










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Odontológica Latinoamericana
versión On-line ISSN 1852-4834
Acta odontol. latinoam. vol.28 no.2 Buenos Aires ago. 2015
ARTÍCULOS ORIGINALES
Association among salivary flow rate, caries risk and nutritional status in pre-schoolers
Patricia N. Rodríguez1, Josefina Martínez Reinoso1, Carlota A. Gamba1, Pablo A. Salgado2,3, María Teresa Mateo4, María del Carmen Manto4, Susana L. Molgatini4, Verónica Iglesias2, Ángela B. Argentieri2
1 Department of Biochemistry. School of Dentistry. University of Buenos Aires. Argentina.
2 Department of Preventive and Community Dentistry. School of Dentistry. University of Buenos Aires. Argentina.
3 Centre for Population Health Research. Durand Hospital, Argentina.
4 Department of Microbiology, School of Dentistry, University of Buenos Aires, Argentina.
CORRESPONDENCE Dra. Angela Argentieri Facultad de Odontologia. Universidad de Buenos Aires. M. T. de Alvear 2142 CABA - C1122AAH Argentina e-mail: abargentieri@gmail.com
ABSTRACT
Modeer T. et al.(2011) claim that there is association between decreased salivary flow rate and caries in obese adolescents. The aim of this study was to determine the association among nutritional status, salivary flow rate and caries risk in preschoolers. The study comprised 60 children aged 3 to 6 years attending kindergartens in areas immediately adjacent to Buenos Aires City, Argentina. Body weight and height of the children were determined. Body mass index was calculated and the population was classified anthropometrically according to the WHO 2007 (WHO Anthro. Program). Caries risk was determined. Saliva was collected in sterile graduated widemouth containers, without stimulation and without food restrictions. Salivary flow rate (SFR) was determined. Statistical analysis was performed using Pearson's test. It was found that 56.7% (IC95%: 37.7-74.0) of anthropometrically adequate children (Ad) and 37.0% (IC95%: 20.1-57.5) of overweight and obese children (OW/Ob) had caries. The odds ratio for caries (OR=3.78; IC95%: 1.2-11.8, p=0.02) was almost 4 times higher in adequate children than in the others. SFR was 0.534 0.318 ml/min in Ad and 0.439 } 0.234 ml/min in OW/Ob. Pearson's test showed no correlation between SFR and nutritional status (r= 0.004592, p= 0.5977). Although the presence of caries was lower in overweight and obese children, no correlation was found between nutritional status and salivary flow rate.
Key words: Nutritional status; Saliva; Dental caries; Child.
RESUMEN
Relación entre la tasa de flujo salival, riesgo de caries y estado nutricional en niños pre-escolares
Modeer T. et al. (2011) afirman que en las poblaciones de adolescentes obesos existe asociacion entre reduccion de tasa de flujo salival y caries. El objetivo del presente estudio fue determinar la asociacion entre el estado nutricional, la tasa de flujo salival y el riesgo de caries en preescolares. Se estudiaron 60 ninos de 3 a 6 anos de edad, que concurrian a Jardines de Infantes del conurbano de la ciudad de Buenos Aires, Argentina. En este grupo de ninos se midio el peso corporal y la talla. Se calculo el indice de masa corporal y se categorizo antropometricamente a la poblacion segun OMS 2007. (Programa WHO Anthro). Se determino el riesgo de caries. La saliva se recolecto en frascos esteriles, graduados, de boca ancha sin estimulacion y sin restricciones alimentarias. Se determino la tasa de flujo salival (TFS). El analisis estadistico se realizo con el Test de Pearson. Presentaron caries el 56.7% (IC95%: 37.7-74.0) de los ninos adecuados (Ad) antropometricamente y el 37.0% (IC95%: 20.1-57.5) de los ninos con sobrepeso y obesidad (SP/O). El odds ratio para caries (OR=3.78; IC95%: 1.2-11.8, p=0.02) fue casi 4 veces mayor en los ninos Ad, comparados con los SP/O. La TFS fue 0.534 0.318 ml/min en Ad y 0.439 0.234 ml/min en SP/O. El test de Pearson no evidencio correlacion entre la TFS y el estado nutricional (r=0.004592, p=0.5977). A pesar que los ninos con sobrepeso y obesidad tienen menor presencia de caries no se encontro correlacion entre el estado nutricional y tasa de flujo salival.
Palabras Clave: Estado nutricional; Saliva; Caries Dental; Preescolares.
