











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The incidence and prevalence of type 2 diabetes mellitus (DM) in adults are increasing, and diabetic nephropathy (DN), one of the most common complications of DM that develops in approximately 40% of the patients, has become the leading cause of end-stage renal disease (ESRD) in developed countries.1-4 DN is usually a clinical diagnosis based on the presence of albuminuria and/or reduced estimated glomerular filtration rate (eGFR) in the absence of signs or symptoms of other primary causes of kidney damage.5-7
Albuminuria, albeit a strong predictor of
DN progression, lacks specificity and sensitivity for the diagnosis of ESRD and the progressive decline in eGFR.8-10 Kidney biopsy, which is the gold standard for definitive diagnosis of DN, is not indicated in patients with DM.7) The risk of such intervention is not justified in the absence of other treatment options currently available for DN beyond the current approach including optimal control of DM, hypertension (HTN), dyslipidemia, and lifestyle modification. 11-13 Worsening DN over time is associated with increased risk of cardiovascular and cerebrovascular events as well as renal morbidity and mortality.(8, 14-15) We evaluated the decline in renal function according to albuminuria levels in patients with DN and analyzed the prognosis of renal function and the incidence of cardiovascular disease (CVD), cerebrovascular disease, and peripheral artery disease (PAD).
METHODS
Study population
In this single-center retrospective study, medical records of 1345 patients with DN treated in Chungnam National University Hospital between January 1, 2012 and December 31, 2018 were reviewed. The inclusion criteria were: 1) urinary albumin to creatinine (Cr) ratio (ACR) >30 mg/g Cr in two or more tests; 2) age >18 years; 3) eGFR (Modification of Diet in Renal Disease, MDRD) >60 mL/min/1.73 m2 at the time of DN diagnosis; 4) follow-up of one year or more. The exclusion criteria were: 1) type 1 DM; 2) diagnosis of a kidney disease other than DN by kidney biopsy; 3) kidney transplantation before or after urine ACR test; and 4) DN diagnosis by urine dipstick or urinary protein to Cr ratio test without an accompanying urine ACR test.
The urine ACR was within normal limits or was >30 mg/g Cr in only one test in 141 patients, whereas it was not determined in 167 patients. Additionally, 632 patients had an eGFR of <60 mL/min/1.73 m2 at the time of urine ACR test and 27 patients had kidney transplantation before urine ACR test. Furthermore, 26 patients have an out-patient follow-up of less than one year and 21 patients were diagnosed with a disease other than DN by kidney biopsy. After the exclusion of these patients, the remaining 331 patients were
included in the final analyses.
Measurements and definitions
The patient medical records were reviewed to collect data on age, sex, initial urine ACR, serum Cr, and eGFR during and after initial urine ACR test; comorbidities (HTN and hyperlipidemia); percutaneous coronary intervention (PCI); heart failure diagnosis (ejection fraction <50%); cerebrovascular disease; PAD; hemodialysis (HD); results of kidney biopsy; treatment with renin- angiotensin system inhibitors (RASi; angiotensin- converting enzyme inhibitors, angiotensin II receptor blockers); and duration of follow-up.
The clinical diagnosis of DN was based on the detection of microalbuminuria (urine ACR >30 mg/g Cr in two randomly collected urine samples). Chronic kidney disease (CKD) was defined as eGFR <60 mL/min/1.73 m2 for 3 months. CVD was defined as a history of PCI performed for angina or myocardial infarction. Cerebrovascular disease was defined as a history of stroke or brain hemorrhage excluding trauma. PAD was defined as an ankle-brachial index <0.9 or a history of percutaneous transluminal angioplasty in lower extremities.
Primary outcomes were renal prognosis including CKD (eGFR <60 mL/min/1.73 m2), >50% decrease in eGFR from baseline value determined at initial DN diagnosis, and HD due to deterioration of renal function. Secondary outcomes were prevalence of CVD, heart failure, cerebrovascular disease, and PAD.
The study cohort of 331 patients was classified into mildly increased albuminuria (microalbuminuria), moderately increased albuminuria, and severely increased albuminuria groups according to their urine ACR of 30-300, 300-900, and >900 mg/g Cr, respectively. The primary and secondary outcomes were compared among the three groups.
