











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Dentin hypersensitivity (DH) is an important clinical problem. It can be defined as an acute pain of short duration resulting from the exposure of dentin to thermal, evaporative, tactile, osmotic or chemical stimulation. It cannot be attributed to any other oral disease. DH is a common problem in many adult populations. Estimates of its occurrence are highly variable and range from less than 10% to more than 50% of the population1-5. Such disparity in the occurrence rate of DH may be related to the target populations, the methods used to measure it, and lack of representativeness in most studies.
The condition tends to be most evident in patients aged 20-40 years, and occurs about equally in males and females. It may affect any tooth, though the most common (50%) are canines and first premolars. It occurs most frequently (95%) on buccal surfaces at the cervical margin4. The most widely accepted explanation of its cause is the hydrodynamic theory, which states that after an external stimulation on the exposed root surface, the fluid inside dentinal tubules moves, stimulating dental pulp neural fibers and causing pain1.
It is well known that all kinds of pain ultimately affect quality of life, and DH is no exception. DH is considered chronic pain, since it is present practically all the time. People who suffer from DH are known to have worse oral health-related quality of life (OHRQoL)5-7, which directly influences overall health, especially in adolescents. Representative studies assessing the occurrence of DH are not available from most countries, though there are studies on adults from China, India and, more recently, Brazil8. Costa et8 reported the occurrence of DH in a representative sample of adults and elderly people in Brazil, with prevalence higher than 30%. DH was associated with gender, age, smoking, gingival recession and periodontal therapy.
However, no representative studies have reported the occurrence of DH in adolescents. It is important to emphasize that during adolescence, some of the reported associated factors might not have acted for long enough, with other factors potentially being responsible in the etiological chain. It is essential to know the prevalence of DH and its associated factors in order to establish strategies for its adequate prevention and control. The aim of this study is to determine the occurrence of self-reported dentin hypersensitivity and its risk indicators in adolescents from southern Brazil.
MATERIALS AND METHODS
Study design and target population
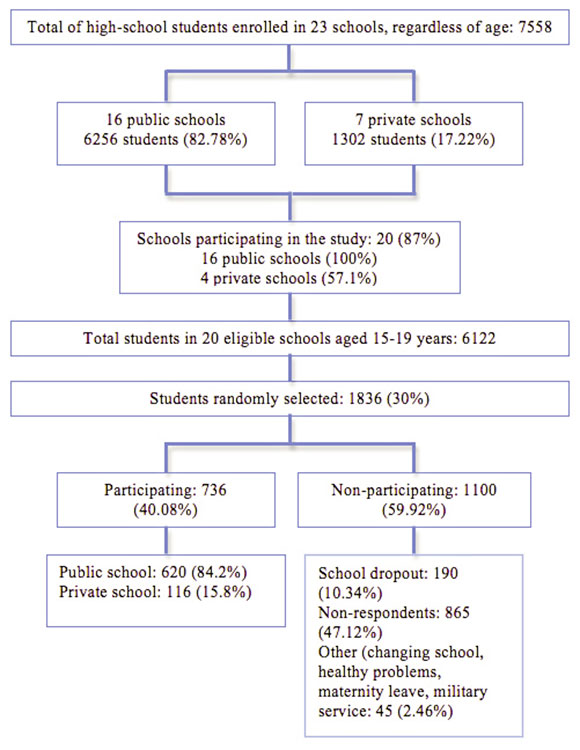
The present study is a cross-sectional observational survey, carried out in the city of Passo Fundo, located in the south of Brazil. The target population for the study comprised adolescents aged 16-19 years, enrolled at public or private high schools in the city in 2012. Passo Fundo has a population of about 190,000, and is considered to be a mediumsized city9. In 2012, there were a total 23 high schools, including 7 private and 16 public, and a total 7,558 students enrolled, of whom 6,256 (82.78%) attended public schools and 1,302 (17.22%) attended private schools.
Ethical Aspects
The study was approved by The Institutional Review Board of the University of Passo Fundo (protocol 066/2012), and all selected students provided informed consent signed by parents or guardian.
Sampling strategy
The study coordinator visited and invited all high schools to participate in the survey, of which 20 (87%) agreed to participate. The student population was 6,122. It was arbitrarily determined that 30% of the students from each school would comprise the study sample. These students were randomly selected by draw from the lists of students enrolled at each school.
After the selection, the research team visited the classrooms to explain the study and its objectives. In case of absence of the selected individual, an extra contact was made.
Interview and clinical examinations
Students were interviewed and examined by a trained team. A structured questionnaire, including demographic information, socioeconomic data, history of dental bleaching, orthodontic treatment, and oral hygiene habits was applied to all respondents. DH was assessed through the answers to the question: "Do you have tooth sensitivity?" indicated by selecting an option on a Likert scale (never, rarely, sometimes, fairly often and always). These answer options were constantly visually available on a card.