INTRODUCTION
Saliva, modulated by the ecosystem, plays a critical role in the homeostasis of the oral cavity1. Its functions include lubricating the food bolus; protecting against virus, bacteria and fungi; repairing oral mucosa; buffer capacity and remineralizing teeth. It has buffer and neutralizing capacity against acids produced by microorganisms or in the diet, enabling a relatively constant pH to be maintained in bacterial plaque and the oral cavity. It constantly provides calcium and phosphates, which are needed for remineralization processes. Salivary buffer capacity depends on bicarbonate concentration and its remineralization capacity depends on calcium and phosphate concentrations. Both are correlated to the saliva flow rate. Reduced salivary flow rate is a risk factor for caries. Salivary secretion rate, which varies according to the type, strength and duration of the stimulus, is the main factor affecting its composition. Some metabolic disorders, such as those found in obesity, may affect saliva synthesis, composition and secretion2,3. Quantitative and/or qualitative alterations in salivary secretion may lead to the development of infections (candidiasis), functional alterations of masticatory or digestive processes, or infections of the digestive system (halitosis). Whole unstimulated saliva reflects basal salivary flow and is present in the oral cavity for long periods of time (about 14 hours), and is thus the main factor responsible for protective properties, while whole stimulated saliva is present after eating (physiological stimulation), and thus only acts for about two hours4.
During the last quarter of the twentieth century, obesity increased worldwide in all age groups, a situation which has become more visible over the past two decades, with little or no distinction among gender, ethnicity or social condition5-8. Children are not exempt from this problem, and child obesity has increased dramatically in recent decades, becoming a Public Health issue9,10. In Argentina, a study including anthropometric data collected from 2007 to 2012 on a population of 120,000 2- to 18-yearolds, found that 14.5% of preschoolers, 19% of schoolchildren and 17.4% of adolescents were overweight, while obesity affected 9.8% of preschoolers, 17.7% of schoolchildren and 9.9% of adolescents11. These data agree with the latest survey on nutrition and health, conducted in 2007, which showed high prevalence of obesity, which affects 10.5% of children of preschool age12. The association between diseases caused by plaque biofilm and nutritional status has been studied by different authors, with contradictory results13-16. Adipocytes secrete various hormones and cytokines which contribute to obesity. Leptin acts on hypothalamus receptors to suppress food intake and increase energy consumption. A reduction in the sensitivity of the receptors of this hormone can induce the beginning of obesity and affect salivary secretion. This led to obesity being linked to hiposalivation and related pathologies such as dental caries3. Overweight or obese children have alterations in the concentration of phosphates, sialic acid, proteins and peroxidase activity, leading to conditions which are favorable to the development of caries2.
Obesity, in particular abdominal obesity, usually accompanied by metabolic syndrome, is linked to chronic inflammation and therefore to higher risk of diseases such as type 2 diabetes, atherosclerosis, respiratory disorders and periodontal disease14-16. Being socially at risk plays a critical part in the etiopathology of obesity and caries because it facilitates synergic interaction among risk factors. Children growing up in urban settings adopt behavior traits that facilitate the progression of the disease. This explains why urbanization and modernization rates are strongly linked to the predominance of obesity17. In addition, dental caries and obesity both have multifactorial etiology and are associated to eating habits. The prevalence of caries and obesity is a growing challenge for Public Health authorities. Many studies on these pathologies have produced controversial results, possibly due to the lack of standardized criteria for diagnosis, and the different age groups and designs used in the different papers. The aim of this study was to determine association among nutritional status, saliva flow rate and caries risk in preschoolers.
MATERIALS AND METHODS
This was a descriptive, correlational study, perfor - med at government-run kindergartens in areas immediately adjacent to Buenos Aires city. The protocol was approved by the Ethics Committee at the School of Dentistry at Buenos Aires University (11/05/2011- no 07).
Phase 1: Preliminary activities
Parents or guardians received information on the study, following current ethical standards. They provided authorization by signing informed consent for children to be included in the study and information about the children's medical and dental history. Then they attended a meeting during which information was provided about frequent diseases of the oral cavity and advice on oral hygiene and ad hoc dietary recommendations.
Phase 2: Sampling
Exclusion criteria were: a) Children with systemic diseases, b) Children having received radiation, or c) Children taking any medication at the time of sampling which would modify the saliva flow rate. All authorized children were evaluated, diagnosed included in a preventive care program, regardless of the exclusion criteria. The purposive sample included 60 children (30 female and 30 male), aged 3 to 6 years old (mean SD= 58.8 10.7 months).
