










Servicios Personalizados
Revista

Articulo
 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista argentina de cirugía
versión impresa ISSN 2250-639Xversión On-line ISSN 2250-639X
Rev. argent. cir. vol.111 no.4 Cap. Fed. dic. 2019
CARTA CIENTÍFICA | SCIENTIFIC LETTER
Neumatosis intestinal. Rara presentación de abdomen agudo
Pneumatosis intestinalis: a rare presentation of acute abdomen
Fabiana B. Mazzei, Nicolás F. Mazzei, Carolina Magraht, Diego M. Fusco, Diego G. Herrera
Servicio de Cirugía General. Hospital Interzonal Dr. Prof. Ramon Carrillo. Ciudadela, Buenos Aires. Argentina.
Correspondencia Correspondence: Fabiana B. Mazzei Email: fmazzei89@gmail.com
Los autores declaran no tener conflictos de interés.
Conflicts of interest None declared.
http://dx.doi.org/10.25132/raac.v111.n4.1422es
Recibido | Received 08-01-19
Aceptado | Accepted 21-05-19
RESUMEN
La neumatosis intestinal es una entidad poco frecuente. Se caracteriza por la presencia de gas en la subserosa o submucosa, o en ambas, a través del tracto gastrointestinal. Presentamos dos casos en los cuales el motivo de consulta fue dolor abdominal generalizado asociado a reacción peritoneal. Se realizó tomografía computarizada (TC) en ambos casos, donde se evidenciaron distensión intestinal, neumatosis intestinal y neumatosis portal. Posteriormente se llevó acabo laparotomía de urgencia y se encontró necrosis intestinal con isquemia mesentérica, hallazgo compatible con imágenes tomográficas. Ambos pacientes fallecieron (uno durante el acto quirúrgico y el otro en el posquirúrgico inmediato).
Palabras clave: Neumatosis intestinal; Neumatosis portal; Abdomen agudo.
ABSTRACT
Pneumatosis intestinalis is a rare condition characterized by the presence of gas in the submucosa or subserosa of the intestinal wall. We report two cases associated with generalized abdominal pain and rebound tenderness. The computed tomography (CT) scans in both cases showed bowel distention, pneumatosis intestinalis and portal venous gas. Both patients underwent emergency surgery which demonstrated bowel necrosis with mesenteric ischemia, consistent with the CT images. Both patients died (one during surgery and the other in the immediate postoperative period).
Keywords: Intestinal pneumatosis; Portal pneumatosis; Acute abdomen.
La neumatosis intestinal (NI) es una entidad muy infrecuente asociada a varias patologías, como el infarto intestinomesentérico, la enterocolitis necrotizante y la enfermedad pulmonar obstructiva crónica. Se caracteriza por la presencia de gas en la subserosa o en la submucosa a través del tracto gastrointestinal. Es un signo radiológico que puede presentarse en pacientes asintomáticos o en cuadros de dolor abdominal agudo1. Registra una incidencia de 0,03 %2 e incluye un espectro que va desde un hallazgo benigno incidental hasta isquemia o necrosis mesentérica, esta última con una alta mortalidad.
La neumatosis portal (NP) es otro signo radiológico que se observa usualmente cuando ocurre necrosis intestinal; sin embargo, numerosas publicaciones han comunicado la coexistencia de NP en el curso de una NI.
Caso clínico 1. Presentamos una paciente mujer de 52 años con antecedentes de hipertensión arterial (HTA), dislipidemia, IRC dialítica que ingresa por cuadro de dolor abdominal generalizado de 12 horas de evolución y vómitos, posterior a diálisis. Al examen físico se encontraba febril (38,3 °C), con tensión arterial de 100/60 mm Hg, frecuencia cardíaca de 110 lpm, frecuencia respiratoria de 18 rpm y una saturometría de pulso al aire ambiente de 90%. Presentaba el abdomen distendido, ausencia de RHA, con aumento de tensión, doloroso, timpánico y con reacción peritoneal.
Se realiza laboratorio cuyos valores arrojan leucocitosis, función renal alterada (urea de 160, creatinina de 3,2).
Se decide realizar tomografía sin contraste debido al antecedente de la insuficiencia renal en la que se evidencia una importante NI que incluye todo el marco duodenal, intestino delgado y colon, así como la presencia de gas en ramas portales y neumatosis mesentérica (Figs. 1 y 2).
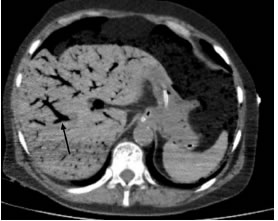
Figura 1
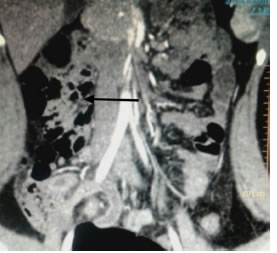
Figura 2
Se decide laparotomía exploradora y se halla isquemia del tronco celíaco con necrosis intestinal, esplénica y hepática asociada a múltiples trombos en mesenterio.
Paciente óbita en acto operatorio por falla multiorgánica.
Caso clínico 2. Paciente masculino de 68 años con antecedentes de HTA consulta por dolor abdominal y distensión de 24 horas de evolución. Refería falta de eliminación de gases y catarsis de varios días antes de la consulta. Al examen físico se encontraba lúcido, afebril, con signos vitales dentro de los parámetros normales, abdomen tenso poco depresible, doloroso generalizado, y RHA ausentes.
Los exámenes de laboratorio muestran leve leucocitosis (11000), hematocrito 37%, Hb 10,1 y creatinina 1,8 mg/dL.
Se solicita radiografía de abdomen simple que revela distensión a nivel intestinal.