The urine ACR test was evaluated with the first urine ACR. After that, urine ACR test was evaluated as the average value when the initial urine ACR test was performed within one year; subsequent values were excluded from the evaluation because urine ACR levels could be high due to the exacerbation of DN.
Statistical analysis
Continuous variables were expressed as means with standard deviation, and discrete variables were presen ted as percentages (%). Continuous variables were analyzed using Student’s t test, and categorical variables were analyzed using Pearson’s %2 test (or Fisher’s exact test used with limited data) and linear by linear association test. Differences in follow-up duration among the groups were evaluated using the Kruskal- Wallis test. Multivariate analysis of risk factors for renal prognosis was performed using logistic regression. All analyses were performed using SPSS Statistics version 20.0 (IBM, Armonk, NY, USA), and p values of less than 0.05 were considered statistically significant (SPSS version 20.0, Chicago, IL, USA).
Ethics statement
The Institutional Review Board (IRB) of Chungnam National University Hospital (IRB No. 2020-04-029) approved the study. Informed consent requirement was waived. We conducted this study in compliance with the principles of the Declaration of Helsinki.
RESULTS
Baseline characteristics and laboratory findings
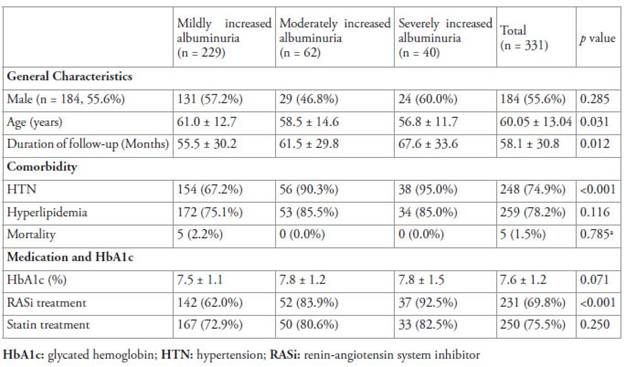
Table 1 shows the demographic characteristics of the three groups. The mean age of the whole cohort was 60.05 ± 13.04 years. There was a significant difference in ages among the three groups, and it was found that age in the severe albuminuria group was significantly young. HTN was more common in the macroalbuminuria group (moderately to severely increased albuminuria groups; 92.2%, 94/102) than that in the microalbuminuria group (mildly increased albuminuria group; 67.2%, 154/229; p<0.001). However, there was no significant difference in the prevalence of HTN between the moderately increased albuminuria and severely increased albuminuria (p=0.391). There were among- group differences in the rates of duration of follow-up, HTN, and RASi treatment. Due to the among-group difference in the rate of HTN as a comorbidity, the rate of patients on RASi treatment was also lower in the microalbuminuria group than in the macroalbuminuria group (p<0.001).
Renal function and renal prognosis
Table 2 shows the comparison of renal function and renal prognosis among the three groups. Serum Cr and eGFR at the time of DN diagnosis based on the initial urine ACR were not significantly different among the three groups. Final serum Cr and eGFR showed a statistically significant tendency to worsen in the group with high urine ACR at the time of DN diagnosis (p<0.001). The follow-up duration was different among the three groups (Table 1); therefore, the rate of reduction in eGFR per year was calculated. The mean rate of reduction in eGFR was 2.90 ± 8.02 mL/min/1.73 m2 per year in the overall study cohort, with a significant difference observed among the three groups (p<0.001). Specifically, the rate of deterioration in renal function based on eGFR reduction per year was faster in the group with high urine ACR at the time of DN diagnosis. Comparison between the microalbuminuria (mildly increased albuminuria) and macro albuminuria (moderately to severely increased albuminuria) groups revealed that the mean eGFR decreased by 1.47 ± 6.61 mL/min/1.73 m2 per year in the microalbuminuria group and by 6.10 ± 9.83 mL/in/1.73 m2 per year in the macroalbuminuria group (p< 0.001). The rate of deterioration in renal function based on eGFR reduction per year in macroalbuminuria group was as follows: 4.10 ± 8.98 mL/min/1.73 m2 in moderately increased albuminuria group, 9.19 ± 10.39 mL/ min/1.73 m2 in severely increased albuminuria group. (Table 2)