Phase 3: Collecting anthropometric clinical data
Anthropometric data were taken using the measuring techniques suggested by the Growth and Development Committee of the Argentine Pediatric Association18, by a single professional, at the same time, and after the children had had breakfast and emptied their bladder. Data were collected and processed as follows:
• Body weight recorded on a CAM brand scale to the nearest 100 g, wearing light clothes;
• Height measured with a CAM brand stadiometer to the nearest 1 mm.
• Body mass index (BMI) calculated as weight (kg)/ height2 (m2).
• Anthropometric classification of the children in the sample using the BMI Z scores corresponding to the WHO standards, by applying the WHO software AnthroPlus19,20. The following zBMI cutoff points were used: underweight ≤ -1 SD, adequate -1.0 to +1.0 SD, overweight ≥ +1.0 y < +2.0 SD, obesity ≥ +2.0 SD21.
Phase 3: Saliva collection and analysis
Unstimulated saliva without food restriction was collected in wide-mouthed, graduated, sterile jars. Spontaneous salivary flow rate was determined (SFR) 22.
Phase 4: Determining history of dental caries and cariogenic risk factors
Clinical examinations were performed by a single professional following validated criteria. The following were calculated:
• dmft index23
• dental plaque biofilm index24
• diet history
Phase 5: Statistical analysis
The data were analyzed using the following statistical analyses:
• Distribution and frequency of study variables (salivary flow rate, presence of caries and nutritional status) and/or percentages in relation to total cases and their respective 95% confidence intervals, using Fisher's exact probability test for significance, with p<0,005 considered statistically significant difference.
• We expressed SFR as mean standard deviation (SD), and analyzed normality assumptions (Kolmogorov & Smirnov test) and homoscedasticity (Bartlett's test). The results were considered significant at a 5% probability level.
• Mann-Whitney's test was applied for comparisons between sexes.
• Pearson's test was used to determine the correlation between SFR and nutritional status and age. We used the software GraphPad Prism, version 5.03 (GraphPad Software, Inc., San Diego, CA, USA).
RESULTS
Results of studies on anthropometric data
Fifty percent of the children in the study had adequate or normal weight, 23.3% were overweight and 21.7% were obese. Because there were very few underweight children (5%) according to zBMI, they were excluded from the sample. Fig. 1 shows the distribution of the sample according to nutritional status evaluated through the Z score of Body Mass Index (BMI).
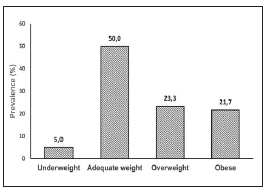
Fig. 1: Distribution of the population according to nutritional status.
Results of studies on teeth
Results for association between anthropometric data and dental status
56.7% (CI 95%: 37.7-74.0) of anthropomorphically adequate children and 37.0% (CI 95%: 20.1-57.5) of overweight and obese children had caries. The odds of having caries (Odds Ratio= 3.78; CI 95%: 1.2- 11.8, p=0.02) was nearly 4 times higher in anthropomorphically adequate children (Fig. 2).
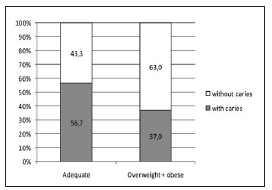
Fig. 2: Presence of caries according to nutritional status.
Results for association between SFR and anthropometric data
SFR was 0.534 } 0.318 ml/min for anthropometrically adequate children and 0.439 } 0.234 ml/min for overweight and obese children, with no statistically significant difference. Pearson's test showed no correlation between SFR and nutritional status (r= 0.004592, p= 0.5977) (Fig. 3).
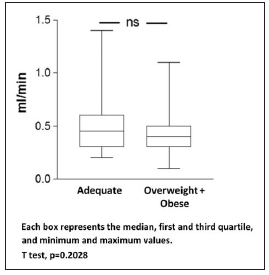
Fig. 3: Salivary flow according to nutritional status.
Results for association between SFR and gender
When salivary flow rate was analyzed with relation to gender in the study population, girls were found to have higher SFR than boys (mean } SD= 0.57} 0.29 vs. 0.40}0.27) (Fig. 4).

Fig. 4: Salivary flow rate according to sex.
Results for association among SFR, gender and anthropometric data
When the population was analyzed according to salivary flow rate, gender and anthropometric data, overweight and obese girls were found to have higher salivary flow rate than boys (Table 1).
Table 1: Salivary flow rate according to gender and nutritional status.