Se complementa su estudio con una TC de abdomen y pelvis, la cual evidencia una neumatosis que compromete el estómago y el intestino delgado hasta íleon distal, a la que se asocia la presencia de gas en el sistema porta.
Se decide laparotomía, por evolución desfavorable clínica del paciente, y se encuentra isquemia mesentérica asociada a necrosis intestinal. El paciente fallece 48 horas después de la operación.
La NI es una poco frecuente presentación de abdomen agudo. Una teoría considera que puede ser causada por la infiltración de gas a través de la pared intestinal, secundaria a un aumento de la presión intraluminal con disrupción de la capa mucosa, mientras que otra teoría sostiene la producción de gas por bacterias intestinales que atraviesa la mucosa intestinal.
El primer caso presentado es una paciente con neumatosis intestinal e isquemia intestinal, producto de la hipoperfusión asociada a diálisis y antecedentes de ateroesclerosis y dislipidemia. En el segundo caso, el paciente no refería antecedentes de relevancia, salvo la HTA.
El tratamiento de la NI parte de la patología de base, pudiéndose optar por tratamiento conservador o quirúrgico3.
El factor más importante en el manejo clínico de pacientes con un abdomen agudo, con hallazgos de NI y gas venoso portal, es la determinación de necrosis intestinal. De no existir esta, se podría optar por un tratamiento conservador.
Aquellos pacientes que presentan isquemia, necrosis y sepsis, habitualmente requieren conducta quirúrgica, pero la la mortalidad es de alrededor del 75%.
ENGLISH VERSION
Pneumatosis intestinalis (PI) is a rare condition associated with several diseases, as bowel infarction, necrotizing enterocolitis and chronic obstructive pulmonary disease. It is characterized by the presence of gas in the submucosa or subserosa of the intestinal wall. Pneumatosis intestinalis is a radiographic sign that may occur in the absence of symptoms or associated with acute abdominal pain1. The incidence of PI is 0.03%2 and the clinical significance ranges from benign to catastrophic with high mortality in cases of mesenteric ischemia or bowel infarction.
Portal venous gas (PVG) is another radiographic sign usually found in case of bowel necrosis, but several publications have reported the coexistence of PVG with PI.
Case report 1. A 52 yearold female patient with a history of hypertension (HT), dyslipidemia and chronic kidney failure with requirement of hemodialysis was admitted to hospital due to generalized abdominal pain lasting 12 hours and vomiting after dialysis. On physical examination she presented fever (38.3 °C), blood pressure of 100/60, heart rate of 110 bpm, respiratory rate of 18 bpm and pulse oxygen saturation of 90% breathing room air. The abdomen was distended and tender with guarding and rebound tenderness, tympanic and with absence of bowel sounds.
The lab tests showed leukocytosis and impaired kidney function (blood urea nitrogen 160 mg/dL and creatinine level 3.2 mg/dL).
A computed tomography (CT) scan without contrast media that was performed due to the history of kidney dysfunction showed large PI involving the duodenal loop, small bowel and colon, PVG and mesenteric pneumatosis (Figs. 1 and 2).
Figure 1
Figure 2
The patient underwent exploratory laparotomy which demonstrated celiac trunk ischemia with bowel, splenic and hepatic necrosis associated with multiple mesenteric thromboses.
The patient died during surgery due to multiorgan failure.
Case report 2 . A 68 yearold male patient with a history of HT sought medical care for abdominal pain and distention lasting 24 hours. He complained of inability to pass gas and constipation on the previous days. On physical examination, the patient appeared lucid, with no fever and the vital signs were within normal parameters. The abdomen was rigid, tender on palpation and with absence of bowel sounds.
The lab tests showed discrete leukocytosis (11,000/mm3), the hematocrit was 30%, hemoglobin level of 10.1 mg/dL and creatinine level of 1.8 mg/dL.
The plain abdominal Xray showed bowel distension.
A CT scan of the abdomen and pelvis showed pneumatosis involving the stomach and small bowel up to the distal ileum, associated with PVG.
The patient evolved with unfavorable clinical course and underwent laparatomy, which revealed mesenteric ischemia associated with bowel necrosis. The patient died 48 hours after surgery.
Pneumatosis intestinalis is a rare presentation of acute abdomen. A theory hypothesizes that gas dissects the mucosa layer into the bowel wall from the intestinal lumen due to increased pressure, while another theory proposes that gas produced by gasforming bacteria enter the bowel wall through the submucosa.
The first case reported is a female patient with PI and bowel ischemia secondary to hypoperfusion associated with dialysis and a history of atherosclerosis and dyslipidemia. In the second case report, the patient had no significant personal past history, except for HT.
The management of PI involves treatment of the underlying condition and may require surgical intervention or medical care3.
The presence of bowel necrosis is the most significant risk factor in patients with acute abdomen, PI and PVG to decide therapy. A conservative approach can be decided in the absence of bowel necrosis.
Patients with ischemia, necrosis and sepsis usually require surgical management, but mortality is about 75%.
Referencias bibliográficas | References
1. Wayne E, Ough M, Wu A, Liao J, Andresen KJ, Kuhen D, et al.Management algorithm for pneumatosis intestinalis and portal venous gas: treatment and outcome of 88 consecutive cases. J Gastrointest Surg. 2010; 14:437-48. [ Links ]
2. Sooby P, Harshen R, Joarder R. An unusual triad of pneumatosis intestinalis, portal venous gas and pneumoperitoneum in an as ymptomatic patient. J SurgCase Rep. 2015;4:1-3 [ Links ]
3. DuBose JJ, Lissauer M, Maung AA, et al. Pneumatosis Intestinalis Predictive Evaluation Study (PIPES): a multicenter epidemiologic study of the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2013; 75:15-23. [ Links ]