Clinical examination to determine the number of present teeth (excluding third molars) was performed after the interview with the aid of a wooden spatula, under standard room illumination. Teeth that could be rehabilitated in some way were considered present in the count. Teeth or roots suitable for extraction were considered absent. Training was conducted among team members and with non-selected students, using the field conditions.
Statistical analysis
Occurrence of DH, the primary outcome of this study, was analyzed as a dichotomous variable. Respondents were categorized as having DH if they answered farly often or always to the question applied in the questionnaire.
Independent variables included age, gender, skin color, use of dental floss, private/public school, smoking, past and current orthodontic treatment, tooth bleaching and number of present teeth. Age was analyzed using three categories (15, 16, and >17 years of age). Skin color was dichotomized into white or non-white (black, yellow, brown or indigenous). Self-reported use of dental floss was analyzed as a dichotomous variable (yes/no). Smoking habit was defined using two groups: adolescents without any history of smoking and adolescents who were either current or former smokers at the time of the interview. Orthodontic treatment was dichotomized into never and past/ current treatment. Respondents were divided into those that reported having undergone any type of tooth bleaching (toothpaste, dental office or home-bleaching) and those that had never been exposed. They were classified according to whether they attended private or public schools, as a proxy for socioeconomic status. Number of present teeth was dichotomized into 28 and less than 28 teeth. Univariable associations between occurrence of DH and other variables were assessed by either the chi-square test or Fisher's exact test when appropriate. Binary logistic regression models were fitted to assess risk indicators for DH. Models were built using a purposeful selection of variables10. Univariable regression models were fitted and all variables with p-values <0.25 were included in a multivariable model. Variables that did not significantly contribute to the multivariable model (p>0.05) were assessed for confounding before being eliminated. Confounding was defined as a >20% change on other variable coefficients. Odds ratios (OR) and 95% confidence intervals (95%CI) were reported.
The significance level was set at 5%. Data analyses were performed using statistical package Stata 10 for Macintosh (STATA, College Station, TX, USA).
RESULTS
A total 1,836 students were randomly selected and invited to participate in the study, of whom 736 accepted, yielding a response rate of 40.1%. Of these, 323 (43.9%) were male and 413 (56.1%) were female. Non-participation in the study was due to either not signing the consent form, school dropout of selected individuals or non-acceptance. Of the 736 participants, 620 (84.2%) were from public schools and 116 (15.8%) from private schools (Fig. 1).
Reproducibility of the clinical examination was conducted in 10% of the examined individuals, randomly selected, revealing an agreement rate of 98%, which implies adequate reproducibility of the method for counting present teeth.
Table 1 presents the characteristics of the study sample. Data parallel the distribution of demographics in the schools and in the city, including the 84.2% of adolescents enrolled in public schools. Most of the students had never smoked, had not undergone or were not undergoing orthodontic treatment and had not undergone tooth bleaching procedures. Approximately half the students reported using dental floss and the majority (approximately 80%) had 28 teeth.
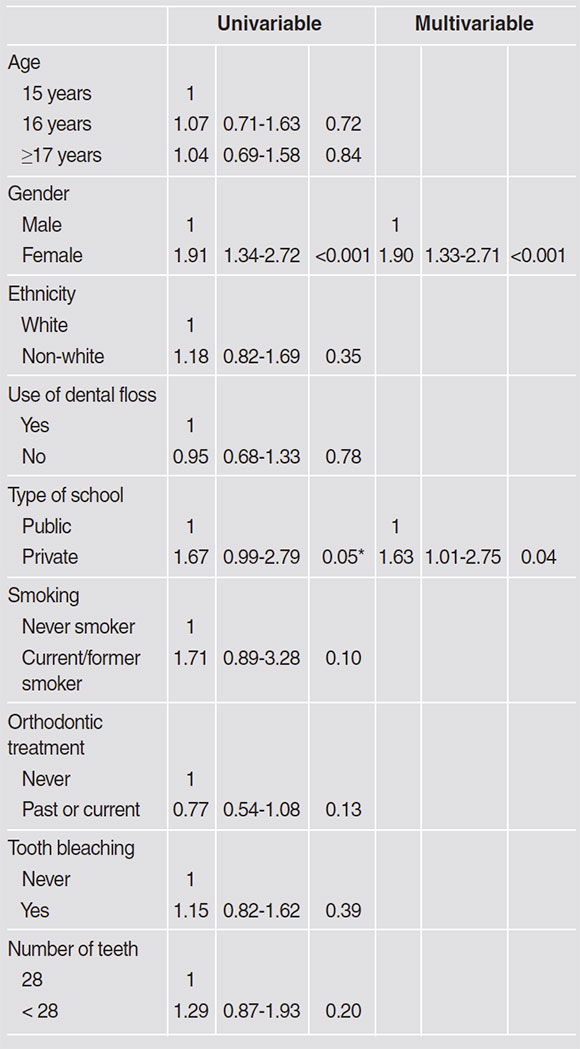
Table 3 shows the univariable and multivariable logistic regression models. In the univariable models, gender was significantly associated with the occurrence of DH. In the final multivariable model, gender and type of school had statistically significant association. Females showed a significantly greater chance of having sensitivity than males (OR=1.90 95%CI 1.33-2.71), and attending public schools increased the chance of sensitive teeth by 63% compared to students from private schools (OR=1.63 95%CI 1.01-2.75).