Results for association between SFR and caries
Both adequate and obese children with caries have higher SFR, although it is only statistically significant in those with adequate weight (0.59 } 0.30 ml/min vs. 0.37 } 0.20 ml/min, mean and SD), p=0.0017 (Table 2).
Table 2: Association among salivary flow rate, nutritional status and caries.

DISCUSSION
There are multiple factors involved in the etiology of dental caries, so the risk analysis should include factors involved in its development, including lifestyle25. Weight gain is the result of a positive energy balance, with intake exceeding expenditure26 due to the intake of food with high caloric density27 and a low level of physical activity28. In the "obesogenic environment" of society today, eating habits and sedentary behavior are the main components influencing obesity. Diet quality as a cause of obesity has been the object of many studies in adults, but few in children. The Bogalusa Heart Study found positive association between the prevalence of obesity and the consumption of beverages and salty snacks but not the consumption of desserts and candies29. Al-Zahrani et al.15 suggest that obesity in childhood and youth predisposes to oral disease. Other authors found contradictory results (Table 3): some found significant association between obesity and dental caries30, while others found that obese children had higher risk of erosion but not necessarily of caries, compared to children of normal weight31. Alm et al.32 found that overweight and obese adolescents had a higher number of proximal caries than those of normal weight, and this finding was associated to higher consumption of snacks since childhood. These findings do not agree with reports by Yen et al.33.
Table 3: Summary of literature found about the association between obesity and caries and salivary flow rate.

Meta-analysis of the association between obesity and dental caries in populations of recently industrialized countries vs. industrialized countries found a significant association between the two conditions in the latter34. Gupta et al.35 found no significant association between presence of caries and body mass index in 12-year-old children, but did find a strong correlation with oral hygiene. Kopycka-Kedzierawski et al.36 found in a population of 6- to 11-year-old children that obese children were less likely to have caries, in agreement with the findings in our study. Fadel37 found that obese adolescents had lower stimulated saliva secretion, higher concentration of secretory IgA (p<0.001), and greater presence of dental caries and gingivitis (p<0.01), with no significant difference in snack consumption and bacterial plaque index. Powers et al.38 found no difference in salivation patterns between obese and non-obese adults. In a cohort of obese adult patients, Flink39 has shown that there is an association between reduction in stimulated salivary flow rate and increased body mass index.
This observation does not agree with the findings of our study, where saliva was not stimulated for collection. Modeer et al.40 conducted a cross-sectional study and found lower stimulated salivary flow rate in obese adolescents. This may be attributed to the fact that salivary secretion neuro-endocrinal regulation may be affected due to the altered ratio in abdominal obesity due to the modulation of the immune system, via cytokines, exercised by the central nervous system41. Fenoll42 suggests that salivary flow is lower in females because they may have smaller salivary glands. However, this does not agree with the findings in our study, where salivary flow was significantly higher in females. Johansson43 found that stimulated salivary flow declined with malnutrition, while unstimulated saliva did not change. It could be inferred that nutritional status has an influence on changes in salivary flow and thus on oral ecology. In the presence of food, the body's first reaction corresponds to the cephalic phase, which includes increased heart rate, body temperature, gastric activity and salivary flow. Faced with repeated food cues, the individual becomes habituated and learns to ignore them. It has been observed that this behavior is much slower in obese persons, i.e., they continue to have an increased salivary response in the presence of food44, with a higher rate of salivary flow. It would be worth conducting studies on food consumption to identify what variables might condition these results.
CONCLUSIONS
1) There was no correlation between overweight/ obesity and salivary flow rate.
2) Obese children had fewer teeth affected by dental caries.
Both diseases - caries and obesity/overweight - have common causes which require integrated management by multidisciplinary teams promoting healthy diets.
ACKNOLWEDGMENTS
This work was supported by a grant from the University of Buenos Aires. UBACyT Program n° 20720130100017BA.