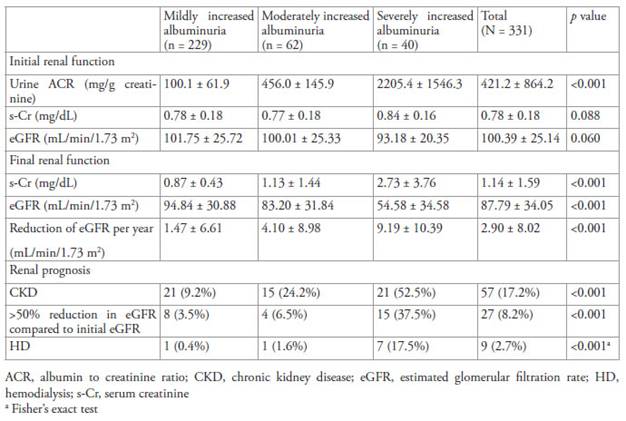
In the whole cohort, the rates of patients with CKD and those with >50% reduction in eGFR from baseline were 17.2% (n=57) and 8.2% (n=27), respectively, and the renal prognosis was poor in the group with high initial urine ACR (p<0.001) (Table 2). HD was performed because of the deterioration of renal function in 2.7% (n=9) of the entire cohort, and the frequency of patients on HD was higher in the group with high initial urine ACR (p<0.001). (Table 2)
The logistic regression analysis to determine risk factors of renal function revealed that PCI (odds ratio [OR] 4.149, 95% confidence interval [CI] 1.496-11.509, p=0.006), PAD (OR 4.788, 95%CI 1.180-19.429, p=0.028), and the degree of albuminuria (OR 4.437, 95% CI 2.564 7.679, p<0.001) were significant risk factors for a >50% reduction in eGFR from baseline.
ACR, albumin to creatinine ratio; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; HD, hemodialysis; s-Cr, serum creatinine a Fisher’s exact test
Cardiovascular and cerebrovascular prognosis Table 2 shows the comparison of the incidence of CVD, heart failure, cerebrovascular disease, and PAD among the three groups. The incidence of CVD tended to be higher in the group with higher
initial urine ACR, with statistically significant difference (p=0.030). However, the incidence of heart failure, cerebrovascular disease, such as stroke and brain hemorrhage, and PAD did not exhibit significant differences among the three groups.
DISCUSSION
Diabetic nephropathy, a renal microvascular complication of DM characterized by albuminuria and progressive loss of kidney function, is a leading cause of ESRD.(1-4, 13) As a marker for kidney/glomerular disease, albuminuria is often the first clinical indicator of DN and is utilized as a clinical tool for predicting prognosis and monitoring therapeutic response.(1, 10) The absence of albuminuria in patients with a reduced eGFR and DM raises the possibility of nondiabetic CKD.1
Concurrent with HTN, which occurs in approximately 65% of patients with DM, hyperglycemia, and genetic predisposition are key factors in the development and progression ofkidney disease.(8, 13) DN is characterized by the development of proteinuria with a subsequent decline in eGFR.(6, 8 n) Although increasing urinary albumin excretion and serum Cr levels accompanied with diminished eGFR are likely important markers of kidney decline, it is unclear whether these biomarkers are independent risk factors for the progression of kidney disease or subsequent outcomes in patients with type 2 DM.(8, 16)
In a study of patients with type 2 DM, Berhane et al. reported that the risk of progression to ESRD was 2.1 fold higher in patients with microalbuminuria and 9.3 fold higher in those with macroalbuminuria, compared to those without albuminuria.17 Conversely, Norris et al. reported that albuminuria, serum Cr, and eGFR were significant factors associated with renal outcomes. 8 In the present study, the rate of reduction in eGFR per year was 1.47 ± 6.61 mL/min/1.73 m2 in the microalbuminuria group and 6.10 ± 9.83 mL/min/1.73 m2 in the macroalbuminuria group, indicating a significant decrease in renal function in patients with macroalbuminuria. Additionally, comparison of the patients according to the severity of macroalbuminuria revealed that the rate of reduction in eGFR per year was significantly higher in those with severe albuminuria (4.10 ± 8.98 mL/min/1.73 m2 in the moderately increased albuminuria group; 9.19 ± 10.39 mL/min/1.73 m2 in the severely increased albuminuria group). Consistent with these results, >50% reduction in eGFR compared to baseline eGFR, CKD, and HD due to the deterioration of renal function were also significantly more frequent in patients with more severe albuminuria.
