










Serviços Personalizados
Journal

Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista argentina de cirugía
versão impressa ISSN 2250-639Xversão On-line ISSN 2250-639X
Rev. argent. cir. vol.112 no.2 Cap. Fed. jun. 2020
ARTÍCULO ESPECIAL| SPECIAL ARTICLE
Reducción de la exposición en residentes de Cirugía frente al brote de COVID-19
Reduction of exposure in residents of Surgery in face of the outbreak of COVID-19
Agustín Morales, Mora Achával, Juan C. López Meyer, Carla Vega, Gerónimo Faillace, Guadalupe Iudica, Ezequiel Verde, Carina Chwat
Servicio de Cirugía General Hospital Universitario Austral. Buenos Aires. Argentina
Correspondencia | Correspondence: Carina Chwat e-mail: carinachwat@gmail.com
Los autores declaran no tener conflictos de interés.
Conflicts of interest None declared.
http://dx.doi.org/10.25132/raac.v112.n2.1492.es
Recibido | Received 01-04-20
Aceptado | Accepted 12-05-20
Actualizado al 13-05-20
RESUMEN
El brote mundial de COVID-19 durante el primer trimestre de 2020 constituye un desafío sin precedentes para el sistema de salud.
El objetivo es describir las estrategias adoptadas por los residentes de Cirugía General de un Hospital Universitario de la Argentina, para salvaguardar la salud de los residentes, reducir el riesgo de exposición de los pacientes quirúrgicos, mantener la formación académica continua y fomentar el trabajo en equipo.
Minimizar la exposición de los residentes dividiendo el personal total en dos equipos que trabajan por quincenas; dividir las actividades, las horas dentro del hospital y los turnos por igual entre los residentes; usar telemedicina para controles posoperatorios/ ambulatorios; suspender la actividad de consultorio; organizar clases diarias en línea y revisiones de artículos publicados.
En el contexto de la pandemia de COVID-19 se deben utilizar todos los medios para minimizar el riesgo de exposición para así optimizar los recursos humanos. A pesar de que estas estrategias pueden aplicarse fácilmente a otras residencias, se necesita más investigación para evaluar su impacto en la transmisión de enfermedades, y en la salud física y emocional de los profesionales de la salud.
Palabras clave: COVID-19; Residencia en cirugía; Medidas para reducir la exposición.
ABSTRACT
The worldwide outbreak of COVID-19 during the first quarter of 2020 constitutes an unprecedented challenge for the health system.
The aim is to describe the strategies adopted by residents of General Surgery of a university hospital of Argentina, to safeguard the health of residents, reduce the risk of exposure of surgical patients, maintain continuous academic training and promote teamwork.
Minimize resident exposure by dividing the group into two teams that work by fortnights; divide activities, hours within hospital, and shifts equally among residents; use telemedicine for postoperative / ambulatory controls; suspend office activity; organize daily online classes and reviews of published articles.
In the context of the COVID-19 pandemic, all means should be used to minimize the risk of exposure in order to optimize human resources. Although these strategies can easily be applied to other residencies, more research is needed to assess their impact on disease transmission, and on the physical and emotional health of health professionals.
Keywords: COVID-19; Residency in surgery; Measures to reduce exposure.
Introducción
En el curso de 2020, la enfermedad por coronavirus (COVID-19) ha afectado a 197 países, áreas o territorios, con 416 686 casos confirmados y 18 569 muertes confirmadas en todo el mundo1. Entre el 9 y el 20% de los profesionales de la salud se han visto afectados por el virus, lo que resulta casi en un colapso del sistema de salud, ya que cada trabajador afectado necesita al menos 14 días de cuarentena2-4.
El primer caso informado en la Argentina fue del 5 de marzo. En las tres semanas posteriores se comunicaron 502 casos, con 8 muertes5. El 21 de marzo, el primer caso COVID-19 fue confirmado en nuestro hospital. Hasta la fecha (13/05/2020), el 40% de los casos en nuestra Institución son proveedores de atención médica, ninguno de ellos parte del Departamento de Cirugía. El número total de casos de COVID 19 en la institución fue de 42 hasta la actualidad.
Actualmente no hay literatura disponible que avale un esquema ideal para los sistemas de residencia quirúrgica durante esta crisis.
El objetivo de este informe es describir las estrategias adoptadas por nuestro grupo de residentes de Cirugía General, para resguardar su salud, optimizar la disponibilidad durante la fase crítica de la pandemia, así como tratar de reducir el riesgo de exposición de pacientes quirúrgicos, manteniendo la formación académica continua y fomentando el trabajo en equipo.