1. Carpenter GH. The secretion, components, and properties of saliva. Annu Rev Food Sci Technol 2013; 4:267-276. [ Links ]
2. Pannunzio E, Amancio OM, Vitalle MS, Souza DN, Mendes FM, Nicolau J. Analysis of the stimulated whole saliva in overweight and obese school children. Rev Assoc Med Bras 2010; 56:32-36. [ Links ]
3. Ueda H, Yagi T, Amitani H, Asakawa A, Ikeda S, Miyawaki S, Inui A. The roles of salivary secretion, brain-gut peptides, and oral hygiene in obesity. Obes Res ClinPract 2013; 7:e321-329. [ Links ]
4. Sreebny LM. Saliva in health and disease: in appraisal and update. Int Dent J 2000; 50: 140-161. [ Links ]
5. Ogden CL, Fryar CD, Carroll MD, Flegal KM. Mean body weight, height, and body mass index, United States 1960- 2002.Adv Data; 2004:1-17. [ Links ]
6. Flodmark CE, Marcus C, Britton M. Interventions to prevent obesity in children and adolescents: a systematic literature review. Int J Obes (Lond) 2006; 30:579-589. [ Links ]
7. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014; 311:806-814. [ Links ]
8. Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet 2010; 375(9727):1737-1748. Review. [ Links ]
9. Karnik S, Kanekar A. Childhood obesity: a global public health crisis. Int J Prev Med 2012; 3:1-7. [ Links ]
10. de Onis M, Blossner M, Borghin E. Global prevalence and trends of overweight and obesity among preschool children. Am J ClinNutr 2010; 92:1257-1264. [ Links ]
11. Hacia el mapa de la obesidad en Argentina. URL: http://www.cesni.org.ar/Content/pres.mapa12.pdf [ Links ]
12. Encuesta Nacional de Nutricion y Salud (ENNyS). Documentos de resultados. Ano 2007. Ministerio de Salud. Presidencia de la Nacion. Argentina. URL: http://www.msal.gov.ar/images/stories/bes/graficos/0000000257cnt-a08-ennysdocumento-de-resultados-2007.pdf [ Links ]
13. Kantovitz KR, Pascon FM, Rontani RM, Gaviao MB. Obesity and dental caries - A systematic review. Oral Health Prev Dent 2006; 4:137-144. [ Links ]
14. Baker JL, Olsen LW, Sorensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med 2007; 357:2329-2337. [ Links ]
15. Al-Zahrani MS, Bissada NF, Borawskit EA. Obesity and periodontal disease in young, middle-aged, and older adults. J Periodontol 2003; 74:610-615. [ Links ]
16. Modeer T, Blomberg C, Wondimu B, Lindberg TY, Marcus C. Association between obesity and periodontal risk indicators in adolescents. Int J Pediatr Obes 2011; 6:e 264-270. [ Links ]
17. Candib LM. Obesity and diabetes in vulnerable populations: reflection on proximal and distal causes. Ann FamMed 2007; 5:547-556. [ Links ]
18. Guias para la evaluacion del crecimiento fisico. Sociedad Argentina de Pediatria; Comite Nacional de Crecimiento y Desarrollo Buenos Aires (Argentina): 2013. URL: Links ]sap.org.ar/docs/publicaciones/libro_verde_sap_2013.pdf" target="_blank">http//www.sap.org.ar/docs/publicaciones/libro_verde_sap_2013.pdf
19. Software for assessing growth and development of the world's children. WHO Anthro for personal computers, version 3.2.2, 2011: Geneva: WHO, 2010. URL : http://www.who.int/childgrowth/software/en/ [ Links ]
20. Onyango AW, de Onis M, Caroli M, Shah U, Sguassero Y, Redondo N, Carroli B. Field-testing the WHO child growth standards in four countries. J Nutr 2007; 137:149-152. [ Links ]
21. Sguassero Y, Moyano C, Aronna A, Fain H Orellano A, Carroli B. Validacion clinica de los nuevos estandares de crecimiento de la OMS: analisis de los resultados antropometricos en ninos de 0 a 5 anos de la ciudad de Rosario, Argentina. Arch Argent Pediatr 2008; 106:198-204. [ Links ]
22. Dawes C. Factors Influencing Salivary Flow Rate and Composition. In: Edgar WM and O'Mullane DM, editors. London. England Saliva and Oral Health. 4o ed. 2013. [ Links ]
23. Klein H, Palmer C.E, Knutson J.W. Studies on dental caries index,dental status and dental needs of elementary school children, Public Health Report (Wsh) 1988; 53:751-765. [ Links ]
24. Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 1964; 22:121-135. [ Links ]
