










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista argentina de cirugía
versão impressa ISSN 2250-639Xversão On-line ISSN 2250-639X
Rev. argent. cir. vol.114 no.4 Cap. Fed. out. 2022
http://dx.doi.org/10.25132/raac.v114.n4.1518
Articles
Three-dimensional computed tomography reconstruction for the diagnosis of traumatic urethral injuries
1 Hospital General de Agudos Donación Francisco Santojanni. Buenos Aires. Argentina
In August 1087, King William I of England sustained a straddle injury of his bulbar urethra while riding on horseback, which was evident by a change in the color of his urine; at that time it was considered a fatal injury, and he died months later1. With the advent of modern technologies, the severity of these lesions was relegated in history, as they have a favorable course with a timely diagnosis.
Urethral injuries are rare in emergency department visits; they are usually associated with polytrauma, mainly in blunt trauma with or without pelvic fracture. These injuries occur between the third and fourth decade of life, with a slight predominance in male patients due to the length of the urethra and supporting ligaments2. Patients may be asymptomatic or may present with a variety of signs and symptoms, as perineum or groin pain, hematoma in the perineum and scrotum, or inability to urinate associated with urethral bleeding; the magnitude of the bleeding is not related with the severity of the injury. This condition should be suspected in patients with blunt trauma to the pelvis and perineum; trauma to the urethra accounts for < 1.5% of all traumas and affects 1/45 000 population per year3.
The mechanism of injury is classified as iatrogenic, due to urethral catheterization, which accounts for 3.2 urethral injuries per 1000 hospital patients, and non-iatrogenic trauma which is more common and more serious because the force required to injure the urethra is very much greater. Within this subgroup, fall-astride injuries and motor vehicle incidents are the most common urethral injuries seen in the emergency department. Depending on the severity of the injury, they can be classified as contusion, complete disruption or partial disruption and, depending on the anatomic location4, in anterior or posterior injuries which are generally associated with pelvic fractures according to the classification of the American Association for the Surgery of Trauma.
An 18-year-old male patient visited the emergency department due to inability to void associated with minor urethral bleeding lasting 1 hour. The patient, who was a motorcycle driver, reported a low-speed car accident, which caused direct impact with the central area of his motorcycle, resulting in trauma to the perineum. On physical examination, the patient had a Revised Trauma Score of 12 points without clinical evidence of perineum injury and normal mobility of the 4 extremities. The laboratory tests were normal. A three-way 16 Fr Foley catheter was placed in the urinary meatus, the balloon was inflated with 5 cm3 of saline and retrograde urethrography was performed. After instillation of 20-30 cm3 of water-soluble contrast medium diluted to 20% (Fig. 1) extravasation of contrast medium was observed at the level of the posterior urethra. Contrast-enhanced threedimensional computed tomography of the abdomen and pelvis with 3D reconstruction was performed to complete the assessment of the abdomen and pelvis according to the mechanism of injury, with no evidence of concomitant lesions. Due to the persistence of contrast medium in the urethra and the availability of appropriate technology, we decided to perform a 3D reconstruction of the urethra. With this approach, we reached the diagnosis of a partial disruption in the posterior urethra, patent urethra and extravasation of contrast agent, with a gap distance of 5 millimeters between both ends (Fig. 2), associated with fracture of the right iliac crest that did not require surgery. A suprapubic cystostomy was made to drain the urinary tract, and 8 hours after admission the department of urology performed surgical repair. After two years of follow-up, there was no evidence of urethral stricture.

Figure 1 Retrograde urethrography with administration of contrast agent. The big arrow indicates contrast extravasation in the posterior urethra and the small arrow shows the urinary catheter through which the contrast agent is instilled.
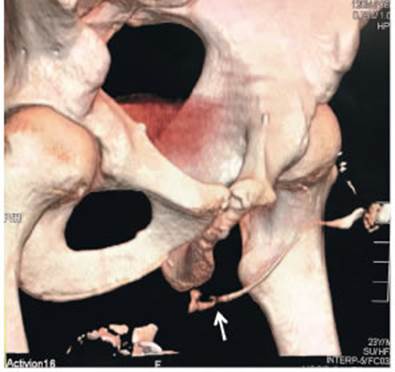
Figure 2 Three-dimensional computed tomography reconstruction. The arrow indicates the injury of the posterior urethra with a gap distance of 5 mm between the ends and a patent urethra with passage of contrast into the bladder.