A study by Yokoyama et al. found that cardiovascular events were more frequent in patients with microalbuminuria and macroalbuminuria compared to those with normal albuminuria and that lower eGFR was associated with higher frequency of cardiovascular events.18 Moreover, a study by Solomon et al. showed that the higher the urine ACR, the greater the cardiovascular death and all-cause mortality.19 In the present study, there was statistically significant difference in the incidence of CVD. However, no statistically significant difference was found in the incidences of heart failure, cerebrovascular disease, and PAD.
In the present study, renal outcomes were compared by classifying the cohort of patients with DN into three groups according to the degree of albuminuria. All patients in the study had a relatively preserved renal function with an initial eGFR >60 mL/min/1.73 m2. The patients with microalbuminuria and those with macroalbuminuria showed significant differences in the rates of progression to CKD, >50% reduction in eGFR compared to baseline, and HD due to deterioration of renal function. Even within the macroalbuminuria group, the severely increased albuminuria group exhibited more severe renal dysfunction compared with the moderately increased albuminuria group. The rate of reduction in eGFR per year was also significantly different depending on the degree of albuminuria.
In agreement with the present study findings, the poor prognosis of renal function in patients with macroalbuminuria compared to those with microalbuminuria has been shown in previous studies.(17, 19-20) In the present study, the prognosis of renal function was worse in patients with severely increased albuminuria (urine ACR >900 mg/g Cr) compared to those with moderately increased albuminuria (urine ACR 300-900 mg/g Cr). There was no significant difference in the prevalence of HTN between the moderately increased albuminuria and the severely increased albuminuria. However, there were significant differences in the rates of progression to CKD (p=0.003), >50% reduction in eGFR compared to baseline (p<0.001), and HD due to deterioration of renal function (p = 0.004). Therefore, faster deterioration of renal function is expected in patients with severely increased albuminuria; therefore, caution is warranted to prevent deterioration of renal function. In previous studies, albuminuria was reported to affect cardiovascular outcomes.(8, 18-19, 21) In the incidence of CVD, there was a significant difference according to the level of albuminuria; however, no significant difference was found in the incidences of heart failure, cerebrovascular disease, and PAD among the groups in the present study.
Several limitations of the present study should be acknowledged. First, this was a single-center study and there were differences in the number of patients among the three groups. As the number of patients was not sufficient, the current study findings should be confirmed in future studies with larger cohorts. Second, DN was not diagnosed by kidney biopsy in most patients, and only 3 (0.9%) patients were diagnosed with DN based on kidney biopsy. Although the DN diagnosis was based on clinical findings, it is known that there are cases in which kidney biopsy is diagnosed as other glomerular disease in approximately 10%-85%,(22'25) and there may be a bias for this. Third, the DN diagnosis was based on the date of first urine ACR test; however, accurate confirmation of the duration of DM and presence ofDN were difficult due to the retrospective study design.21 Fourth, the prevalence rate of HTN and RASi treatment were different between the microalbuminuria and macroalbuminuria groups. HTN and RASi treatment can affect renal prognosis and might have introduced a bias.(6, 26 27) However, there was no significant difference in the prevalence rate of HTN and RASi treatment between the moderately increased albuminuria group and severely increased albuminuria group despite the significant difference in renal prognosis between the moderately increased albuminuria group and severely increased albuminuria group. Finally, whether the patients had HTN and were on RASi treatment could be confirmed; however, it was difficult to confirm the degree of blood pressure control in patients. Therefore, although HTN is a risk factor that can impact renal prognosis,27 there is a limitation that can act as a bias because the efficacy of blood pressure control could not be evaluated.
In conclusion, this retrospective study compared the degree of deterioration in renal function according to the albuminuria level in patients with DN who maintained a relatively preserved renal function with an eGFR >60 mL/min/1.73 m2. Our analyses revealed that the deterioration of renal function was significantly worse in patients with more severe albuminuria. Also, in the incidence of CVD, there was a significant difference according to the albuminuria level. Further investigation with randomized controlled trials and large cohorts is warranted.