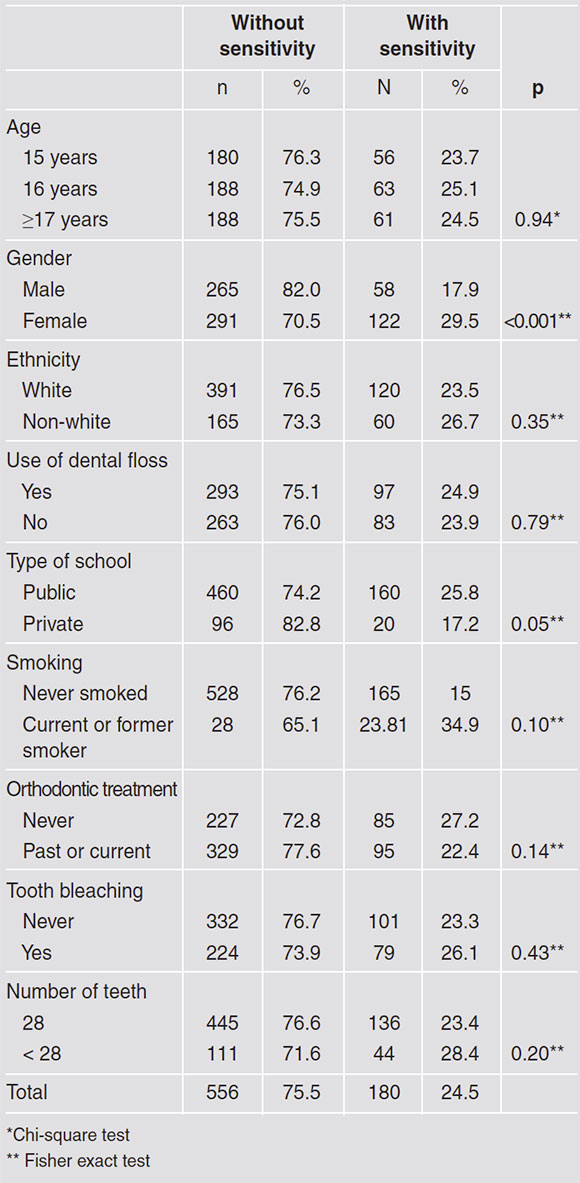
Table 2 presents the occurrence of DH and its association with independent variables. Overall, 556 (75.5%) subjects reported sensitive teeth never, rarely or sometimes, while 180 (24.5%) reported having sensitive teeth often or always. Of all risk indicators assessed, gender was significantly associated to greater dentin hypersensitivity occurrence in females. Students from public schools tended to present higher occurrence of DH.

DISCUSSION
The aim of present study was to assess the occurrence and risk indicators of DH in Brazilian adolescents. Epidemiological studies that assess prevalence of DH are extremely heterogeneous, so the methodology used in each of them needs to be taken into account in order to understand the estimates. The uniqueness of the present study is that it assesses the condition in adolescents. To the best of our knowledge, there are few studies on prevalence of DH in adolescents. The only study conducted with adolescents found a prevalence of 19%, but it was conducted in Piaui, where the climate and socioeconomic situation differ from those in Rio Grande do Sul11.
The study was performed in a medium-sized city in southern Brazil. All the schools in the city were invited to participate, and 86% of them agreed to do so. In these schools, 30% of the enrolled students were randomly selected to be invited to participate in the survey, of whom 40% accepted. The response rate is similar to that found in other epidemiological studies in the literature12. Non-participants did not differ from participants in terms of demographic and socioeconomic characteristics and the reasons for non-participation were related to school dropout or parents/guardians not signing the informed consent. These reasons are relatively common in studies with adolescents13. Considering that the percentages of participants in terms of gender and type of school resemble the percentages of students in the city, some degree of representativeness can be claimed in the present study.
DH was assessed by means of self-report. There is ongoing profound discussion about the strengths and limitations of using self-reported pain in different studies. There is no doubt that self-reported pain is a true outcome variable1 that has to be understood differently from surrogates. Even though there is some degree of subjectivity involved in assessing self-reported pain, there is no uncertainty that it is considered impacting by the study volunteer. Studies with DH have been performed worldwide and used different measurements. Air stimulation, probing and self-reported DH are the most commonly used outcomes in published studies14 16. Falta la referencia 15. Studies that use self-reported DH and another type of stimulation in the assessment of DH suggest that self-reported DH tends to overestimate the occurrence of the disease17, 18.