Nowadays, multislice computed tomography scanners allow acquisition of high-resolution images which, together with three-dimensional reconstructions, has allowed computed tomography urography to become the technique of choice for the evaluation of the urinary tract, replacing traditional urography in patients with hematuria and risk factors for cancer5. In our experience as a trauma referral center, this method allows evaluation of the site of urethral injury, the gap distance between the ends and associated injuries as fracture of the pelvic ring and intra-abdominal organs. The literature analyzed describes the indirect signs in the CT scan that reveal a probable urethral injury. These include extravasation of contrast material, elevation of the prostate, distortion of the fat plane, hematoma of the ischiocavernosus muscle, distortion and obscuration of the prostatic contour and bulbocavernosus muscle, which are most commonly associated with complicated pelvic fractures and which cannot be detected in retrograde urethrography6.
Retrograde urethrography is the gold standard technique for the diagnosis of these injuries, using 20- 30 mL of water-soluble contrast medium administered through the urinary meatus. The advantages of this method are its low cost, short duration and availability in the hospital setting, but it is not very conclusive in terms of the extent of the injury, the gap distance between the two ends, and the site and anatomical characteristics of the injury6. As we have already mentioned, the use of computed tomography for the diagnosis of the intra-abdominal urinary tract is accepted worldwide due to its high sensitivity and specificity, while magnetic resonance imaging is used for the diagnosis of urethral lesions7. In the case reported, we offered the patient the combination of retrograde urethrography with transurethral contrast and computed tomography with intravenous contrast and transurethral water-soluble contrast. In this way we were able to reconstruct the entire urinary tract down to the urinary meatus, evaluate the presence of associated injuries of the pelvis, abdomen, thorax and brain in the context of acute trauma. This was extremely helpful to the urology team, as the patient was immediately treated with the endoscopic placement of a urinary catheter. The disadvantages of this method are its costs and availability in healthcare centers, since our hospital counts with a Toshiba Aquilion 16 CT scanner. Nevertheless, we can highlight that this condition is not quite common, it usually occurs in large cities, and is managed in health care centers equipped with this type of computed tomography scanners. The indisputable benefit of the technique is the possibility of diagnosing major associated injuries requiring treatment before or simultaneously with the injury of the final segment of the urinary tract. This approach reduces the use of complementary imaging tests as X-rays and retrograde urethrography which delay treating the patient.
As a working group, we propose its use to change the gold standard for the diagnosis of this condition considering the benefits of this technique which include a complete diagnosis of urinary tract injury and adjacent organs, and operative planning.
Referencias bibliográficas /References
1. Mundy A, Andrich D. Urethral trauma. Part I: introduction, history, anatomy, pathology, assessment and emergency management. BJU international. 2011; 108:310-27. [ Links ]
2. Ballesteros M, Maffei D, Maldonado G, Leonidas Pontel FA, Muro M, Díaz GN. Manejo de los Traumatismos de pelvis. Rev Argent Cirug. 2002;82(1-2):11-21. [ Links ]
3. Day A, Andrich D. Proposed mechanisms of lower urinary tract injury in fractures of the pelvic ring. BJU International. 2007;100(3): 567-73. [ Links ]
4. Djakovic L, Martínez-Piñeiro L, Mor Y, Plas E. Traumatismos urológicos. Asociación Europea de Urología. 2005, Actualización 2009;47:202-10. [ Links ]
5. Hermosilla K M, Cabrera R, Horwitz B, Raurich R, et al. Multislice ct urography (uro-ct): adescriptive study using split bolus technique. Revista Chilena de Radiología. 2009; 15(2):65-9. [ Links ]
6. Ali M, Safriel Y, Sclafani SJ, Schulze R. CT signs of urethral injury. Radiographic. 2003;23(4):951-63. [ Links ]
7. Theisen KM, Kadow BT, Rusilko PJ. Three-Dimensional Imaging of Urethral Stricture Disease and Urethral Pathology for Operative Planning. Curr Urol Rep. 2016;17:54. [ Links ]
Received: April 12, 2021; Accepted: July 15, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
