Gynaecol Can. 2016 ; 38(10):979-81. [ Links ]
6. Peters A, Mansuria SM. The role of appendectomy at the time of laparoscopic surgery for benign gynecologic conditions. Curr Opin Obstet Gynecol. 2018; 30(4): 237-42. [ Links ]