Estrategias adoptadas por los residentes de Cirugía General
Además de las medidas descriptas y adoptadas por el Departamento de Cirugía se aplicaron institucionalmente los principios básicos de prevención y control de las infecciones, y las precauciones estándar recomendadas por la Organización Mundial de la Salud6
Todas las estrategias adoptadas por los residentes de Cirugía General se ejecutaron de acuerdo con las pautas de nuestro hospital y las recomendaciones del Departamento de Cirugía. Estas se implementaron antes de nuestro primer caso COVID-19 confirmado.
Los principios que definieron dichas estrategias fueron: protección de la salud de los residentes, asegurar la cobertura de las actividades del servicio, tener un sistema de comunicación que conectase a los residentes en el hospital con los que estaban en su casa, mantener la actividad académica y reducir el riesgo de exposición de los pacientes quirúrgicos.
Horas de trabajo por residente y cobertura de actividades del servicio
Teniendo en cuenta el comportamiento epidemiológico de la enfermedad, los residentes se dividieron en dos grupos. Cada grupo cubriría períodos quincenales, asignando tres o cuatro residentes para cubrir las necesidades diarias del hospital (cirugías no electivas o evaluación clínico- quirúrgica de pacientes e interconsultas).
Antes del brote de COVID-19, las actividades se distribuían según el año de residencia. De haberse mantenido ese esquema, los residentes del primer año hubieran estado particularmente expuestos en comparación con otros residentes, por lo que se eliminó la jerarquía de residencia. Las actividades, las horas dentro del hospital y los guardias se dividieron en partes iguales entre los 15 residentes (Tabla 1).
Table 1
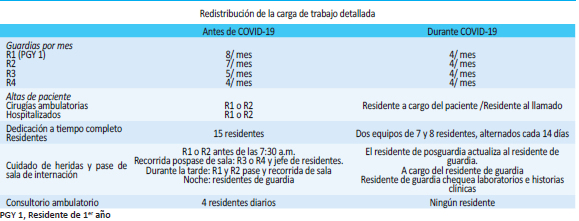
Se suspendieron todas las rotaciones externas e internas en curso, así como las que hubieran tenido lugar en los meses futuros.
Además se modificó cada equipo de guardia para reducir el número de residentes por turno de 3 residentes a 2 (cada 24 horas).
Telemedicina
Los residentes continuaron brindando atención y seguimiento posoperatorio mediante telemedicina. Todos los pacientes recibieron un número de teléfono de urgencia y se los educó para identificar pautas de alarma. De presentar una recuperación óptima , no se programarían controles presenciales. De aparecer signos de alarma, se solicitaría a los pacientes su pronta consulta con Cirugía en el hospital.
Comunicación entre residentes: Se creó un grupo de WhatsApp para mantener un intercambio de información fluida entre los residentes, especialmente en cuanto al seguimiento ambulatorio de los posoperatorios de bajo riesgo y los casos de diverticulitis no complicada, reduciendo al mismo tiempo el contacto entre los residentes.
Actividad académica
Se organizaron discusiones en línea de temas programados, con clases diarias y revisiones de artículos publicados.
Durante el período de aplicación de estas estrategias ningún miembro del Departamento de Cirugía resultó infectado por SARS-CoV-2.
Conclusión
Durante la pandemia de COVID-19, la situación de cada institución cambia día a día. En este escenario dinámico se deben utilizar todos los medios posibles para minimizar el riesgo de exposición y así optimizar los recursos humanos durante el período crítico.
El potencial aumento de personal sanitario infectado (o en cuarentena) requeriría una redistribución urgente de la carga de trabajo y cambios en las rutinas diarias.
Dicha redistribución se puede realizar con anticipación para preservar la salud de los residentes, tratar de evitar el colapso del sistema de salud, reducir la exposición de los pacientes quirúrgicos, continuar el crecimiento académico y fomentar el trabajo en equipo.
A pesar de que estas estrategias pueden aplicarse fácilmente a otras residencias, se necesita más investigación para evaluar su impacto en la transmisión de la enfermedad y en la actividad de los profesionales de la salud.
ENGLISH VERSION
Introduction
In the course of 2020, coronavirus disease (COVID-19) has affected 197 countries, areas or territories, with 416 686 confirmed cases and 18 569 confirmed deaths worldwide1. Between 9 and 20% of health professionals have been affected by the virus, which almost results in a collapse of the health system, since each affected worker needs at least 14 days of quarantine2-4.