The present study shows occurrence of DH in 25% of high school adolescents, i.e., 1 out of 4, 15 to 19-year-olds. The answers "fairly often" or "always" on the Likert scale were considered to indicate presence of DH. This cutoff point infers more impact and has been widely used in the literature10. In terms of prevalence of different diseases/ conditions, 25% is considered a relatively high occurrence3, 20.Falta referencia 19 In the same state in Brazil, Costa et al. (2014)8 recently analyzed the prevalence of DH in adults and the elderly by means of an air blast and probing, reporting estimates of 33% and 34%, respectively. Considering that the region of the country is the same and that gingival recession increases with age21,7, the figures reported in the present study are probably not overestimated. It should also be noted that there is a cycle in DH, related to biological factors. Even though gingival recession increases with age, dentin also forms over the years. A study by Costa et al. found that the elderly tend to present lower estimates of DH than do younger adults8.This should be taken into account when analyzing data from adolescents. Although gingival recession in adolescents may not be as extensive as in adults, nevertheless the pulp chamber is larger, and therefore closer to external stimulation22.
In addition to determining prevalence, it is important to understand the associated factors that can be considered risk indicators for DH. The present study conducted univariable and multivariable analyses to assess which factor(s) may be associated to selfreported DH in adolescents. Age, ethnicity, oral hygiene habits, smoking, orthodontic and bleaching experiences were not associated to DH in the present study. Although these variables have been shown to be risk indicators for DH in different studies20, 22-25,it should be highlighted that the age range in this survey is 15-19 years, a relatively short period of the lifespan. In addition, the low occurrence of some of the possible risk indicators -smoking, dental treatment and tooth loss - might have contributed to the lack of association. These variables were not associated with DH in this age range. It should be kept in mind that the information in the literature from other age ranges should not be dismissed, and that these adolescents will grow older, exposed to these risk indicators, which could lead to an increase in DH.
The results of the present study showed that female gender and studying in public schools are associated with DH. Other studies with different populations have also reported higher rates in women. There are various possible explanations for this. All kinds of self-perceptions have greater impact in women than in men20, 26. In addition, women present both higher quality of oral hygiene and more gingival recession. This leads to higher chances of DH among females. A study by Costa et al. sh owed an odds ratio of more than 2 for female:male adults for DH8. In the present study, females had a 90% greater chance of reporting DH than males. This will probably increase over time. Especially in adolescence, there is an opportunity for informing females of these chances in order to limit the consequences of DH.
The type of school that the adolescent attended was also associated with higher chances of DH. Studying in a public school increases the chances of reporting DH by 67%. Although this was a borderline significance, it should not be disregarded as an opportunity for implementing preventive strategies. In the context of this study, the type of school and ethnicity were used as a proxy of socioeconomic status27. Skin color was not associated with DH. One of the reasons for this is the low percentage of non-whites in the study. However, students from public schools tended to present higher degrees of self-reported DH. Other studies that assessed gingival recession found higher occurrence in subjects from lower socioeconomic levels. This should be taken into account to focus on educational strategies at public schools, where students could benefit.
The strengths and limitations of this study should be highlighted. In terms of strengths, studying the epidemiology of DH in adolescents is important in view of the lack of literature on the subject and the opportunity it provides for creating preventive strategies. Moreover, the representativeness of the study increases its external validity, providing information on disease occurrence, which is limited in non-representative studies. One of the possible limitations of the study is the lack of a second DH measurement, which could increase the internal validity of the study -probably confirming the selfreported outcomes-, and might enable the extension of DH to be determined, providing interesting information. The present study, understanding its methods, shows that DH is a condition that impacts subjects as from adolescence, so the opportunity to apply preventive strategies as from this age should not be missed.
DH has direct impact on both oral and systemic health, affecting quality of life. It is important for adolescents to learn health-related attitudes and behaviors that will last through adulthood28. One of the World Health Organization (WHO) strategies to improve oral health for the twenty-first century, in addition to the effective use of fluoride and a healthier diet, is to improve oral health for children and adolescents through health promotion in schools29. Because adolescents are establishing their independence from the influence of their parents in relation to various aspects of their development30, they are a challenging group in terms of oral health. The vulnerability of their permanent teeth often exposes them to major chronic oral diseases, such as caries and periodontal diseases, with early onset and progressive, cumulative effect, manifesting in childhood, adolescence and in all age groups of adult life31.
In conclusion, DH is a prevalent condition in adolescence. It is associated with female gender and lower socioeconomic status. Preventive strategies for DH need to begin in adolescence; taking into consideration these risk indicators.