25. Bordoni NE. Plan de atencion integral de la salud bucal en ninos y adolescentes. In Odontologia pediatrica. La salud bucal del nino y el adolescente en el mundo actual. Bordoni N, Escobar Rojas A, Castillo Mercado R. Buenos Aires, Argentina. Ed. Medica Panamericana 2010: 103-122
26. Keast DR, Fulgoni VL 3rd, Nicklas TA, O'Neil CE. Food sources of energy and nutrients among children in the United States: National Health and Nutrition Examination Survey 2003-2006. Nutrients 2013; 5:283-301. [ Links ]
27. Nicklas TA, Yang SJ, Baranowski T, Zakeri I, Berenson G. Eating patterns and obesity in children. The Bogalusa Heart Study. Am J Prev Med 2003; 25:9-16. [ Links ]
28. Gubbels JS, van Assema P, Kremers SP. Physical Activity, Sedentary Behavior, and Dietary Patterns among Children. Curr Nutr Rep 2013; 2:105-112. [ Links ]
29. O'Neil CE, Nicklas TA, Liu Y, Berenson GS. Candy consumption in childhood is not predictive of weight, adiposity measures or cardiovascular risk factors in young adults: the Bogalusa Heart Study. J Hum Nutr Diet 2015; 28 (Suppl. 2): 59-69. [ Links ]
30. Bailleul-Forestier I, Lopes K, Souames M, Azoguy-Levy S, Frelut ML, Boy-Lefevre ML. Caries experience in a severely obese adolescent population. Int J Paediatr Dent 2007; 17:358-363. [ Links ]
31. Tong HJ, Rudolf MC, Muyombwe T, Duggal MS, Balmer R. An investigation into the dental health of children with obesity: an analysis of dental erosion and caries status. Eur Arch Paediatr Dent. 2014; 15:203-210. [ Links ]
32. Alm A, Fahraeus C, Wendt LK, Koch G, Andersson-Gare B, Birkhed D. Body adiposity status in teenagers and snacking habits in early childhood in relation to approximal caries at 15 years of age. Int J Paediatr Dent 2008; 18:189-196. [ Links ]
33. Yen CE, Hu SW. Association between dental caries and obesity in preschool children. Eur J Paediatr Dent 2013; 14: 185-189. [ Links ]
34. Hayden C, Bowler JO, Chambers S, Freeman R, Humphris G, Richards D, Cecil JE. Obesity and dental caries in children: a systematic review and meta-analysis. Community Dent Oral Epidemiol 2013;41:289-308. [ Links ]
35. Gupta P, Gupta N, Singh HP. Prevalence of Dental Caries in relation to Body Mass Index, Daily Sugar Intake, and Oral Hygiene Status in 12-Year-Old School Children in Mathura City: A Pilot Study.Int J Pediatr 2014; 2014:ID 921823. [ Links ]
36. Kopycka-Kedzierawski DT, Auinger P, Billings RJ, Weitzman M. Caries status and overweight in 2- to 18-yearold US children: Findings from national surveys. Community Dentistry and Oral Epidemiology 2008; 36 : 157-167. [ Links ]
37. Fadel HT, Pliaki A, Gronowitz E, Marild S, Ramberg P, Dahlen G, Yucel-Lindberg T, Heijl L, Birkhed D. Clinical and biological indicators of dental caries and periodontal disease in adolescents with or without obesity. Clin Oral Investig 2014; 18:359-368. [ Links ]
38. Powers PS, Holland P, Miller C, Powers HP. Salivation patterns of obese and normal subjects. Int J Obes 1982; 6: 267-270. [ Links ]
39. Flink H, Bergdahl M, Tegelberg A, Rosenblad A, Lagerlof F. Prevalence of hyposalivation in relation to general health, body mass index and remaining teeth in different age groups of adults. Community Dent Oral Epidemiol 2008; 36:523-531. [ Links ]
40. Modeer T, Blomberg CC, Wondimu B, Julihn A, Marcus C. Association between obesity, flow rate of whole saliva, and dental caries in adolescents. Obesity (Silver Spring) 2010;18:2367-2373. [ Links ]
41. Pasquali R, Vicennati V, Cacciari M, Pagotto U. The hypothalamic- pituitary-adrenal axis activity in obesity and the metabolic syndrome. Ann N Y Acad Sci 2006; 1083: 111-128. [ Links ]
42. Fenoll-Palomares C, Munoz Montagud JV, Sanchiz V, Herreros B, Hernandez V, Minguez M, Benages A. Unstimulated salivary flow rate, pH and buffer capacity of saliva in healthy volunteers. Rev Esp Enferm Dig 2004; 96: 773-783. [ Links ]
43. Johansson I, Saellstrom AK, Rajan BP, Parameswaran A. Salivary flow and dental caries in Indian children suffering from chronic malnutrition. Caries Res 1992; 26:38-43. [ Links ]
44. Aspen VA, Stein RI, Wilfley DE. An exploration of salivation patterns in normal weight and obese children. Appetite 2012; 58:539-542. [ Links ]