The first case reported in Argentina was on March 5. In the following three weeks, 502 cases were reported, with 8 deaths5. On March 21, the first COVID-19 case was confirmed in our hospital. To date (05/13/2020), 40% of the cases in our Institution are health care providers, none of them part of the Department of Surgery. The total number of COVID 19 cases in the institution was 42 to date.
Currently there is no literature available that supports an ideal scheme for surgical residency systems during this crisis.
The objective of this report is to describe the strategies adopted by our group of General Surgery residents, to safeguard their health, optimize availability during the critical phase of the pandemic, as well as try to reduce the risk of exposure of surgical patients, maintaining the continuous academic training and promoting teamwork.
Strategies adopted by residents of general surgery
In addition to the measures described and adopted by the Department of Surgery, the basic principles of infection prevention and control and the standard precautions recommended by the World Health Organization were institutionally applied6.
All the strategies adopted by the residents of General Surgery were executed in accordance with the guidelines of our hospital and the recommendations of the Department of Surgery. These were implemented before our first confirmed COVID-19 case.
The principles that defined these strategies were: protection of the health of residents, ensuring coverage of service activities, having a communication system that connects residents in the hospital with those who were at home, maintaining academic activity and reduce the risk of exposure of surgical patients.
Hours of work per resident and coverage of service activities
Taking into account the epidemiological behavior of the disease, the residents were divided into two groups. Each group would cover biweekly periods, assigning three or four residents to cover the daily needs of the hospital (non-elective surgeries or clinical-surgical evaluation of patients and interconsultations).
Before the COVID-19 outbreak, activities were distributed by year of residency. If that scheme had been maintained, the first-year residents would have been particularly exposed compared to other residents, so the hierarchy of residency was eliminated. Activities, hours within the hospital, and on-calls were divided equally among the 15 residents (Table 1).
Table 1

All ongoing external and internal rotations were suspended, as well as those that would have occurred in future months.
In addition, each on-calls team was modified to reduce the number of residents per shift from 3 residents to 2 (every 24 hours).
Telemedicine
Residents continued to provide postoperative care and follow-up using telemedicine. All patients received an emergency phone number and were educated to identify alarm patterns. If there is an optimal recovery, face-to-face controls would not be scheduled. If alarm signs appear, patients will be asked for their prompt consultation with Surgery in the hospital.
Communication between residents: A WhatsApp group was created to maintain a fluid exchange of information between residents, especially regarding outpatient follow-up of low-risk postoperative and cases of uncomplicated diverticulitis, while reducing contact between residents. .
Academic activity
Online discussions of scheduled topics were organized, with daily classes and reviews of published articles.
During the period of application of these strategies, no member of the Department of Surgery was infected with SARS-CoV-2.
Conclusion
During the COVID-19 pandemic, the situation of each institution changes from day to day. In this dynamic scenario, all possible means should be used to minimize the risk of exposure and thus optimize human resources during the critical period.
The potential increase in infected (or quarantined) healthcare personnel would require an urgent redistribution of workload and changes in daily routines.
Such redistribution can be done in advance to preserve residents’ health, try to avoid collapse of the health system, reduce exposure of surgical patients, continue academic growth, and encourage teamwork.
Although these strategies can easily be applied to other residences, more research is needed to assess their impact on disease transmission and on the activity of health professionals.
Agradecimientos
Nos gustaría agradecer al Dr. Fernando Iudica y al staff mayor de Cirugía General por su continuo apoyo, dedicación e incentivo.
Acknowledgements
We would like to thank Dr. Fernando Iudica and the senior staff of General Surgery for their continued support, dedication and incentive.
Referencias bibliográficas/References
1. World Health Organization Report. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 25 March 2020) [ Links ]
2. Centers for Disease Control and Prevention. Healthcare Professionals: Frequently Asked Questions and Answers https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html [ Links ]
3. Schwartz J, King CC, Yen MY. Protecting Health Care Workers during the COVID-19 Coronavirus Outbreak –Lessons from Taiwan’s SARS response. Clin Infect Dis. 2020. doi:10.1093/cid/ciaa255
4. Editorial. COVID-19: Protecting health-care workers. . 2020; 395(Issue 10228).
5. Nuevo Coronavirus (COVID-19) Reporte diario: 5 de marzo de 2020. Ministerio de Salud de la Nación. Buenos Aires. Published online: https://www.argentina.gob.ar/coronavirus/informe-diario [ Links ]
6. World Health Organization. Infection prevention and control during health care when COVID-19 is suspected: interim guidance (19 march 2020). [ Links ]

